Orchidectomy step by step for testicular infart
Reading File
Finding Sources
Finding Sources
Searching the Web
orchidectomy step by step surgical technique testicular infarct
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I have all the content needed. Here is the full step-by-step guide:
Simple (Scrotal) Orchidectomy for Testicular Infarct
Indication: A non-viable testis secondary to prolonged ischemia (testicular torsion, segmental infarct from vasculitis, trauma) where salvage is impossible. Simple orchidectomy via a scrotal approach is the standard - not a radical inguinal approach, which is reserved for suspected malignancy.
Pre-operative
- Consent: Include consent for unilateral orchidectomy and, if desired, simultaneous testicular prosthesis placement. Counsel the patient that the contralateral testis will also be explored and fixed (orchidopexy) if the cause was torsion.
- Anesthesia: General, spinal, or regional (spermatic cord block with sedation). A full spermatic cord block alone is rarely sufficient for an acutely inflamed/infarcted testis.
- Position: Supine, legs slightly abducted.
- Prep: Shave and sterile prep the scrotum and perineum.
Step-by-Step Technique
Step 1 - Skin Incision
Make a transverse hemiscrotal incision within the scrotal rugae over the affected side, avoiding prominent scrotal blood vessels. Alternatively, a vertical midline incision along the median raphe gives access to both sides through a single skin incision - useful if bilateral exploration is planned (e.g., after torsion).
Use diathermy on "cut" mode to incise, minimizing bleeding from scrotal skin vessels.
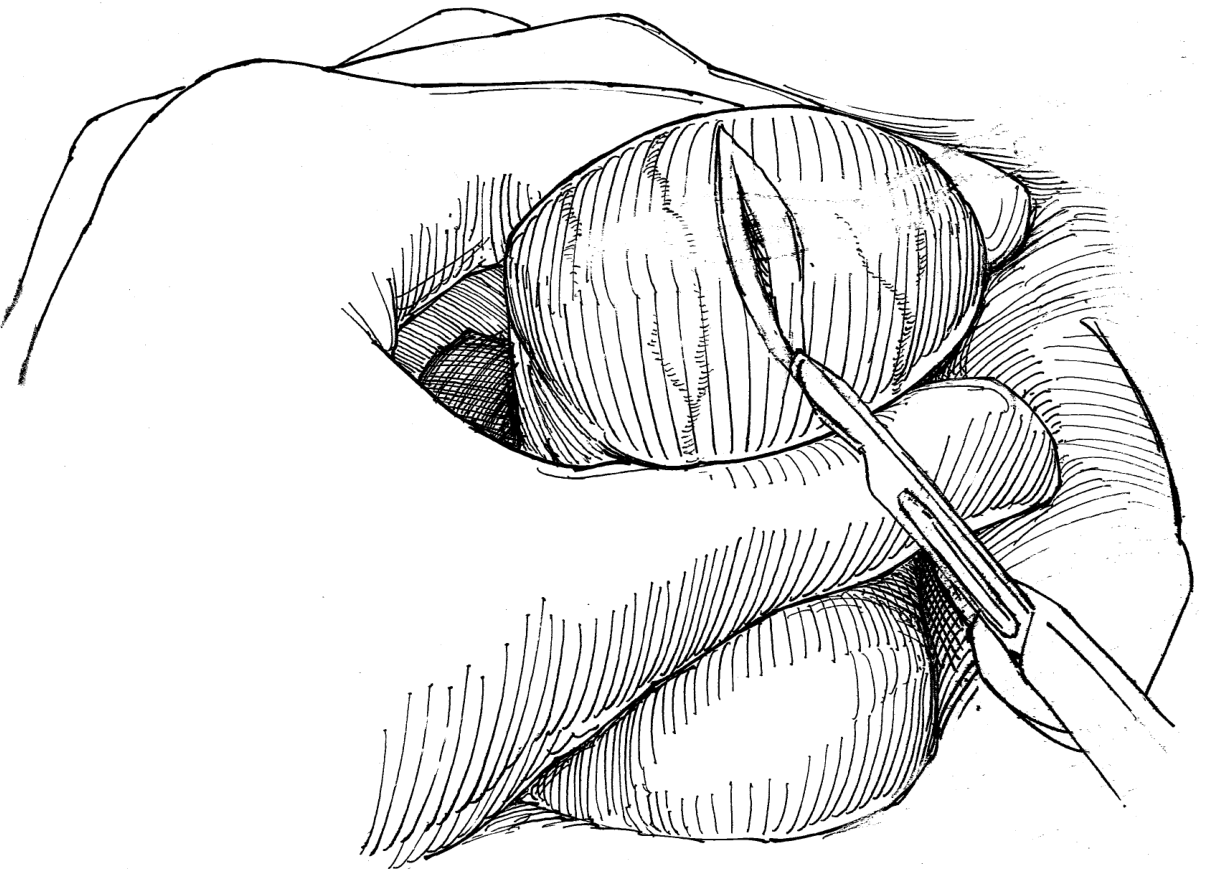
Step 2 - Layer-by-Layer Dissection and Testis Delivery
Carry the incision down through:
- Scrotal skin
- Dartos muscle/fascia
- Tunica vaginalis (open sharply)
Deliver the testis into the wound. Inspect it - an infarcted testis is typically dark blue/black, firm, and non-pulsatile when the tunica albuginea is nicked. Apply gentle traction on the testis to expose the spermatic cord.
Step 3 - Assess Viability
If any doubt exists about viability, nick the tunica albuginea and look for bleeding. A frankly necrotic, non-bleeding testis with no arterial pulsation confirms non-viability - proceed to orchidectomy. If there is any uncertainty and the patient is young, an on-table urological consult or intraoperative Doppler is appropriate before committing to removal.
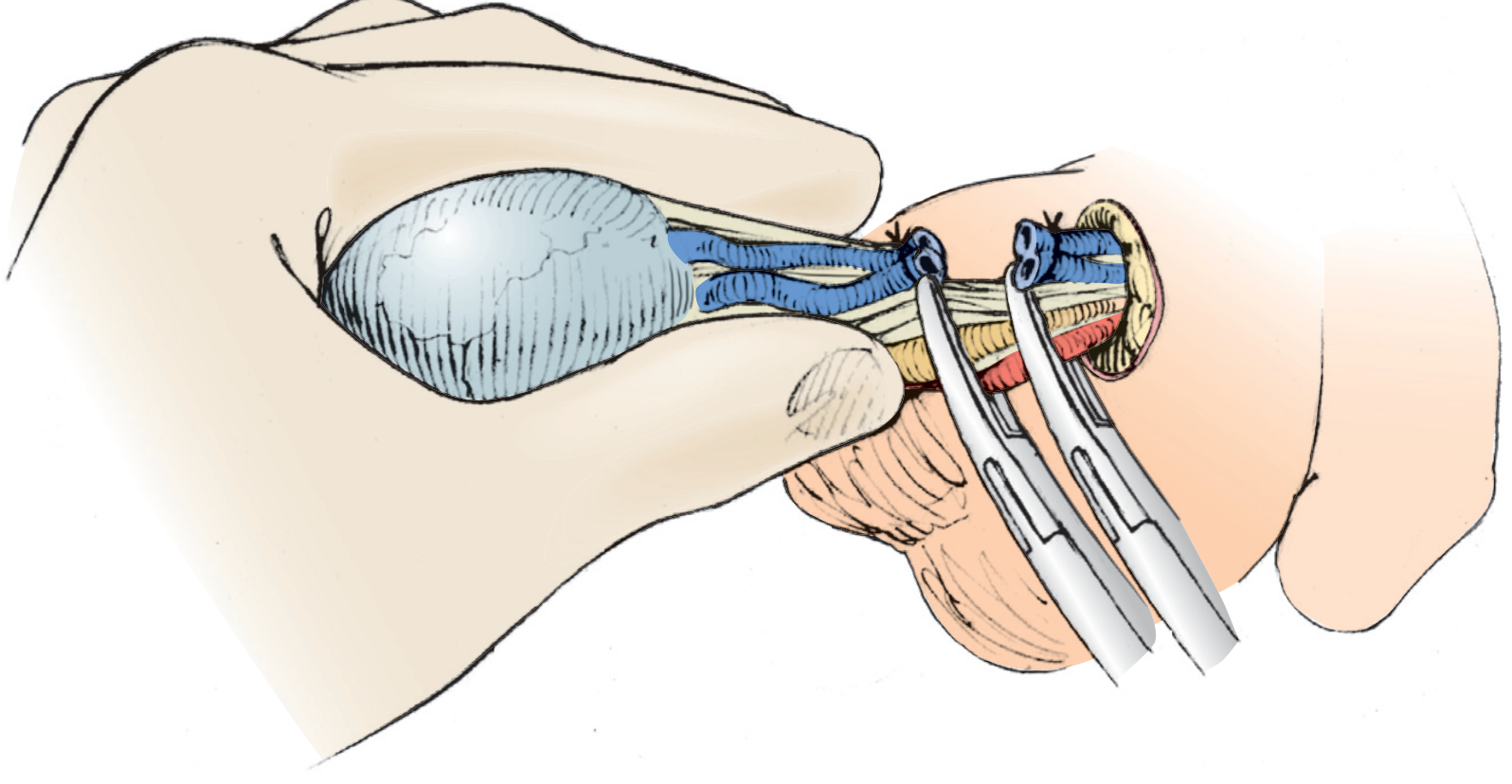
Step 4 - Separate and Ligate the Spermatic Cord
Separate the cord into two bundles:
Bundle 1 - Vas deferens:
- Double-clamp proximally, single clamp distally
- Divide sharply between the clamps
- Place a 2-0 Vicryl (or silk) tie proximally, release the first clamp, then place a 2-0 Vicryl suture-ligature distally
Bundle 2 - Internal spermatic vessels (cremasteric vessels):
- Identify and separate the cremasteric muscle from the internal spermatic vessels
- Ligate each component separately with 2-0 silk sutures
- Double-clamp proximal and single-clamp distal, divide, and suture-ligate
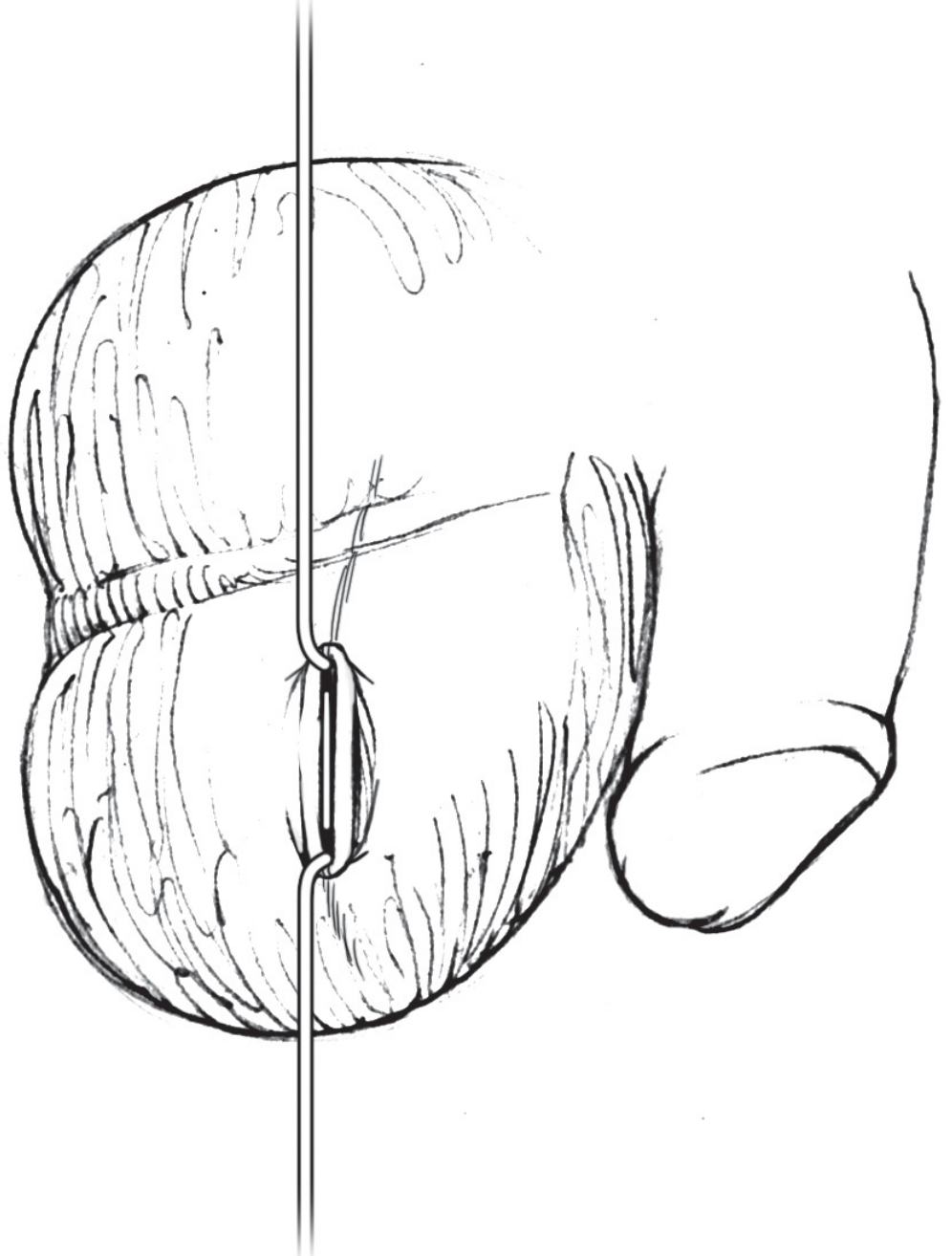
Step 5 - Remove the Testis
With both cord bundles ligated and divided, the testis and attached cord are free. Remove the specimen from the operative field and send it for histopathology (to exclude underlying tumour, which can present as infarction).
Step 6 - Haemostasis
Ensure meticulous haemostasis - inspect the cord stumps, the tunica vaginalis, and the dartos layer. Use electrocautery or additional ties as needed.
Step 7 - Optional Testicular Prosthesis
If the patient pre-operatively consented to a prosthesis, now is the time to insert it. Leave the gubernaculum and tunica vaginalis intact during the orchidectomy so the prosthesis can be placed inside the tunica vaginalis - this gives a natural position and appearance. The scrotal skin is inverted and the prosthesis is sutured to the dartos fascia internally to prevent high-riding.
Step 8 - Closure
- Dartos muscle - reapproximate with interrupted 3-0 or 4-0 absorbable suture (Vicryl)
- Local anaesthetic - inject wound with bupivacaine before skin closure
- Skin - close in a running subcuticular fashion with 5-0 absorbable suture (Monocryl or Vicryl), using skin hooks at the apices to aid closure. Alternatively, interrupted 4-0 chromic sutures
Step 9 - Contralateral Exploration (if torsion was the cause)
If the infarct was caused by testicular torsion, explore the contralateral testis through the same midline skin incision (or a separate transverse incision). Perform a three-point orchidopexy to prevent metachronous torsion on the remaining side, even if it appears normal.
Step 10 - Wound Dressing
Dress with antibiotic ointment, dry fluffed gauze, and an athletic supporter (scrotal support) to reduce edema and provide comfort.
Post-operative Care
| Item | Detail |
|---|---|
| Analgesia | Regular paracetamol + NSAID; opioids rarely needed |
| Scrotal support | Wear for 2-4 weeks |
| Activity | Avoid heavy lifting or straining for 2-3 weeks |
| Wound check | 7-10 days |
| Histology | Follow up results to exclude malignancy |
| Hormone status | Single testis is sufficient for normal testosterone; check if bilateral |
Key Decision Point: Simple vs Radical Orchiectomy
| Approach | When |
|---|---|
| Simple scrotal orchidectomy | Confirmed infarct/torsion, no suspicion of malignancy |
| Radical inguinal orchidectomy | Any suspicion of testicular malignancy - to avoid disrupting scrotal lymphatic drainage |
If there is any preoperative suspicion of tumour (solid mass, elevated AFP/beta-hCG, US findings), perform a radical inguinal approach instead. An infarcted testis can harbour an underlying germ cell tumour.
Sources: Hinman's Atlas of Urologic Surgery (Ch. 109, 116); Campbell-Walsh-Wein Urology (Ch. 83)
This is a shared conversation. Sign in to Orris to start your own chat.