Estrogen vs progesterone
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
I now have rich, comprehensive material from multiple authoritative textbooks. Here is the full comparison:
Estrogen vs Progesterone
Both are ovarian steroid hormones derived from cholesterol, working in a coordinated and sometimes opposing fashion across the female reproductive cycle and beyond.
1. Biosynthesis
Both are synthesized by the ovarian follicles through the combined action of theca cells and granulosa cells:
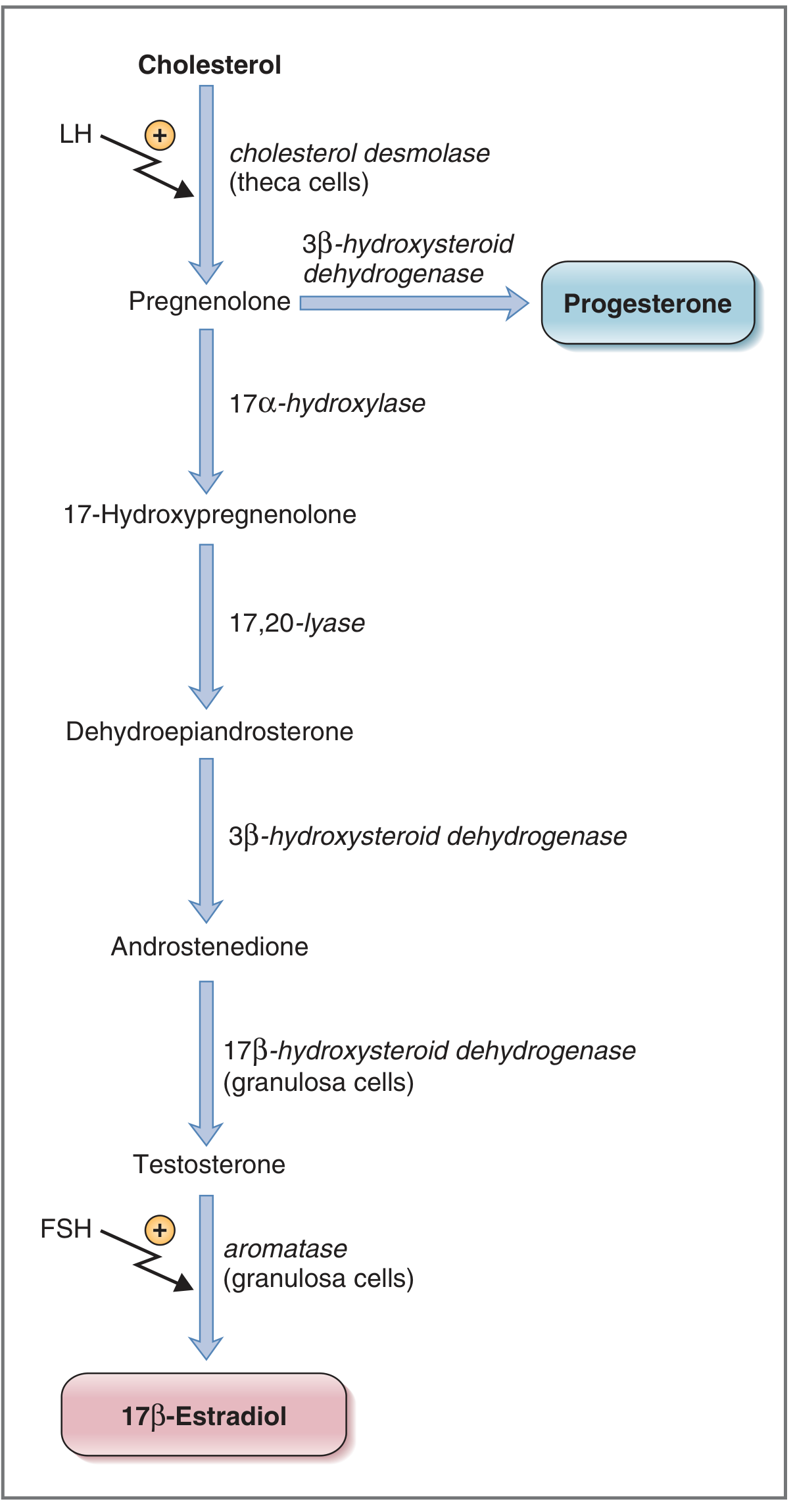
- Progesterone: Pregnenolone → Progesterone (via 3β-hydroxysteroid dehydrogenase) in theca cells. LH stimulates cholesterol desmolase, the first step.
- Estrogen (17β-Estradiol): Theca cells synthesize androstenedione → diffuses to granulosa cells → converted to testosterone → then aromatized to 17β-estradiol by aromatase. FSH stimulates aromatase, the final step.
Source: Costanzo Physiology 7th Edition
The three biologically active estrogens are estradiol (E2), estrone (E1), and estriol (E3), with E2 being the major secretory product of the ovaries.
2. Receptors & Mechanism of Action
| Feature | Estrogen | Progesterone |
|---|---|---|
| Receptor type | ERα, ERβ (nuclear, distinct anatomical distributions) | PR-A, PR-B (nuclear) |
| Receptor regulation | Up-regulates its own receptors AND progesterone receptors | Down-regulates estrogen receptors in some tissues |
| Key principle | Must prime target tissues first | Requires prior estrogen exposure to act; biologically inactive without it |
Estrogen up-regulates progesterone receptors - this means estrogen must act first before progesterone can exert its effects. Without this estrogen priming, progesterone has little biological activity.
3. Actions: A Side-by-Side Comparison
Uterus
| Tissue | Estrogen | Progesterone |
|---|---|---|
| Endometrium | Proliferative - stimulates cell growth and thickening | Secretory - stimulates glandular secretion, prepares for implantation |
| Contractility | Increases contractility (lowers threshold to stimuli) | Decreases contractility (raises threshold) - protects pregnancy |
| Cervical mucus | Increases quantity, makes it watery and penetrable by sperm (around ovulation) | Makes mucus less abundant and thicker - hostile to sperm |
Fallopian Tubes
- Estrogen: Stimulates ciliary activity and contractility - helps move sperm toward the uterus
- Progesterone: Increases secretory activity, decreases contractility
Vagina
- Estrogen: Stimulates proliferation of epithelial cells
- Progesterone: Stimulates differentiation but inhibits proliferation
Breasts
Both are required for breast development. Estrogen is specifically required for ductal development; progesterone for lobular-alveolar development. Notably, estrogen blocks the action of prolactin on the breast (paradoxically, despite stimulating prolactin secretion).
4. Summary of Target Tissue Actions
Estrogen Actions (Table 10.2, Costanzo):
- Maturation of uterus, fallopian tubes, cervix, vagina
- Development of female secondary sex characteristics at puberty
- Proliferation of ovarian granulosa cells
- Up-regulation of estrogen, progesterone, and LH receptors
- Negative and positive feedback on FSH/LH (negative throughout most of cycle; positive feedback triggers the LH surge at ovulation)
- Stimulation of prolactin secretion
- Decreases LDL cholesterol - cardioprotective
- Anti-osteoporosis effect (inhibits bone resorption)
- Pubertal growth spurt and epiphyseal closure
- Subcutaneous fat deposition (female fat distribution)
Progesterone Actions (Table 10.3, Costanzo):
- Maintains secretory endometrium during the luteal phase
- Development of breasts
- Negative feedback on FSH/LH (but no positive feedback)
- Maintenance of pregnancy
- Raises uterine threshold to contractile stimuli during pregnancy
- Thermogenic - increases basal body temperature in the luteal phase (basis of the "rhythm method")
5. Role in the Menstrual Cycle
| Phase | Dominant Hormone | Key Events |
|---|---|---|
| Follicular (days 0-14) | Estrogen | Endometrial proliferation; negative feedback → at peak, positive feedback triggers LH/FSH surge |
| Ovulation (day 14) | Estrogen peak | Cervical mucus becomes watery; LH surge triggers ovum release |
| Luteal (days 14-28) | Progesterone + Estrogen | Secretory endometrium; BBT rises; thick cervical mucus; prepares for implantation |
| Late luteal (if no pregnancy) | Both fall | Corpus luteum degenerates; endometrium shed (menstruation) |
The luteal phase is constant at ~14 days; variability in cycle length comes from the follicular phase.
6. CNS and Psychiatric Effects
From Kaplan & Sadock's Psychiatry:
Estrogen:
- Mood-enhancing; increases serotonin sensitivity (possibly by inhibiting MAO)
- Lower estrogen levels associated with acute psychosis and worse cognition
- May delay onset of Alzheimer's dementia in postmenopausal women
- Enhances dopamine synthesis and release
- Modulates spatial cognition and verbal memory
Progesterone:
- Progesterone itself may be anxiogenic
- Its metabolites (allopregnanolone, pregnenolone) are anxiolytic and hypnotic via GABA-A agonism
- Co-localized with serotonin in median raphe cells; increases serotonin uptake and turnover
- Has anti-estrogen effects in the CNS
7. Key Opposing Effects (Head-to-Head)
| Parameter | Estrogen | Progesterone |
|---|---|---|
| Endometrium | Proliferation | Secretion |
| Uterine contractility | Increases | Decreases |
| Cervical mucus | Watery, copious | Thick, scant |
| Body temperature | No effect | Raises BBT |
| LH/FSH feedback | Negative AND positive | Negative only |
| Estrogen receptors | Up-regulates | Down-regulates |
| Progesterone receptors | Up-regulates | - |
| Vaginal epithelium | Proliferates | Differentiates, inhibits proliferation |
| Mood | Antidepressant, anxiolytic | Anxiogenic (but metabolites are anxiolytic) |
8. Clinical Relevance
- Hormone receptor status in cancer: ER (estrogen receptor) and PR (progesterone receptor) positivity in breast and endometrial cancer are favorable prognostic markers; these tumors respond to endocrine therapy (e.g., tamoxifen, aromatase inhibitors). - Goldman-Cecil Medicine, Schwartz's Surgery
- Endometriosis treatment: Targets both receptors - progestins, progesterone antagonists/SPRMs, SERMs, aromatase inhibitors are all used. - Berek & Novak's Gynecology
- HRT: Unopposed estrogen causes endometrial hyperplasia; progesterone is added to protect the endometrium
- Contraception: Combined OCP suppresses ovarian hormone synthesis and increases SHBG
Sources: Costanzo Physiology 7th Ed. | Kaplan & Sadock's Comprehensive Textbook of Psychiatry | Katzung's Basic and Clinical Pharmacology 16th Ed. | Goldman-Cecil Medicine | Berek & Novak's Gynecology | Schwartz's Principles of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.