Subtotal petrosectomy
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
Subtotal petrosectomy
Reading File
Searching the Web
subtotal petrosectomy skull base surgery technique indications
Searching PubMed
subtotal petrosectomy skull base
Finding Sources
Reading Web Page
subtotal petrosectomy technique indications steps
Finding Sources
Reading Article
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
I now have sufficient information from textbooks, literature, and the web extract. Let me compile a comprehensive answer.
Subtotal Petrosectomy (STP)
Definition and Concept
Subtotal petrosectomy is an otological/skull base surgical procedure that exenterates the majority of the pneumatic cells of the petrous temporal bone while preserving the otic capsule. It converts the middle ear cleft into a permanently obliterated, closed space - sealing the ear from the outside environment. The term distinguishes it from total petrosectomy (which removes the otic capsule and labyrinth entirely).
The four defining steps, as described by Fisch and later formalized by Prasad et al. (Laryngoscope 127:2833, 2017), are:
- Blind sac closure (BSC) of the external auditory canal (EAC) - the EAC skin is removed and the meatus is closed in two layers, permanently separating the canal from the outside world
- Canal wall down mastoidectomy (CWDM) with complete removal of all middle ear epithelium and pathology
- Exenteration of all mastoid, perisigmoid, perilabyrinthine, perifacial, and hypotympanic cells - with retention of the otic capsule, fallopian canal, and middle and posterior fossa plates
- Obliteration of the surgical cavity with abdominal fat, plus Eustachian tube occlusion
Indications
Primary / Otological Indications
| Indication | Notes |
|---|---|
| Recurrent/recalcitrant chronic otitis media with or without cholesteatoma | Most common (35.9% in Prasad's series of 460 cases) |
| Failed prior canal wall down or canal wall up mastoidectomy | Often the 2nd or 3rd revision surgery |
| Radical mastoid cavity problems (persistent discharge, difficult care) | Eliminates cavity maintenance |
| Osteoradionecrosis of the temporal bone | After head and neck radiotherapy |
| Temporal bone fractures involving the otic capsule | To control CSF leak and prevent meningitis |
Cochlear Implantation (CI) Indications
STP is used to prepare the ear for cochlear implantation when the middle ear is unsafe or inaccessible via conventional approaches. Specific CI-related indications:
- Chronic otitis media / cholesteatoma / osteoradionecrosis
- Existing radical cavity or prior canal wall down surgery
- Cochlear ossification / obliteration
- Inner ear malformations (especially IP-I and IP-III, which risk CSF gusher - STP with blind sac closure and ET obliteration hermetically seals the ear)
- Temporal bone fracture involving the otic capsule
- Unfavorable anatomical conditions
- Revision CI surgery in an infected field
- Skull base lesions where the cochlear nerve and cochlea are preserved
As noted in Cummings Otolaryngology Head and Neck Surgery: in children with persistent CSF leak or recurrent meningitis after cochlear implantation, "the ear can be hermetically sealed by performing a subtotal petrosectomy with blind sac closure of the ear canal and obliteration of the Eustachian tube."
Skull Base Indications
- Jugular foramen tumors (paragangliomas, schwannomas): STP extends atticomastoidectomy to enable wider facial nerve transposition. According to Scott-Brown's Otorhinolaryngology: "In order to be able to mobilize the facial nerve more extensively, atticomastoidectomy should be extended to subtotal petrosectomy. This involves removal of the skin of the external auditory meatus along with the tympanic membrane, the malleus and incus, drilling away the posterior canal wall and extensive exenteration of pneumatic cells."
- Class B3 tympanomastoid paragangliomas (8.3% of Prasad's series)
- Petroclival lesions (chordomas, meningiomas, cholesterol granulomas) - as a component of extended skull base approaches
- Parotid neoplasms requiring mastoidectomy in a field at high risk for radionecrosis - STP with obliteration is used prophylactically
Surgical Technique
Positioning and Setup
- Supine with head rotated, facial nerve monitoring mandatory
- Retroauricular incision (C-shaped or extended postauricular), wider shaving than standard CI
Step 1 - Blind Sac Closure of EAC
- Circumferential incision at the bony-cartilaginous junction
- Complete removal of EAC skin (lateral and medial portions)
- Annulus, malleus, and incus removed
- Meatus closed with anterior pedicled musculoperiosteal flap in two watertight layers
Step 2 - Canal Wall Down Mastoidectomy
- Complete atticomastoidectomy with removal of the posterior canal wall
- All middle ear epithelium removed; tympanic membrane, ossicles, and any disease cleared
Step 3 - Cell Exenteration
- Exenteration of: mastoid cells, perisigmoid cells, perilabyrinthine cells, perifacial cells (around the fallopian canal), and hypotympanic bone/cells
- Structures preserved: otic capsule (cochlea and labyrinth), fallopian canal (with facial nerve intact), middle fossa dural plate, posterior fossa/sigmoid sinus plate
- Eustachian tube orifice is obliterated (with muscle plug, bone wax, or a combination)
Step 4 - Cavity Obliteration
- Surgical defect filled with abdominal fat (harvested from a separate incision)
- Fat obliteration eliminates all dead space, prevents fluid accumulation and infection
For CI: The Cochleostomy
- After obliteration setup, cochleostomy is performed through the round window or via a cochleostomy anterior-inferior to it
- Array inserted; lead exited to the implant bed through a separate bony channel
- Cavity then packed with fat around the electrode
For Skull Base Extension (jugular foramen)
- After STP, the facial nerve is mobilized from its full mastoidal and tympanic segments
- Rerouted anteriorly with the pivot at the second genu (limited) or first genu (maximum exposure)
- Sigmoid sinus/jugular bulb controlled with Surgicel packing or ligation
- IJV ligated high in the neck after extending the incision inferiorly
Key Anatomical Landmarks and Relations
- Otic capsule: preserved (distinguishes STP from total petrosectomy)
- Fallopian canal: skeletonized but preserved (the facial nerve remains in situ unless transposition is needed)
- Sigmoid sinus: skeletonized during cell exenteration
- Jugular bulb: dome exposed by diamond burr removal of overlying bone
- Eustachian tube: obliterated to prevent reflux of secretions into the cavity
- Internal carotid artery: petrous segment at risk in extensive procedures; must be identified and protected
Outcomes (Prasad et al., largest series - 460 cases)
- 64.6% of patients had undergone multiple prior surgeries before STP
- Complications rate: very low - recidivism and postauricular wound fistula were the most common at only 1.1% each
- CI outcomes after STP: comparable to standard CI; 80% of cases can be done as a single-stage procedure
- A 2023 Italian multicenter review (PMID 37698103) of 55 patients (mean follow-up 44 months) confirmed STP + CI is safe; cholesteatoma was the most common indication; single-stage surgery was the preferred strategy
Complications
- Recidivism of cholesteatoma (if epithelium removal incomplete before obliteration): most important long-term risk
- Postauricular wound fistula / fat necrosis: fat may liquefy, creating a fistulous tract
- Facial nerve injury: risk varies with degree of transposition required
- CSF leak: particularly with skull base extensions or in cases with pre-existing dural defects
- Device extrusion or infection (CI cases): dramatically reduced by STP compared to implanting into a diseased ear
- Postoperative meningitis: reduced by hermetic sealing
Comparison to Related Procedures
| Procedure | Otic Capsule | Hearing | Key Use |
|---|---|---|---|
| Canal wall down mastoidectomy | Preserved | Preserved | Cholesteatoma without CI need |
| Subtotal petrosectomy | Preserved | Sacrificed (conductive; CI possible) | Recalcitrant disease + CI or skull base access |
| Translabyrinthine approach | Removed | Sacrificed | Acoustic neuroma, IAC tumors |
| Total petrosectomy | Removed | Sacrificed | Temporal bone malignancy |
Summary
STP is an expanding procedure in the modern otology/skull base armamentarium. Its threshold for use is decreasing as more surgeons recognize its value: it provides definitive disease clearance, eliminates cavity maintenance, hermetically seals the ear from infection, enables safe cochlear implantation in a hostile ear, and opens wide surgical access for jugular foramen and petrous apex pathology. When correctly performed, it carries minimal morbidity. - Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2; Cummings Otolaryngology Head and Neck Surgery
Bells palsy
Reading File
Searching PubMed
Bell's palsy treatment management
Finding Sources
Reading Article
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, high-quality content from Harrison's, Adams & Victor, and Scott-Brown's. Here is the full answer:
Bell's Palsy
Definition and Epidemiology
Bell's palsy is the most common cause of acute unilateral peripheral (lower motor neuron) facial paralysis - accounting for approximately 60-75% of all cases of acute unilateral facial palsy. It is a diagnosis of exclusion: all other identifiable causes must be ruled out before the label is applied.
- Incidence: ~23-25 per 100,000 per year; roughly 1 in 60 persons in a lifetime
- Sex: affects men and women approximately equally
- Age: any age; peak incidence in the 15-45 year range
- Risk factors: pregnancy (especially third trimester and early postpartum, up to threefold increase cited), diabetes mellitus, hypertension, immunosuppression
- Recurrence: ~7-8% of cases; average interval ~10 years between episodes
Pathophysiology
The leading hypothesis - now supported by molecular evidence - is reactivation of herpes simplex virus type 1 (HSV-1) in the geniculate ganglion of the facial nerve within the petrous temporal bone. Murakami et al. (1996), using PCR, identified HSV-1 DNA in the endoneurial fluid surrounding the facial nerve in 11 of 14 patients with Bell's palsy during surgical decompression. The same group reproduced facial paralysis in mice by inoculating HSV into the ears. The virus causes:
- Inflammatory edema of the facial nerve
- Compression of the swollen nerve within the tight confines of the fallopian canal
- Ischemia and demyelination - or in severe cases, axonal degeneration
Varicella zoster virus (VZV) accounts for up to one-third of cases and may be the second most frequent cause. When VZV reactivation produces a vesicular rash in addition to facial palsy, the syndrome is called Ramsay Hunt syndrome (herpes zoster oticus), which carries a worse prognosis than Bell's palsy. SARS-CoV-2 and HIV seroconversion have also been implicated.
The pathological findings on the rare occasions when the nerve has been examined show varying degrees of nerve fiber degeneration, inflammatory infiltrate of mononuclear cells, and edema of the nerve sheath.
Clinical Features
Onset: Abrupt - about half of patients reach maximal weakness within 48 hours; nearly all within 3-4 days.
Motor: Complete or partial unilateral lower motor neuron (LMN) facial paralysis:
- Inability to close the eye (lagophthalmos) - risk of corneal exposure injury
- Loss of nasolabial fold, drooping of the corner of the mouth
- Inability to wrinkle the forehead (distinguishes LMN from UMN palsy)
- Inability to puff out cheeks, whistle, or show teeth on the affected side
Sensory / autonomic features:
- Pain behind the ear (mastoid region) - may precede paralysis by 1-2 days; occasionally intense and persistent
- Loss of taste on the anterior two-thirds of the tongue (chorda tympani involvement) - indicates the lesion is proximal to where the chorda tympani joins the main nerve
- Hyperacusis - paralysis of the stapedius muscle (nerve to stapedius branch) causes recruitment of loud sounds on the ipsilateral side
- Mild numbness or fullness in the face (some patients), though true sensory loss is uncommon
- Reduced lacrimation or salivation in some cases (greater superficial petrosal nerve involvement)
CSF: Mild lymphocytosis in a small number of patients.
Grading
The House-Brackmann (HB) Scale is the standard grading system:
| Grade | Description | Function |
|---|---|---|
| I | Normal | 100% |
| II | Slight dysfunction | Slight weakness on close inspection; complete eye closure |
| III | Moderate | Obvious difference; complete eye closure with effort |
| IV | Moderately severe | Obvious weakness; incomplete eye closure |
| V | Severe | Barely perceptible motion; incomplete eye closure |
| VI | Total paralysis | No movement |
Differential Diagnosis
Bell's palsy is a diagnosis of exclusion. The following must be actively considered:
| Condition | Clues |
|---|---|
| Ramsay Hunt syndrome (VZV) | Vesicular eruption in EAC, pinna, palate; more severe palsy; VIII nerve involvement (SNHL, vertigo) |
| Lyme disease | Tick exposure, erythema migrans, can be bilateral; in endemic areas, ≥10% of facial palsies |
| Otitis media / cholesteatoma | Abnormal otoscopy, conductive hearing loss |
| Parotid malignancy | Slow onset, palpable parotid mass |
| Acoustic neuroma / CPA tumor | Other cranial nerve signs, progressive course, abnormal MRI |
| Sarcoidosis | Can be bilateral (Heerfordt's syndrome); elevated ACE, chest imaging |
| Guillain-Barré syndrome | Often bilateral facial palsy, ascending weakness, areflexia, CSF albuminocytologic dissociation |
| Melkersson-Rosenthal syndrome | Recurrent facial palsy, facial/labial edema, fissured tongue |
| Diabetes mellitus | Facial neuropathy as mononeuropathy |
| Leprosy | Endemic regions, skin changes, peripheral nerve thickening |
| Malignant otitis externa | Immunocompromised/diabetic, ear pain, skull base involvement |
| UMN lesion (stroke, tumor) | Forehead sparing, ipsilateral limb signs, other cranial nerve deficits |
Key distinguishing feature of LMN vs. UMN palsy: In UMN (supranuclear) lesions, the frontalis (forehead wrinkling) and orbicularis oculi are relatively spared because the upper face has bilateral cortical representation. In Bell's palsy (LMN), the entire ipsilateral face is involved, including the forehead.
Investigations
The diagnosis is clinical in straightforward cases with:
- Typical acute presentation
- No risk factors pointing to another cause
- No vesicular rash in the ear (which would suggest Ramsay Hunt)
- Normal neurological exam apart from CN VII
- Normal otoscopy and hearing
Investigations to consider in atypical/uncertain cases:
- MRI with gadolinium: Shows swelling and smooth linear enhancement of the geniculate ganglion and facial nerve segments within the temporal bone (genu, tympanic, mastoid segments). This is highly suggestive of Bell's palsy but is not pathognomonic - Lyme disease, sarcoidosis, and perineural malignant spread can look identical.
- Blood glucose / HbA1c (diabetes)
- ESR / CRP
- Lyme serology (in endemic areas)
- HIV serology
- ACE level + chest imaging (sarcoidosis)
- Lumbar puncture (if Guillain-Barré suspected - bilateral palsy, areflexia)
Electrophysiology (EMG/ENoG):
- Evidence of denervation on EMG after 10 days indicates axonal degeneration - predicts prolonged recovery (3+ months) and possible incomplete recovery
- Electroneurography (ENoG): >90% degeneration correlates with poor prognosis
- Early motor recovery within 5-7 days is the most favorable prognostic sign
MRI Appearance
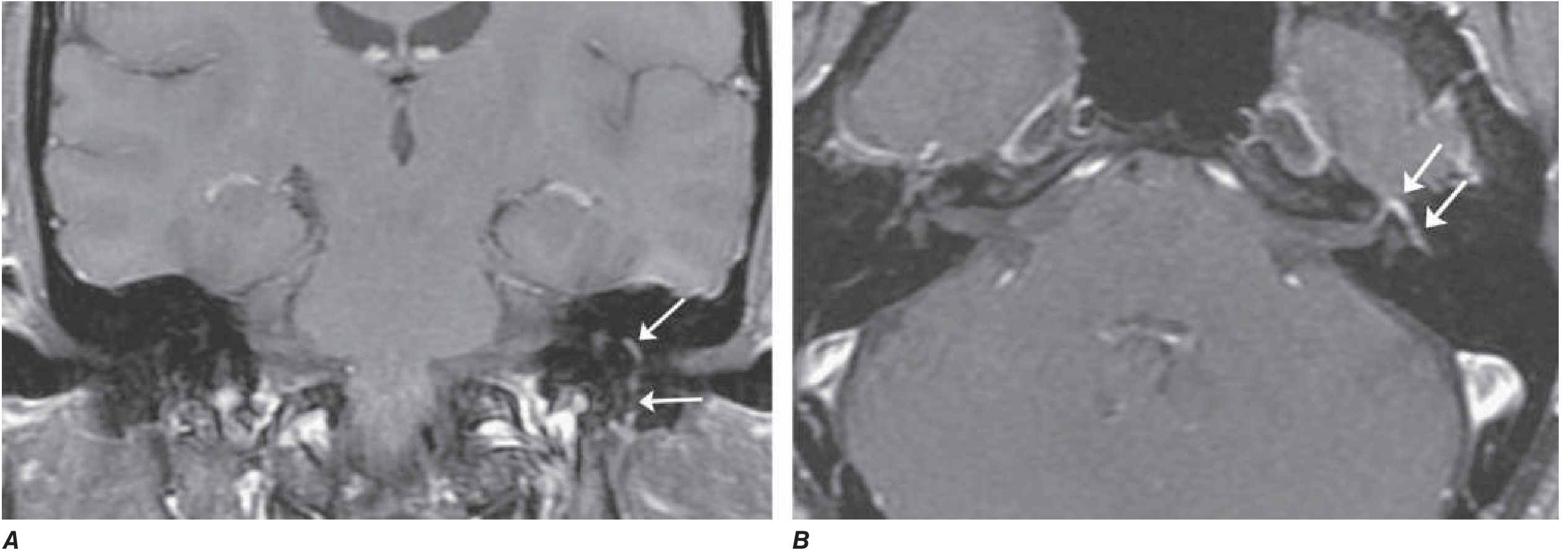
Axial (B) and coronal (A) T1-weighted gadolinium-enhanced MRI with fat suppression: diffuse smooth linear enhancement of the left facial nerve involving the genu, tympanic, and mastoid segments within the temporal bone (arrows). No mass lesion. Highly suggestive of Bell's palsy but similar findings occur in Lyme disease, sarcoidosis, and perineural malignant spread. - Harrison's Principles of Internal Medicine, 22nd Ed.
Treatment
1. Corticosteroids (strongly recommended)
The cornerstone of treatment. Must be started within 72 hours of onset for maximum benefit.
- Prednisone 60-80 mg/day for the first 5 days, then tapered over the next 5 days (Harrison's 22E)
- Alternative: prednisolone 40-60 mg/day for 7-10 days
- Mechanism: reduces nerve edema and pressure within the fallopian canal
- Benefit: modestly but significantly shortens recovery and improves functional outcome
- The 2023 Japanese clinical practice guidelines (PMID 39079445) strongly recommend systemic standard-dose corticosteroids; high-dose corticosteroids showed no significant advantage over standard-dose in a 2023 systematic review and meta-analysis (PMID 36706448)
- Children: recovery rate is ~90% regardless of treatment; steroid use is debated and not universally recommended
2. Antiviral agents (weakly recommended)
- Most large randomized trials, including the landmark Sullivan trial, found no added benefit of valacyclovir or acyclovir over corticosteroids alone
- Should be added if vesicular lesions are present in the EAC or palate (suggesting VZV/Ramsay Hunt), or in severe/complete palsy
- Regimens: valacyclovir 1000 mg/day for 5-7 days, or acyclovir 400 mg five times daily for 10 days
- One RCT (Hato et al.) suggested additive benefit of valacyclovir + prednisolone over prednisolone alone in complete palsy - hence weak recommendation persists in guidelines
- Oral vs. IV steroids: a 2024 meta-analysis (PMID 37940744) found no significant difference between oral and IV steroid administration
3. Eye care (mandatory)
- Artificial tears during the day (lubricating eye drops)
- Lubricating eye ointment at night
- Tape the upper eyelid shut during sleep to prevent corneal drying (lagophthalmic keratitis)
- In severe lagophthalmos: moisture chamber, temporary tarsorrhaphy, or gold weight implant in upper eyelid
4. Physical therapy
- Facial neuromuscular retraining, massage, mirror exercises
- A 2025 systematic review (PMID 39647183) supports physical therapy for idiopathic facial palsy, though evidence quality remains limited
5. Surgical decompression
- Not recommended as routine treatment - there is no good evidence of benefit, and it may cause harm
- The 2023 Japanese guidelines weakly recommend it only in selected severe cases
- Decompression of the meatal foramen (narrowest part of the fallopian canal, where the nerve is most compressed) has been proposed, but the evidence base remains weak
6. Botulinum toxin / reanimation surgery
- Botulinum toxin useful for synkinesis (aberrant reinnervation causing co-contraction) after recovery
- Surgical reanimation (nerve grafting, muscle transfer, static procedures) for permanent paralysis
Prognosis
- ~70% recover completely within 1-2 months; ~85% achieve near-normal function (Adams & Victor)
- ~80% recover within weeks to months (Harrison's)
- Incomplete paralysis in the first week = most favorable prognostic sign
- Early return of taste in week 1 = favorable sign
- Complete paralysis at onset + >90% degeneration on ENoG = poor prognosis
- Axonal degeneration (seen after 10 days on EMG) predicts 3+ month delay in recovery
- Recurrence rate: ~7-8% of cases
Bell's Palsy in Pregnancy
- Incidence is increased, particularly in the third trimester and first 2 weeks postpartum (up to threefold cited, though disputed)
- Managed similarly to non-pregnant patients; short-course prednisolone is generally considered safe after the first trimester
- Antivirals: use with caution; consult obstetric guidance
Key Teaching Points
- Always check the ear (otoscopy) and hearing before labelling a facial palsy as Bell's - abnormal findings point to an alternative diagnosis
- Check for vesicles in the EAC - if present, this is Ramsay Hunt (VZV), not Bell's, and requires antiviral therapy
- Forehead involvement confirms peripheral (LMN) palsy - if the forehead is spared, suspect a central (UMN) lesion
- Steroids within 72 hours = best outcomes; beyond 72 hours the benefit is unproven
- Protect the cornea - exposure keratitis is the most urgent complication
Sources: Harrison's Principles of Internal Medicine, 22nd Ed.; Adams and Victor's Principles of Neurology, 12th Ed.; Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 1; Japanese Clinical Practice Guidelines for Bell's Palsy 2023 (PMID 39079445)
Coblation in ent
Finding Sources
Searching PubMed
coblation tonsillectomy ENT outcomes
Finding Sources
Searching PubMed
coblation versus other tonsillectomy techniques pain hemorrhage
Reading File
Reading File
Reading File
Reading File
Reading File
Reading Article
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive content. Let me compile the full answer.
Coblation in ENT
The Technology - What is Coblation?
Coblation (Controlled Ablation) is a proprietary bipolar radiofrequency (RF) energy-based technology developed by ArthroCare Corporation (now Smith & Nephew). The name is a portmanteau of "controlled ablation."

PROCISE laryngeal Coblation wand - Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Mechanism of Action
RF energy is delivered through a bipolar wand immersed in a conductive saline medium (either external irrigation or saline gel at the tip). The current ionizes the sodium ions in the saline, creating a plasma field - a thin layer of highly energized charged particles (active protons/ions). These plasma particles have sufficient energy to break molecular bonds within tissue (molecular dissociation) rather than generating bulk heat.
This achieves tissue removal, tissue shrinkage, or vessel coagulation at comparatively low temperatures of 40-70°C - in stark contrast to:
- Monopolar electrocautery: >400°C
- Bipolar diathermy: ~400°C
- Laser: very high focal temperatures
- Harmonic scalpel: mechanical energy but generates ~80°C
The result is tissue ablation with minimal thermal spread to surrounding structures, reduced charring, and - at least theoretically - less collateral tissue damage.
ENT Applications
1. Tonsillectomy
Introduced in 2001, coblation tonsillectomy is now one of the most widely used techniques worldwide. The wand is used to dissect the tonsil en bloc outside its capsule (extracapsular) while the bipolar coagulation function simultaneously controls bleeding.
Technique: The tonsil is grasped and retracted medially. The coblation wand simultaneously ablates and coagulates as it follows the capsular plane, separating the tonsil from the underlying superior constrictor muscle. Lower temperatures theoretically reduce damage to the constrictor musculature, resulting in less postoperative pain and faster healing.
Evidence:
- Multiple studies show coblation is comparable to electrocautery for postoperative pain, hemorrhage, and recovery - K.J. Lee's Essential Otolaryngology
- A Cochrane review of nine trials found no significant differences in pain or speed of recovery between coblation and other tonsillectomy techniques - Cummings Otolaryngology
- A 2023 systematic review and meta-analysis of 6 studies (1,824 adult patients) comparing coblation vs. bipolar diathermy found no significant differences in reactionary hemorrhage (OR 1.81, p=.51), delayed hemorrhage (OR 0.72, p=.20), or postoperative pain, though there was a general trend favoring coblation and a greater healing effect on tonsillar tissue. Coblation had a slightly longer operating time. (PMID 33719616)
- Post-tonsillectomy hemorrhage remains the most feared complication and rates with coblation are comparable to other techniques (~1-5%)
Tonsillotomy (intracapsular) via coblation: Partial tonsil removal preserving the capsule ("powered intracapsular tonsillectomy") - used especially in children with sleep-disordered breathing. Reduces pain and hemorrhage risk but carries a small risk of tonsil regrowth.
2. Adenoidectomy
Coblation is suitable for adenoidectomy under direct endoscopic vision. Compared to traditional cold curettage:
- Less intraoperative blood loss
- More complete adenoid removal (particularly of residual lateral nasopharyngeal tissue)
- Allows precise tissue removal under vision, reducing the risk of damage to the Eustachian tube orifices and soft palate
- Cost limitation: the high unit cost of single-use wands restricts its use as a sole procedure for adenoidectomy alone; however, when tonsillectomy is being performed simultaneously using the same wand, the marginal cost of performing adenoidectomy is negligible
3. Inferior Turbinate Reduction
Coblation inferior turbinate reduction (CITR) is classified under mucosal preservation surgery, alongside radiofrequency ablation, submucosal diathermy, and microdebrider reduction. It is preferred over mucosal-destructive techniques (cautery, laser, cryosurgery) because it spares the overlying mucosa and ciliated epithelium.
Technique: The coblation wand is inserted submucosally into the inferior turbinate and activated as it is withdrawn, creating a controlled area of submucosal tissue ablation and fibrosis, reducing turbinate volume while preserving surface mucosa and its mucociliary function.
Indications: Inferior turbinate hypertrophy causing nasal obstruction - particularly in allergic or non-allergic chronic rhinitis unresponsive to medical therapy.
Evidence: Long-term follow-up studies (Leong et al., Cavaliere et al.) show significant improvement in nasal airflow and symptoms at 3 and 32 months post-operatively. Cummings Otolaryngology notes that no single turbinate reduction technique is considered the standard of care, but mucosal-sparing techniques are preferred to prevent atrophic rhinitis. Complete turbinate resection is to be avoided (risk of empty nose syndrome / paradoxical obstruction).
4. Tongue Base Reduction for OSA
RF coblation of the tongue base is a well-established minimally invasive treatment for obstructive sleep apnea (OSA) and snoring where bulky tongue base tissue is a contributing factor.
Technique: A needle-tip coblation probe is inserted into the tongue base musculature, near the foramen cecum. RF energy is delivered to create a controlled area of thermal coagulation necrosis within the muscle, which shrinks and fibroses during healing, reducing tongue base volume over subsequent weeks.
Key anatomical caution: The neuroascular bundle of the tongue is located 2.7 cm deep and 1.6 cm lateral to the foramen cecum - care must be taken to avoid this structure.
Evidence: A meta-analysis (Farrar et al., 2008) found RF surgery of the tongue base and soft palate results in a 45% reduction in long-term (>24 months) respiratory distress index (RDI). Results are comparable to other OSA procedures and morbidity is low. Treatment can be repeated for additional benefit - K.J. Lee's Essential Otolaryngology
5. Recurrent Respiratory Papillomatosis (RRP)
Coblation is used as an alternative to microdebrider and CO2 laser for debulking laryngeal and tracheal papillomata in juvenile-onset and adult RRP (JORRP/AORRP).
Advantages: Low thermal damage, potentially less scarring of the laryngeal mucosa compared to laser, and disposable wands reduce cross-infection risk.
Limitation: Evidence remains limited to mostly case reports and small retrospective series. In the UK, coblation accounted for only 3% of interventional RRP treatments. Specialist centres more commonly use microdebrider or KTP/pulsed dye laser. - Scott-Brown's Otorhinolaryngology, Vol. 2
6. Soft Palate Surgery / Uvulopalatoplasty (for Snoring and OSA)
Coblation uvulopalatoplasty and soft palate reduction are used as office-based or OR procedures for snoring/mild OSA. The wand reduces palatal bulk by submucosal ablation while preserving the mucosal surface, minimising the risk of velopharyngeal insufficiency compared to ablative techniques.
7. Other ENT Uses
- Head and neck tumor palliation: RF ablation for symptom control in unresectable tumors
- Microcystic lymphatic malformations: intralesional coblation ablation
- Nasal polyp debulking: adjunct to FESS
- Lingual tonsil reduction: in tongue base hypertrophy contributing to OSA
Coblation vs. Other Techniques: Summary Comparison
| Parameter | Cold Steel | Monopolar Electrocautery | Bipolar Diathermy | Coblation | Microdebrider | Harmonic Scalpel |
|---|---|---|---|---|---|---|
| Temperature | Ambient | >400°C | ~400°C | 40-70°C | Mechanical | ~80°C |
| Haemostasis | Poor (sutures needed) | Good | Good | Good | Poor | Good |
| Post-op pain | Moderate | High | Moderate-high | Low-moderate | Low | Low-moderate |
| Haemorrhage risk | Moderate | Low | Low | Low | Moderate | Low |
| Thermal spread | None | High | Moderate | Minimal | None | Moderate |
| Cost | Low | Low | Low | High (disposable wands) | High | High |
| Operating time | Moderate | Short | Moderate | Slightly longer | Moderate | Moderate |
Advantages of Coblation
- Low thermal tissue damage - no charring, minimal collateral injury
- Simultaneous ablation and haemostasis in a single instrument
- Mucosal preservation in submucosal applications (turbinates, tongue base, soft palate)
- Reduced post-operative pain compared to monopolar diathermy (though evidence is mixed vs. bipolar)
- Single-use wands eliminate cross-infection risk
- Versatile - multiple wand designs for tonsil, larynx, turbinate, tongue base, adenoids
- Can be used in office-based settings under local anaesthesia (turbinate reduction, tongue base)
Disadvantages / Limitations
- High unit cost of single-use wands - limits use especially for isolated adenoidectomy
- Longer operating time compared to electrocautery in some studies
- Evidence for pain advantage is mixed - not consistently proven superior to bipolar diathermy in meta-analyses
- Requires saline irrigation or gel at the tip for plasma generation - slightly more complex technique
- Post-tonsillectomy haemorrhage rate not demonstrably lower than other standard techniques
- Limited evidence for some applications (RRP, laryngeal use)
Key Points for Exams
- Coblation works via plasma-mediated molecular dissociation, not conventional heat transfer
- Operating temperature: 40-70°C (vs. ~400°C for conventional diathermy)
- Requires a conductive saline medium to generate the plasma field
- In tonsillectomy: comparable outcomes to other techniques; no definitive superiority for pain or haemorrhage
- In turbinate reduction: classified as mucosal preservation surgery - preferred over destructive techniques
- Tongue base coblation for OSA: ~45% reduction in RDI long-term
- Not to be confused with radiofrequency ablation (RFA) used in thyroid nodules/head-neck tumors - though the RF principle is shared, the mechanisms and applications differ
Sources: K.J. Lee's Essential Otolaryngology; Cummings Otolaryngology Head and Neck Surgery; Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vols 1 & 2; PMID 33719616 (meta-analysis, coblation vs. bipolar diathermy)
This is a shared conversation. Sign in to Orris to start your own chat.