Steps surgical umbilical hernia
Reading File
Finding Sources
Searching the Web
surgical steps umbilical hernia repair Mayo repair mesh technique
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from Fischer's Mastery of Surgery and Bailey & Love to provide a thorough answer.
Surgical Steps: Umbilical Hernia Repair
Umbilical hernia repair can be performed by three main approaches depending on defect size and patient factors. The approach is chosen before the procedure begins.
Decision Framework (Defect Size-Based)
| Defect Size | Recommended Approach |
|---|---|
| < 1 cm | Primary suture repair (tissue-only) |
| 1-2 cm | Primary suture repair OR mesh (patient/surgeon-dependent) |
| > 2 cm | Mesh repair strongly recommended |
| > 4 cm | Laparoscopic repair preferred |
A. Open Primary Suture Repair (No Mesh)
Indication: Defects < 1-2 cm, BMI < 30, no high-risk comorbidities.
Steps:
-
Anaesthesia - General or local anaesthesia with sedation.
-
Incision - A curvilinear (supraumbilical or infraumbilical) incision is made in a natural skin crease, not exceeding 180°. An umbilical incision through the umbilicus itself is also an option for cosmesis.
-
Dissection - Dissect through dermis. Identify the hernia sac and umbilical stalk. Dissect the sac circumferentially around the umbilical stalk. Take care not to injure the overlying skin.
-
Hernia sac dissection - Separate the hernia sac from the umbilical stalk. The sac is opened and its contents inspected.
-
Reduction of contents - Reduce hernia contents (usually omentum or preperitoneal fat) back into the abdominal cavity. If the contents cannot be reduced, they can be ligated and excised at fascial level (for omentum/fat). If bowel is involved and ischaemic, midline extension may be required.
-
Peritoneal closure - The peritoneum is closed with an absorbable running suture.
-
Fascial clearance - Clear the fascia circumferentially to ensure adequate bites during closure.
-
Defect closure:
- Very small (< 1 cm): Simple interrupted sutures in transverse direction, or figure-of-eight sutures. Use 2-0 slowly absorbable monofilament (e.g., PDS) or nonabsorbable suture. A "darn" repair using criss-crossed non-absorbable monofilament is also acceptable.
- Up to 2 cm - Mayo ("waistcoat-over-trousers") technique: Extend the defect transversely. Create two fascial flaps. Overlap the superior flap over the inferior flap by 3 cm. Fix with horizontal mattress sutures using 0 non-absorbable or long-acting absorbable monofilament. Relaxing incisions 5 cm lateral to the defect may be needed.
-
Umbilicus reconstruction - Reapproximate the umbilical stalk back to the linea alba with absorbable sutures to create a cosmetically acceptable bellybutton. Suture the apex of subcutaneous tissue below the umbilicus to the linea alba to invert the navel.
-
Skin closure - Redundant skin is excised if needed. Subcutaneous dead space is obliterated with absorbable sutures. Skin is reapproximated with slowly absorbable subcuticular suture. Dressing applied.
B. Open Mesh Repair
Indication: Defects > 1-2 cm, high-risk comorbidities (obesity, diabetes, COPD, collagen disorders), recurrent hernia.
Preperitoneal (Sublay) Repair - Preferred Open Mesh Technique
- Incision and dissection - Same as above; curvilinear incision, dissect to hernia sac.
- Preserve hernia sac - The sac is preserved initially to help identify and enter the preperitoneal plane.
- Create preperitoneal pocket - Dissect in the preperitoneal plane circumferentially under the fascia, creating a pocket large enough to accommodate mesh with 3-5 cm overlap beyond the defect edge.
- Close peritoneal defects - Any holes in the peritoneum are closed with absorbable suture.
- Mesh placement - A flat sheet of polypropylene mesh (non-coated) is placed flat in the preperitoneal space. Intra-abdominal pressure is usually sufficient to hold it - fixation sutures are often not required.
- Fascial closure - The fascial defect is closed over the mesh using permanent or slowly absorbable suture.
- Skin closure - As above.
Open Intraperitoneal Repair (Hernia Patch)
- Used when the peritoneum is too thin to create a reliable preperitoneal pocket.
- A barrier-coated hernia patch (e.g., polypropylene with antiadhesive coating) is placed intraperitoneally.
- Inserted through the defect, positioned centrally, and secured with 0 non-absorbable sutures to the anterior abdominal wall at the 12, 6, 3, and 9 o'clock positions (through linea alba and rectus sheath).
- Fascia is then re-approximated over the mesh.
Mesh note: A flat sheet (non-coated) is suitable for onlay or preperitoneal positions. If mesh contacts viscera (intraperitoneal), an antiadhesive barrier-coated mesh is mandatory to prevent bowel adhesion, erosion, and fistulation.
C. Laparoscopic Umbilical Hernia Repair
Indication: Defects > 4 cm, obese patients, recurrent hernias.
Steps:
- Port placement - Camera port + two working ports placed laterally on the abdominal wall, well away from the defect.
- Reduction of contents - Contents of the hernia are reduced by traction and external pressure.
- Adhesiolysis - The falciform ligament (above) and median umbilical fold (below) may need to be taken down to create a smooth surface for mesh placement.
- Mesh sizing - A disc of non-adherent mesh (designed for intraperitoneal use) is introduced; it must provide adequate overlap.
- Mesh placement and fixation - Positioned on the undersurface of the abdominal wall, centred on the defect. Fixed to the peritoneum and posterior rectus sheaths using staples, tacks, or sutures.
- Port closure - Port sites closed.
Laparoscopic note: This approach achieves generous overlap without surgical damage to the umbilicus and surrounding fascia. However it requires specialised, expensive tissue-separating mesh, and intraperitoneal mesh carries risks of bowel adhesion, erosion, and fistulation. Tack fixation can cause severe chronic pain.
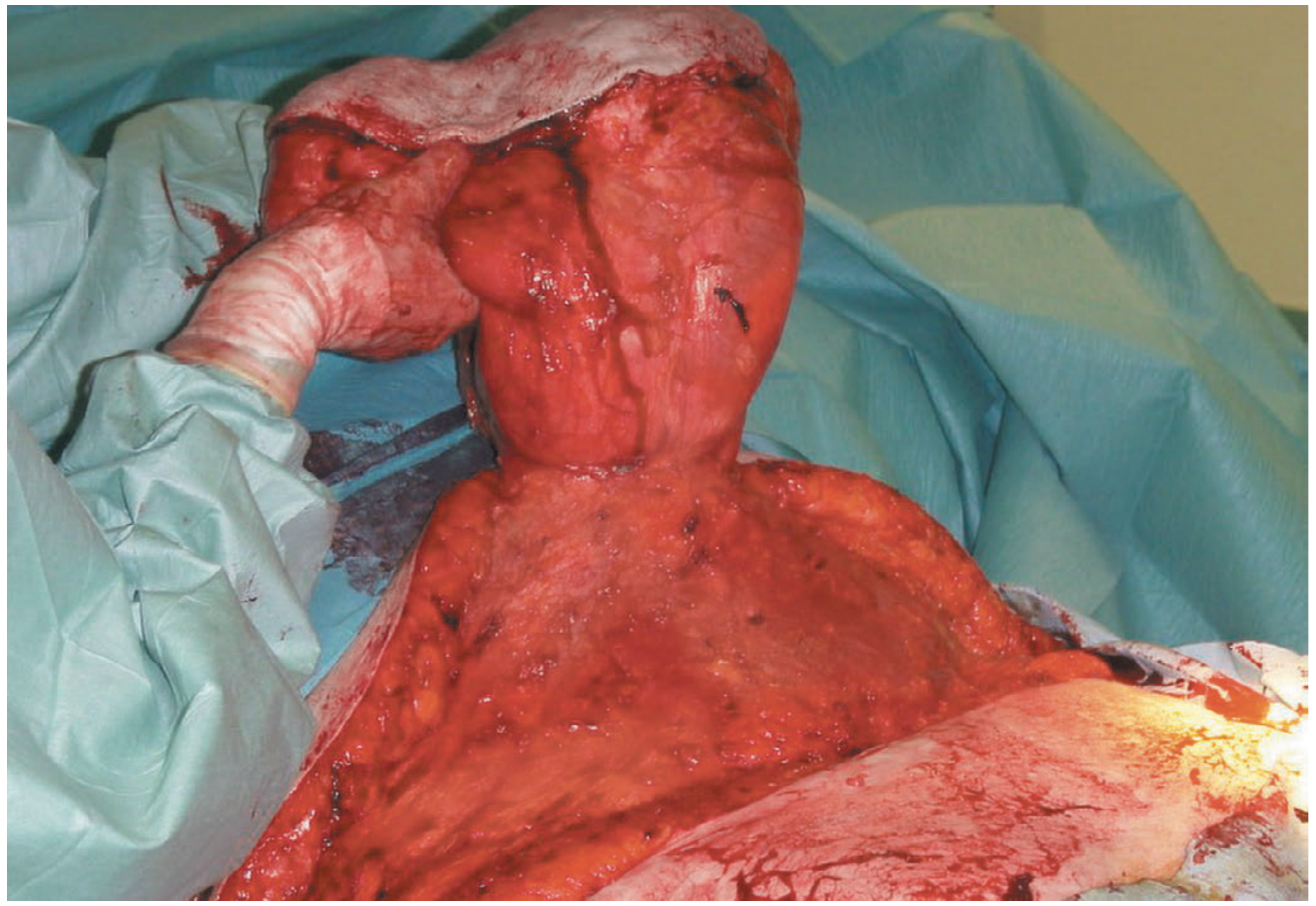
Intraoperative Image
Massive umbilical hernia - intraoperative view, showing the hernia contents prior to reduction:
Special Considerations
- Cirrhosis / ascites: Fascial repair with fine continuous sutures minimises risk of post-operative ascites leakage. Child's B/C disease carries very high mortality - careful patient selection required.
- Pregnancy: Avoid repair before or during pregnancy unless the hernia is large, significantly symptomatic (pain, obstruction), and surgery is considered in the 2nd trimester.
- Children: Umbilical hernias usually resolve by age 2; repair delayed until age 5 if persistent. Primary repair (no mesh) is used in children.
- Recurrence risk factors: Obesity, diabetes, COPD, collagen synthesis disorders - all favour mesh over suture repair.
Sources:
- Fischer's Mastery of Surgery, 8th ed., Ch. 216 (Primary Umbilical Hernia Repair; Mesh-Based Umbilical and Epigastric Hernia Repair)
- Bailey and Love's Short Practice of Surgery, 28th ed., Ch. 64 (Open and Laparoscopic Umbilical Hernia Repair)
This is a shared conversation. Sign in to Orris to start your own chat.