Hey I was on rounds in the post ctvs surgical icu and my consultants was discussing some post op gradient,rv and lv hyperdynamic,what was it,also tell me about the basic pathophysiology of icr then what are the surgical steps and how to manage post icr patient in ICU
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Searching the Web
ICR intracardiac repair TOF post-op ICU management residual gradient RV hyperdynamic
Reading Web Page
https://www.frontiersin.org/journals/pediatrics/articles/10.…
Reading File
Loading Image
I now have comprehensive information. Let me compile the full answer.
ICR (Intracardiac Repair) - Complete Overview for the CTVS ICU
What Was Your Consultant Discussing?
The post-op gradient + RV/LV hyperdynamic state your consultant mentioned almost certainly refers to the residual RV-to-PA pressure gradient measured on echo after ICR (intracardiac repair) for Tetralogy of Fallot (TOF). Specifically:
- A residual RVOT gradient (measured by CW Doppler, modified Bernoulli: 4v²) that persists after VSD patch closure and infundibular resection
- Both ventricles can appear hyperdynamic in the immediate post-op period - the RV because it is still hypertrophied but now decompressed (afterload suddenly dropped), and the LV because it now receives full pulmonary venous return that was previously bypassed through the right-to-left shunt
- This hyperdynamic state is actually expected and reassuring in the first 24-48 hours if there are no residual lesions and cardiac output is adequate
1. Basic Pathophysiology of ICR (TOF)
ICR = Intracardiac Repair is the definitive surgical correction for Tetralogy of Fallot. Understanding the pre-repair physiology is key:
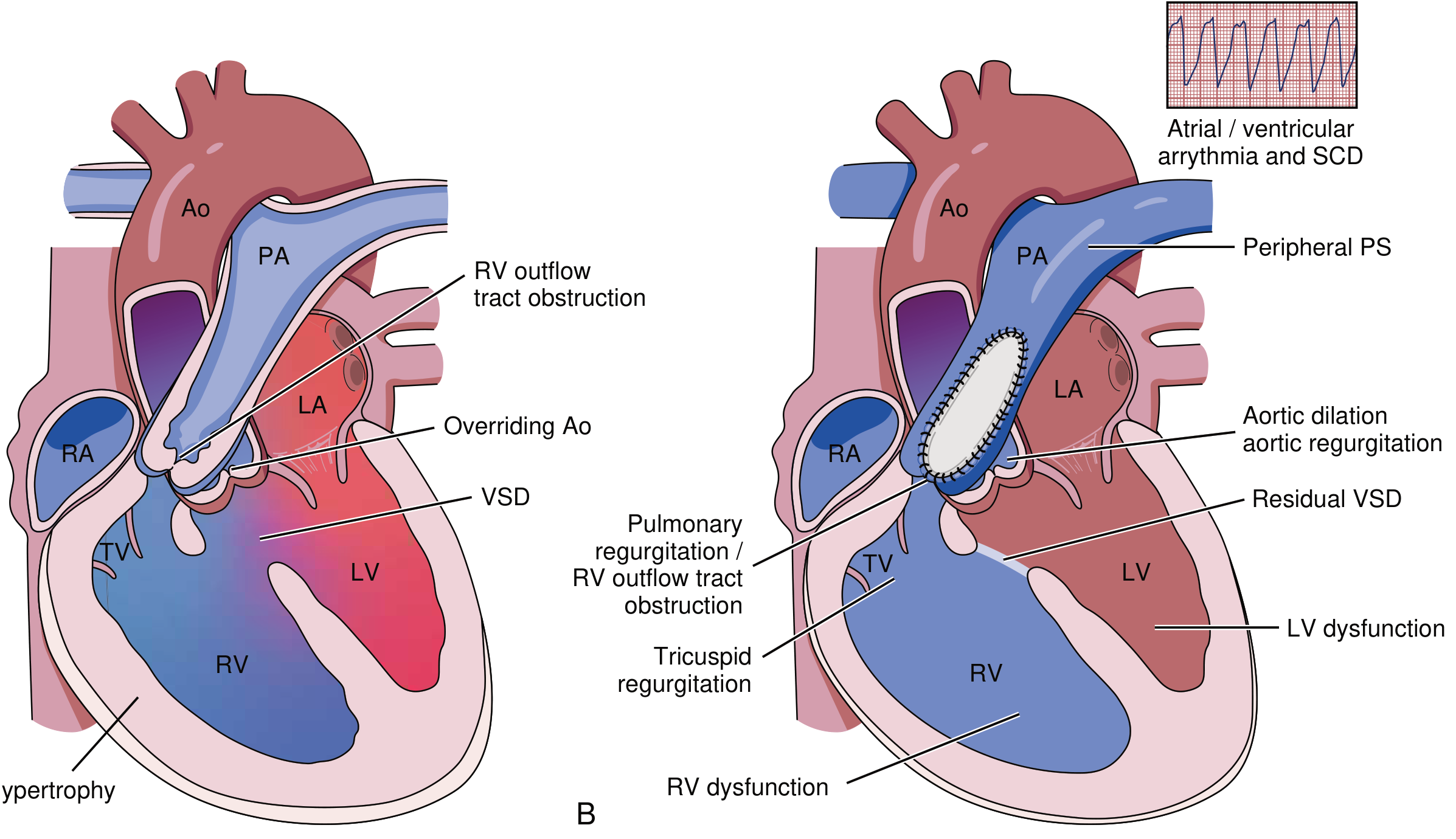
The Tetrad (Anatomic Basis)
TOF is caused by anterocephalad deviation of the outlet septum, producing four features:
| Feature | Consequence |
|---|---|
| RVOT obstruction (subvalvular/valvular/supravalvular) | Increased RV afterload, RV hypertrophy |
| Large subarterial VSD | Right-to-left shunting when RV pressure > LV |
| Overriding aorta (straddles VSD) | Receives mixed blood - desaturated |
| RV hypertrophy (compensatory) | Secondary to obstruction |
Pathophysiological Flow
Obstruction at RVOT
↓
RV pressure rises → exceeds LV pressure
↓
Right-to-left shunt across VSD
↓
Desaturated blood enters aorta → Cyanosis
↓
Chronic hypoxia → Polycythemia, clubbing, tet spells
↓
LV is "underfilled" (pulmonary blood flow is reduced)
Tet spells occur when RVOT spasm suddenly increases obstruction, dropping SpO2 acutely. LV is chronically small in severe TOF because it has received reduced pulmonary venous return.
- Braunwald's Heart Disease, p. 886
2. Surgical Steps of ICR for TOF
The repair is done on cardiopulmonary bypass (CPB) with aortic cross-clamping and cardioplegic arrest. The classic approach:
Access
- Median sternotomy + initiation of CPB (bicaval and aortic cannulation)
- Cardioplegic arrest
- Right atriotomy (preferred modern approach to avoid right ventriculotomy whenever possible)
Step 1 - VSD Closure
- Identify the large perimembranous/outlet VSD through the right atrium and tricuspid valve
- Close with a Dacron/Gore-Tex patch, securing it to avoid damage to the conduction system (AV node and His bundle run along the inferior rim of the VSD)
- Leaving a residual VSD causes L→R shunt post-op with volume overload
Step 2 - RVOT Relief (Infundibulectomy)
- Resection of hypertrophied infundibular muscle bundles (the obstructing bands in the subpulmonary region)
- If the pulmonary valve annulus is adequate: pulmonary valvotomy/commissurotomy only
- If annulus is too small: Transannular patch (TAP) - a patch is sutured across the pulmonary annulus + into the main PA, widening the RVOT. This reliably relieves obstruction but at the cost of pulmonary regurgitation (PR), which is the main long-term complication
Step 3 - Pulmonary Artery Augmentation (if needed)
- Branch PA stenosis may require patch augmentation
- If an anomalous LAD crosses the RVOT, a right ventricle-to-pulmonary artery conduit (RV-PA conduit) is used instead of a ventriculotomy or TAP
Optional - ASD Closure
- A coexistent ASD (or patent foramen ovale) is closed, unless intentionally left as a "pop-off" valve for restrictive RV physiology
Endpoint Criteria on the Table
-
Residual RVOT gradient < 30-40 mmHg (RV/LV pressure ratio < 0.7)
-
No significant residual VSD (by TEE, bubble study)
-
SpO2 on room air > 95% on coming off bypass
-
Braunwald's Heart Disease, p. 887
3. Post-ICR ICU Management
A straightforward ICR patient is often extubated within 12-24 hours. The ICU approach is organized around monitoring for and managing the three main post-op complications:
Routine Post-Op Care
| Parameter | Target |
|---|---|
| SpO2 | >95% (room air acceptable) |
| MAP | 55-70 mmHg |
| CVP | 8-12 mmHg (higher if restrictive RV) |
| Heart rate | 90-120 bpm in infants/children |
| Urine output | >1 mL/kg/hr |
| Temperature | Normothermia, avoid hyperthermia |
- Sedation/analgesia: Morphine + midazolam infusion; wean toward extubation
- Fluid: Crystalloid/colloid boluses <20 mL/kg in the first post-op night
- Inotropes: Milrinone (reduces RV afterload + positive inotropy) ± low-dose dopamine or dobutamine; wean as tolerated
- Pleural drains: Left in situ 24-48 hours due to pleural effusion risk
Complication 1 - Restrictive RV Physiology
This is the most important and most common ICU complication. It is defined echocardiographically as antegrade end-diastolic forward flow into the pulmonary artery (on pulse-wave Doppler in RVOT). The stiff, hypertrophied RV cannot relax and fill normally.
Risk factors:
- Pre-op severe desaturation
- Transannular patch repair
- Long bypass/cross-clamp time
- Pre-op RV hypertrophy >5 mm wall thickness
Clinical features:
- Low cardiac output syndrome (poor perfusion, hypotension, lactic acidosis)
- High CVP with hepatomegaly
- Positive fluid balance, ascites, pleural effusions
- Oliguria → may need peritoneal dialysis or CRRT
- Paradoxical improvement with spontaneous breathing (negative intrathoracic pressure augments RV filling and reduces RV afterload)
Management of Restrictive RV:
- Maintain preload - higher filling pressures (CVP 12-15); these patients are preload-dependent
- Milrinone - reduces PVR and RV afterload, improves relaxation
- Avoid tachycardia - need adequate diastolic filling time; consider low-dose beta-blocker if rate is very high
- Positive pressure ventilation (PPV) - use cautiously; increased intrathoracic pressure impairs RV filling. Consider early extubation when stable, as spontaneous breathing helps RV function
- Inhaled nitric oxide (iNO) - reduces pulmonary vascular resistance, unloads the RV
- Open the PFO/ASD - if a "pop-off" ASD was intentionally left open at surgery, this decompresses the right atrium at the cost of some cyanosis; accept SpO2 80-85% if cardiac output improves
- Peritoneal dialysis - for fluid overload and renal support
Complication 2 - Arrhythmias
Post-ICR arrhythmias arise because the repair involves the conduction system region.
| Arrhythmia | Cause | Management |
|---|---|---|
| Junctional ectopic tachycardia (JET) | Most common; catecholamine-induced; bypass-related | Cool patient to 35°C, amiodarone, atrial pacing at rate > JET rate, avoid inotropes if possible |
| Complete heart block (CHB) | Damage to His bundle near VSD inferior rim | Temporary epicardial pacing (wires placed at surgery); permanent PPM if persists >10-14 days |
| AF/flutter | Older patients with repaired TOF | Rate control / cardioversion |
| VT/VF | Late complication (scar in RVOT); rare acute post-op | ACLS, treat electrolytes, amiodarone |
Epicardial pacing wires are routinely placed at surgery (RA + RV wires) and are used for temporary pacing, overdrive pacing for JET, and diagnosing arrhythmias.
Complication 3 - Residual Lesions
These are detected on post-op echo (TEE on table + TTE in ICU):
| Residual Lesion | Echo Finding | Action |
|---|---|---|
| Residual RVOT gradient | Peak gradient >40 mmHg on CW Doppler | If hemodynamically significant with low CO → return to OR or catheter intervention |
| Residual VSD | Color Doppler L→R jet through patch | Small (<3 mm): observe; large: re-exploration |
| Pulmonary regurgitation | Diastolic reverse flow in RVOT | Expected after TAP; severity guides long-term follow-up |
| Aortic regurgitation | Diastolic jet in LVOT | If VSD patch distorts aortic annulus |
The RV/LV Hyperdynamic State (What Your Consultant Was Discussing)
In the first 12-48 hours post-ICR:
- The RV is suddenly decompressed after years of pressure overload → it now ejects against a low-resistance pulmonary circuit → appears hyperdynamic on echo (high fractional area change, rapid ejection)
- The LV now receives full pulmonary venous return (previously reduced due to low pulmonary blood flow) → fills better → also appears hyperdynamic
- Doppler will show a residual gradient across the RVOT (mild to moderate is expected and accepted; >40 mmHg is concerning)
- The consultant was likely reviewing the echo and noting: "The RV and LV are both hyperdynamic - this is expected post-decompression. There's a residual gradient of X mmHg - we'll watch this."
This pattern is reassuring as long as cardiac output is maintained and there is no hemodynamic compromise.
Summary at a Glance
| Topic | Key Point |
|---|---|
| ICR | Intracardiac repair for TOF - VSD patch + RVOT relief on CPB |
| Pathophysiology | RVOT obstruction → RV hypertension → R→L shunt via VSD → cyanosis |
| Post-op gradient | Residual RVOT pressure gradient; acceptable <30-40 mmHg |
| Hyperdynamic RV+LV | Expected post-decompression; RV unloaded, LV preload normalized |
| Biggest ICU risk | Restrictive RV physiology → low cardiac output |
| Key drug | Milrinone (PDE3 inhibitor - inotrope + vasodilator, reduces PVR) |
| Key monitor | Epicardial pacing wires, LA line (if placed), CVP, echo |
| Extubation target | 12-24 hours if uncomplicated |
Sources: Braunwald's Heart Disease, pp. 886-887; Textbook of Clinical Echocardiography, pp. 554-556; Frontiers Pediatrics - Management of TOF in PICU (2023)
This is a shared conversation. Sign in to Orris to start your own chat.