Anesthetic concern for patient with pacemaker and icd in flowchart form
A detailed medical anesthesia flowchart titled "Anesthetic Concerns for Patient with Pacemaker / ICD (CIED)" with the following structure: TOP LEVEL: "Patient with CIED (Pacemaker / ICD) for Surgery" box Second level splits into 3 parallel boxes: - "Preoperative Assessment" - "Intraoperative Management" - "Postoperative Care" Under PREOPERATIVE ASSESSMENT, list: 1. Device identification: type, manufacturer, model, age, settings 2. Patient carries manufacturer ID card - note date of last interrogation 3. Assess underlying cardiac disease: HF, IHD, valvular disease, arrhythmias 4. Is patient pacemaker-dependent? (Yes/No branch) - YES → Program to asynchronous mode (DOO/VOO/AOO) preoperatively - NO → Monitor closely; magnet available 5. ICD present? → Deactivate antitachycardia function before surgery (reprogram or apply magnet) 6. Consult electrophysiologist / cardiologist before elective surgery 7. Note rate-modulation features that may malfunction with EMI Under INTRAOPERATIVE MANAGEMENT, list: EMI Sources: Monopolar electrocautery, RF ablation, lithotripsy, radiation therapy, guidewire movement Strategies: - Prefer BIPOLAR electrocautery - Place grounding pad FAR from device - Use SHORT bursts of cautery - External defibrillator pads applied and ready - Continuous pulse oximetry or arterial line for perfusion monitoring - ECG monitoring ICD-Specific Risks (box inside): 1. Cautery misread as VF → inappropriate shock 2. Inhibition of pacemaker function 3. Increased pacing rate (rate-responsive sensor) 4. Permanent reset to backup mode Pacemaker-Dependent Patient: → Asynchronous pacing mode programmed → Magnet available at all times Under POSTOPERATIVE CARE: 1. Restore and interrogate device immediately after surgery 2. Confirm all therapeutic functions restored 3. Continuous monitoring until antitachycardia functions confirmed active 4. Document any intraoperative events 5. Cardiology follow-up if device issues noted At bottom: WARNING BOX - "Unexpected ICD discharge during intracranial, spinal, or ocular surgery can cause CATASTROPHIC patient movement" Color coding: Blue for preoperative, Green for intraoperative, Orange for postoperative, Red for warnings. Clean professional medical flowchart style with clear arrows and boxes.
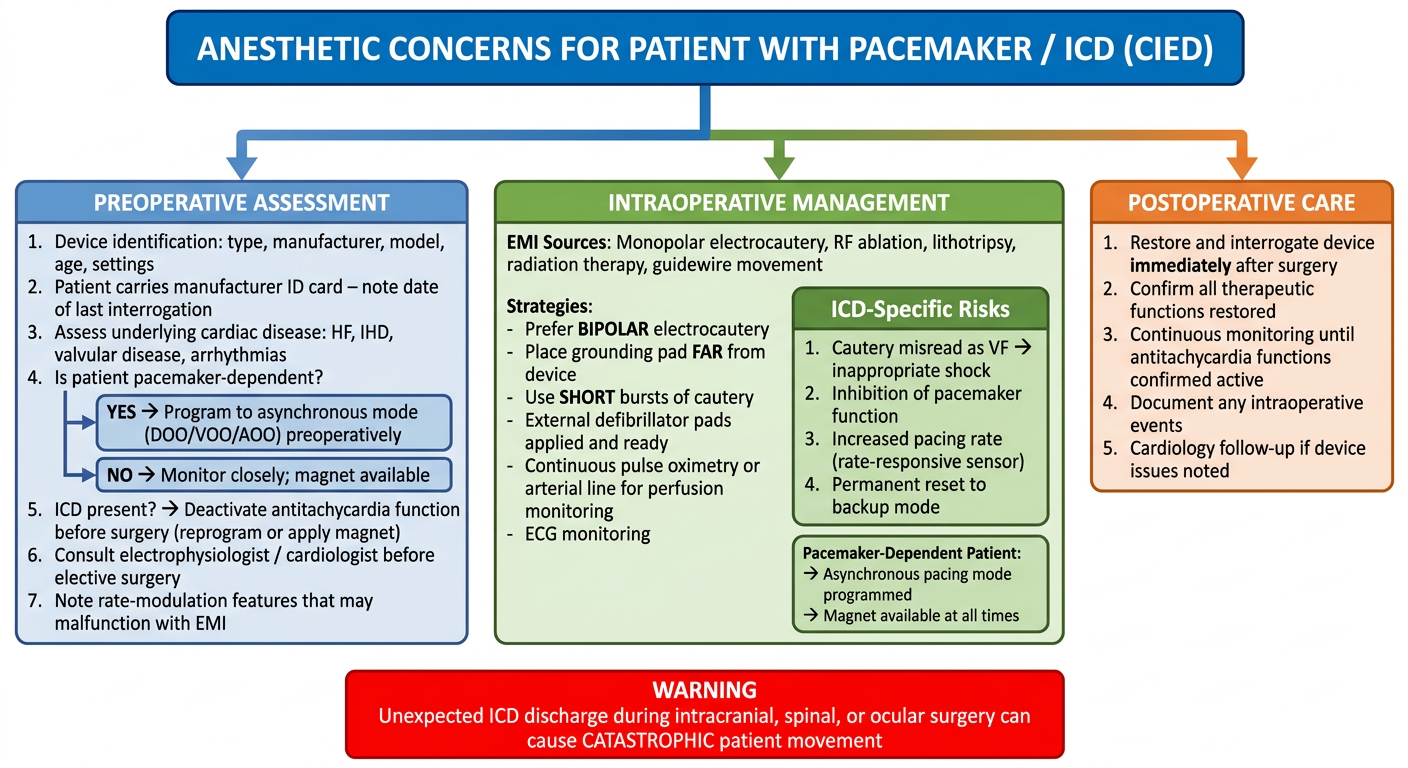
Anesthetic Concerns: Patient with Pacemaker / ICD (CIED)
PREOPERATIVE
- Type (pacemaker vs. ICD vs. CRT-D), manufacturer, model number, age, current settings
- Date of last interrogation (most devices should be checked within 6-12 months)
- Patient usually carries a manufacturer ID card - use it
- Call the manufacturer if needed for programming/magnet response details
- CIEDs are implanted for HF, IHD, valvular disease, or life-threatening arrhythmias - all carry independent perioperative risk
- Evaluate and optimize these comorbidities before elective surgery
- YES → Program to asynchronous mode (DOO/VOO/AOO) to prevent EMI-induced inhibition
- NO → Careful monitoring and magnet availability may suffice
- Antitachycardia function should be deactivated before surgery (especially if cautery will be used)
- Options: reprogram OFF or apply magnet (magnet suspends anti-tachycardia but does NOT convert to asynchronous pacing in most ICDs)
- Consult electrophysiologist / cardiologist
- Rate-responsive sensors (motion, minute ventilation) may trigger inappropriate pacing rate increases intraoperatively
INTRAOPERATIVE
| Source | Risk |
|---|---|
| Monopolar electrocautery | Highest risk - misread as VF, inhibits pacing |
| Radiofrequency ablation | Significant EMI |
| Lithotripsy devices | Can alter device settings |
| Radiation therapy | Potential device damage |
| Guidewire/CVC insertion | Direct mechanical interference with leads |
- Use bipolar cautery whenever possible
- Place dispersive (grounding) pad far from device
- Use short, intermittent cautery bursts (< 1 second)
- Avoid cautery in proximity to the device or leads
- Cautery artifact interpreted as VF → inappropriate defibrillation shock (patient movement risk)
- EMI inhibits pacemaker output → bradycardia / asystole
- Activation of rate-responsive sensor → inappropriate tachycardia
- Temporary or permanent reset to backup/factory mode
- Continuous pulse oximetry or arterial line (to detect perfusion loss during ECG artifact from cautery)
- ECG monitoring throughout
- External defibrillation pads applied and connected to a defibrillator before incision
POSTOPERATIVE
- Interrogate the device immediately after surgery to confirm all functions restored
- Continuously monitor patient until antitachycardia functions are confirmed active
- Document any intraoperative device-related events
- Cardiology follow-up if any device anomaly was noted
- Miller's Anesthesia, 10e - Chapter 28 (Cardiovascular Implantable Electronic Devices, p. 3934-3935)
- Morgan & Mikhail's Clinical Anesthesiology, 7e - p. 749-751
Management of a 18 year old girl with 4 cm endometrioma -take references from asrm guidelines and williams and novacks gyane
ASRM guidelines endometrioma management 2022 2023 2024
https://integration.asrm.org/practice-guidance/practice-comm…
endometrioma adolescent management surgery ovarian reserve
endometrioma surgery ovarian reserve AMH
A detailed clinical management flowchart titled "Management of 18-Year-Old Girl with 4 cm Endometrioma" with the following hierarchical structure: START BOX (top center, large): "18-year-old female | 4 cm ovarian endometrioma on ultrasound" STEP 1 - INITIAL ASSESSMENT (blue box): "Initial Clinical Assessment" - History: Dysmenorrhea, dyspareunia, pelvic pain, bowel/bladder symptoms, family history - Examination: Pelvic exam, adnexal tenderness, nodularity - Investigations: Transvaginal/transabdominal USS, CA-125, AMH (baseline ovarian reserve), CBC Arrow leads to STEP 2 - KEY DECISION (yellow diamond): "Is there indication for surgery?" (Pain uncontrolled by medical therapy? Suspected malignancy? Cyst >4 cm? Fertility concerns?) LEFT BRANCH from diamond (NO / Mild symptoms, no malignancy concern): Box: "Medical Management (First-line in Young Patient)" - NSAIDs for dysmenorrhea - Combined oral contraceptive pills (continuous or cyclic) - Progestins (dienogest, DMPA) - GnRH agonists (short-term; add-back therapy if >6 months - CAUTION in adolescents - bone density) - Regular follow-up USS every 3-6 months - Monitor cyst size change RIGHT BRANCH from diamond (YES - Surgery indicated): Box: "Surgical Management" Sub-point: "Preferred: LAPAROSCOPIC CYSTECTOMY (excision of cyst wall)" - Advantages over drainage+ablation: * Lower recurrence rate (OR 0.41) * Better pain relief (dysmenorrhea OR 0.15) * Higher spontaneous pregnancy rate (OR 5.21) * Histologic confirmation - Technique: Aspirate → incise → strip cyst wall from ovarian cortex - MAXIMIZE PRESERVATION of normal ovarian tissue - Hemostasis: prefer suture over bipolar coagulation (protects ovarian reserve) WARNING BOX (red): "OVARIAN RESERVE CONCERN in Young Patient" - AMH drops post-cystectomy (3.9 → 2.9 ng/mL at 6 months) - Risk of inadvertent removal of normal ovarian follicles - Counsel patient and parents pre-op about fertility risk - Consider fertility preservation / oocyte cryopreservation if high risk STEP 3 - POSTOPERATIVE MANAGEMENT (green box): "Post-Surgical Management - KEY in Adolescent" - Histopathology of excised cyst wall (confirm endometrioma) - Hormonal suppression to prevent recurrence: * Combined OCP (preferred in adolescent) * Dienogest 2 mg/day * Continue for 18-24 months minimum (ESHRE/ASRM) - Repeat USS at 3-6 months post-op - AMH reassessment at 6 months BOTTOM BOX (purple) - SPECIAL CONSIDERATIONS FOR ADOLESCENTS: - Avoid GnRH agonists as long-term therapy (bone density risk in adolescents) - Avoid oophorectomy / BSO (radical surgery contraindicated in 18-year-old) - Multidisciplinary approach: Gynecologist + Reproductive endocrinologist + Pain specialist - Psychological support / counseling - ASRM: Long-term OCP post-cystectomy reduces recurrence risk - Berek & Novak: Women aged ≤30 at hysterectomy report more residual symptoms - conservative approach essential BOTTOM RIGHT BOX (orange): "Recurrence / Refractory" - If recurrence: consider repeat laparoscopic cystectomy or prolonged medical suppression - IVF if future infertility (do NOT repeat surgery without benefit analysis - risk of diminishing ovarian reserve) - Discuss long-term plan for definitive surgery only if family complete Use color-coding: blue for assessment, yellow for decision diamonds, green for post-op, red for warnings, purple for special adolescent notes, orange for recurrence. Professional medical flowchart with clear directional arrows, clean layout, well-spaced boxes.
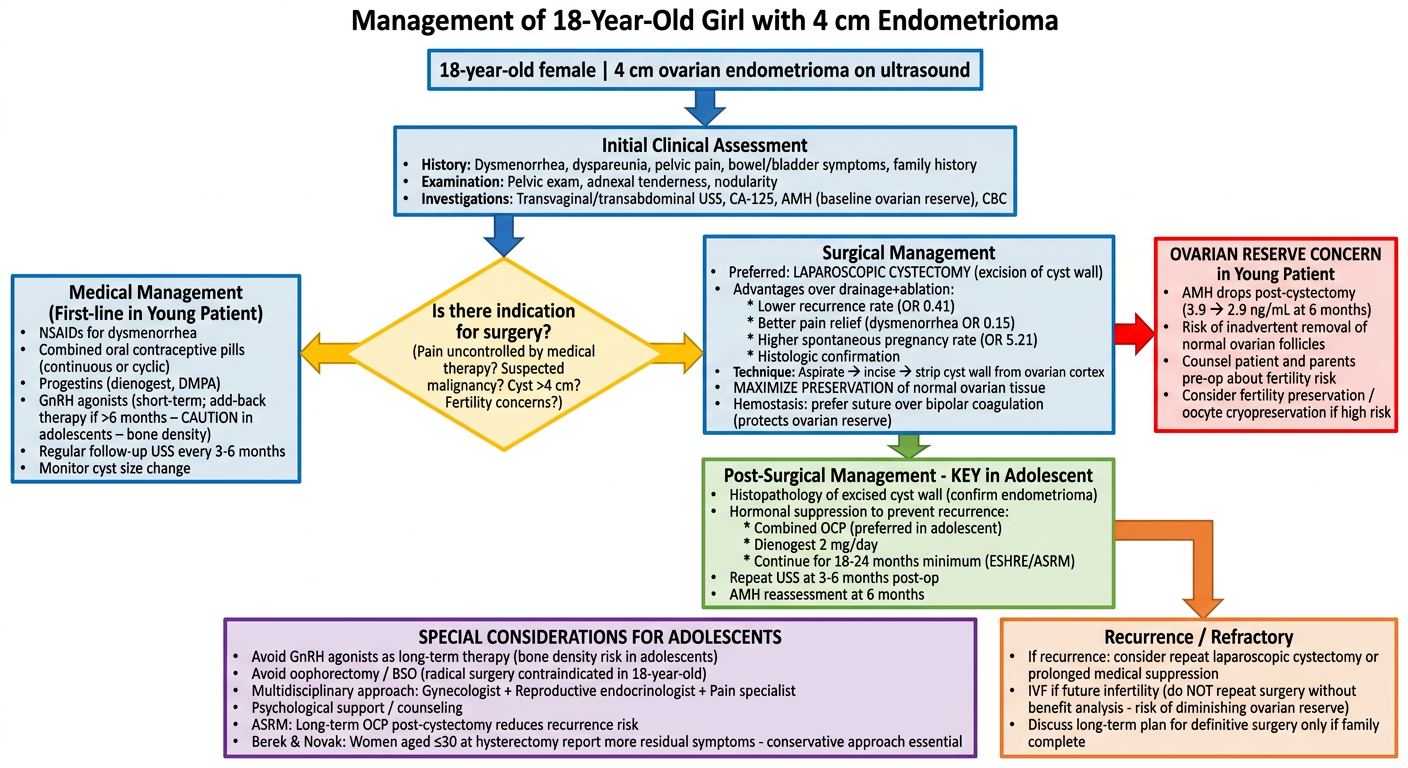
Management of an 18-Year-Old with a 4 cm Endometrioma
STEP 1: Initial Assessment
- Dysmenorrhea, dyspareunia, chronic pelvic pain, dyschezia, dysuria
- Family history of endometriosis
- Menstrual pattern, sexual/reproductive history
- Pelvic exam: uterosacral nodularity, adnexal tenderness/mass
- Abdominal examination
- Transvaginal/transabdominal ultrasound (confirm 4 cm endometrioma - ground-glass echogenicity, homogeneous low-level internal echoes)
- AMH (baseline ovarian reserve) - essential before any intervention in a young patient
- CA-125 (elevated in endometriosis, also excludes malignancy)
- CBC, inflammatory markers
STEP 2: Surgical vs Medical Decision
Indications for Surgery (at 4 cm)
- Cyst ≥3-4 cm with surgical threshold met
- Symptoms refractory to medical therapy
- Suspicion of malignancy (warrant histology)
- Desire for fertility evaluation
Medical Management (First-Line in Adolescent - Even with 4 cm Cyst)
| Drug | Notes |
|---|---|
| NSAIDs | First-line for dysmenorrhea (Berek & Novak) |
| Combined OCP (continuous preferred) | Reduces pain, slows progression, reduces recurrence |
| Progestins - Dienogest 2 mg/day | Highly effective for endometriosis-associated pain |
| GnRH agonists (short-term only) | Effective but risks bone loss in adolescents; must use add-back therapy; NOT recommended long-term in this age group |
ASRM: GnRH agonist is not recommended as first-line because it is more expensive and associated with more side effects and bone density concerns than OCPs. - Berek & Novak's Gynecology (p. 664)
STEP 3: If Surgery is Needed
Approach: Laparoscopic Cystectomy (Excision of Cyst Wall)
"According to a systematic review, there is good evidence that excisional surgery for endometriomas with a diameter of 3 cm provides a more favorable outcome than drainage and ablation with regard to the recurrence of the endometrioma, recurrence of pain symptoms, and in women who were previously subfertile."
- Berek & Novak's Gynecology, p. 656
| Outcome | Cystectomy Advantage |
|---|---|
| Recurrence of dysmenorrhea | OR 0.15 (95% CI 0.06-0.38) |
| Recurrence of dyspareunia | OR 0.08 (95% CI 0.01-0.51) |
| Endometrioma recurrence | OR 0.41 (95% CI 0.18-0.93) |
| Need for reoperation | OR 0.21 (95% CI 0.05-0.79) |
| Spontaneous pregnancy rate | OR 5.21 (95% CI 2.04-13.29) |
- Aspirate cyst → incise wall → strip cyst wall from ovarian cortex
- Maximize preservation of normal ovarian tissue - critical in an 18-year-old
- For hemostasis: prefer suturing over bipolar coagulation - bipolar coagulation causes more thermal damage to primordial follicles
- Send specimen for histopathology
CRITICAL CONCERN: Ovarian Reserve
"Cystectomy and ablation of an endometrioma carry potential risks for the ovarian reserve, either by removal of normal ovarian tissue during excision or by thermal damage to the ovarian cortex during ablation. Although as little as one-tenth of an ovary may be enough to preserve function and fertility, there is concern that ovarian cystectomy with concomitant removal or destruction of normal ovarian tissue may reduce ovarian follicle reserve."
- Berek & Novak's Gynecology, p. 680
- AMH drops from ~3.9 to 2.9 ng/mL at 6 months post-cystectomy (vs. minimal drop with three-stage procedure)
- Counsel patient and guardian pre-operatively about fertility risk
- Consider oocyte/embryo cryopreservation before surgery if the patient requests it
- Recent meta-analyses (PMID: 36334993, 38509401) confirm cystectomy reduces AMH more than ablation in the short term, but provides better long-term outcomes
STEP 4: Post-Operative Management
"The ESHRE guideline recommends the use of postoperative hormonal therapy... after cystectomy for an endometrioma in women not immediately seeking conception... for at least 18 to 24 months, for secondary prevention."
- Berek & Novak's Gynecology, p. 663
- Combined OCP - preferred in adolescents (bone density safe, contraceptive benefit)
- Dienogest 2 mg/day as alternative
- Duration: minimum 18-24 months
- Repeat ultrasound at 3-6 months
- AMH reassessment at 6 months post-op
- Annual review of symptoms and recurrence
Special Adolescent Considerations
| Principle | Rationale |
|---|---|
| Avoid long-term GnRH agonists | Bone density loss during peak bone accrual years (age 18) |
| Avoid oophorectomy/BSO | Radical surgery is contraindicated in an 18-year-old |
| Prefer laparoscopy over laparotomy | Less adhesion formation, faster recovery, better cosmesis |
| Multidisciplinary team | Gynecology + Reproductive endocrinology + Pain specialist + Psychologist |
| Recurrence planning | If cyst recurs, weigh benefit vs. diminishing ovarian reserve before reoperation |
"Women aged 30 years or younger at the time of hysterectomy for endometriosis-associated pain are more likely than older women to have residual symptoms, to report a sense of loss... bilateral salpingo-oophorectomy in young women should be considered in only the most severe or recurrent cases."
- Berek & Novak's Gynecology, p. 663
References
- Berek & Novak's Gynecology (16th ed.) - Ovarian Endometriosis, pp. 656-681
- ASRM Practice Committee - Endometriosis and Infertility: A Committee Opinion (2012) - Surgery for Endometriomas; Postoperative Hormonal Suppression
- Zhang Y et al. (2022) - Impact of cystectomy versus ablation for endometrioma on ovarian reserve: a systematic review and meta-analysis. Fertil Steril. [PMID: 36334993]
- Paik H, Jee BC (2024) - Impact of Ablation Versus Cystectomy for Endometrioma on Ovarian Reserve, Recurrence, and Pregnancy: An Updated Meta-Analysis. Reprod Sci. [PMID: 38509401]
- Moreno-Sepulveda J et al. (2022) - Effect of Laparoscopic Endometrioma Surgery on AMH: Meta-Analysis. JBRA Assist Reprod. [PMID: 34755503]
Describe the pathogenesis of borderline ovarian tumor. c) Discuss the management of a 30-year-old Para 2 detected post operatively as borderline mucinous ovarian tumor on histopathological examination after laparoscopic unilateral ovarian cystectomy done 2 weeks back for ovarian cyst."- for dnb exam paper,explain in simple flowcharts taking reference from -gynae williams and gyane