ReCode classification of still birth
Reading File
Finding Sources
Searching the Web
ReCoDe classification stillbirth categories groups
Finding Sources
Reading Web Page
https://www.pi.nhs.uk/pnm/ReCoDe_Classification.pdf
Here is a complete breakdown of the ReCoDe (Relevant Condition at Death) Classification for stillbirth, developed by Gardosi et al. (Perinatal Institute, UK, 2005):
ReCoDe Classification of Stillbirth
ReCoDe identifies the condition(s) present at the time of intrauterine death, rather than trying to assign a single cause. The system uses anatomical groups (A through I) in a hierarchy that moves from fetus outward.
Guiding Principles
- Stillbirths are distinct from neonatal deaths and warrant their own classification.
- No sub-classification by gestation - "prematurity" is not a relevant cause for stillbirths.
- No sub-classification by weight, but fetal growth status (weight-for-gestation) is used.
- The classification emphasizes what went wrong, not necessarily why - so more than one category can be coded.
- The hierarchy starts from conditions affecting the fetus and moves outward through anatomical categories (A-F), then intrapartum events, trauma, and unclassified.
- The primary condition should be the highest on the list that applies to the case.
Groups and Sub-categories
| Group | Category | Sub-conditions |
|---|---|---|
| A | Fetus | 1. Lethal congenital anomaly |
| 2. Infection - 2.1 Chronic (e.g. TORCH), 2.2 Acute | ||
| 3. Non-immune hydrops | ||
| 4. Iso-immunisation | ||
| 5. Fetomaternal haemorrhage | ||
| 6. Twin-twin transfusion | ||
| 7. Fetal growth restriction ¹ | ||
| 8. Other | ||
| B | Umbilical Cord | 1. Prolapse |
| 2. Constricting loop or knot ² | ||
| 3. Velamentous insertion | ||
| 4. Other | ||
| C | Placenta | 1. Abruptio |
| 2. Praevia | ||
| 3. Vasa praevia | ||
| 4. Placental insufficiency/infarction ³ | ||
| 5. Other | ||
| D | Amniotic fluid | 1. Chorioamnionitis |
| 2. Oligohydramnios ² | ||
| 3. Polyhydramnios ² | ||
| 4. Other | ||
| E | Uterus | 1. Rupture |
| 2. Other | ||
| F | Mother | 1. Diabetes |
| 2. Thyroid diseases | ||
| 3. Essential hypertension | ||
| 4. Hypertensive diseases in pregnancy | ||
| 5. Lupus / Antiphospholipid syndrome | ||
| 6. Cholestasis | ||
| 7. Drug abuse | ||
| 8. Other | ||
| G | Intrapartum | 1. Asphyxia |
| 2. Birth trauma | ||
| H | Trauma | 1. External |
| 2. Iatrogenic | ||
| I | Unclassified | 1. No relevant condition identified |
| 2. No information available |
Footnotes
- ¹ Fetal growth restriction: Defined as birth weight < 10th customized weight-for-gestation centile (using the customized centile calculator at gestation.net).
- ² Constricting loop/knot, oligohydramnios, polyhydramnios: Only coded if severe enough to be considered relevant.
- ³ Placental insufficiency/infarction: Requires histological diagnosis.
Why ReCoDe Was Developed
The older Wigglesworth classification left ~66% of stillbirths as "unexplained." ReCoDe reduced this to only ~15% unexplained by:
- Introducing fetal growth restriction (FGR) as a distinct category - this alone accounted for 43% of stillbirths as the most common condition.
- Of 1738 "unexplained" Wigglesworth cases, ReCoDe identified 57.7% as growth restricted.
- It allows coding of multiple conditions (primary + secondary), giving a fuller clinical picture.
Key Advantage Over Other Systems
| Feature | Wigglesworth | ReCoDe |
|---|---|---|
| Unexplained % | ~66% | ~15% |
| FGR as a category | No | Yes (A7) |
| Multiple conditions | No | Yes |
| Gestational age sub-classification | Yes | No (not needed for stillbirths) |
| Based on customized growth norms | No | Yes |
The original paper is by Gardosi et al., BMJ 2005 (cited over 749 times), and the full classification reference is available from the Perinatal Institute.
How to diagnose placenta previa on TVS
Finding Sources
Finding Sources
Searching the Web
placenta previa diagnosis transvaginal ultrasound TVS criteria distance internal os
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading Web Page
https://www.contemporaryobgyn.net/view/placenta-previa-pract…
Loading Image
Here is a comprehensive guide to diagnosing placenta previa on TVS (transvaginal sonography), based on Creasy & Resnik's Maternal-Fetal Medicine and current guidelines.
Diagnosis of Placenta Previa on Transvaginal Sonography (TVS)
Why TVS over Transabdominal Ultrasound (TAS)?
- TAS overdiagnoses low-lying placenta and placenta previa, especially with an empty bladder (the distended posterior bladder wall can mimic a low-lying placenta).
- TVS is the gold standard for definitive placental localization - it is more accurate, safe, and reproducible.
- Concerns about TVS provoking bleeding are unfounded; multiple studies confirm its safety.
- If TVS is unavailable, translabial (transperineal) ultrasound is a valid alternative.
TVS Technique
- Insert the probe under continuous ultrasound visualization on the monitor - never insert blindly.
- Avoid placing the probe into a potentially dilated cervix.
- The probe need only be inserted 2-3 cm into the vagina; the cervix and lower uterine segment are in the near field.
- Identify the internal cervical os clearly in the sagittal plane.
- Measure the distance from the inferior placental edge to the internal os in millimeters.
- Apply color Doppler if vasa previa is suspected (to distinguish fetal vessels from placental edge).
Diagnostic Criteria (Current Multisociety Consensus - 2014)
| Finding | Distance from Placental Edge to Internal Os | Diagnosis |
|---|---|---|
| Placenta covers the internal os | Overlap (negative distance) | Placenta Previa |
| Placental edge within 2 cm of os but not covering | 0 to 20 mm | Low-lying Placenta |
| Placental edge beyond 2 cm from os | > 20 mm | Normal position |
- The old classification (complete, partial, marginal, low-lying previa) has been abandoned in favor of this two-category system: placenta previa vs low-lying placenta.
- A low-lying placenta with a placental edge-to-os distance of < 10 mm in the third trimester is associated with a very high likelihood of cesarean delivery.
- > 10 mm distance: vaginal delivery may be considered; management should be individualized.
TVS Image: TAS vs TVS Comparison
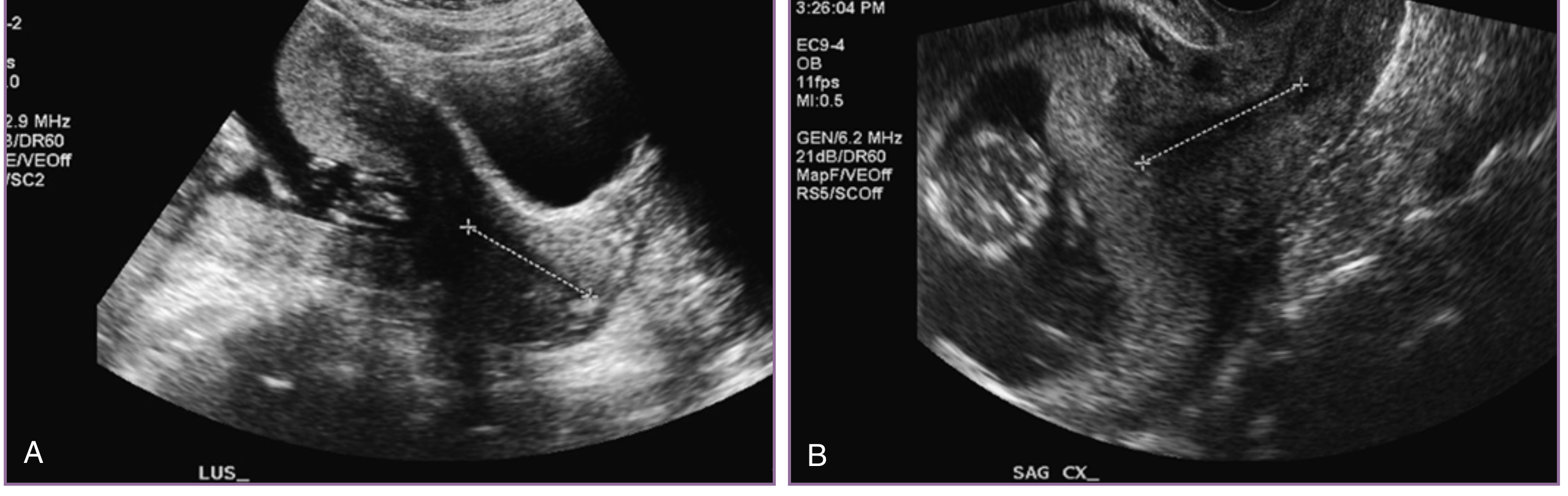
Figure: (A) Transabdominal ultrasound at 18 weeks shows an apparent "low-lying placenta." (B) TVS of the same patient confirms the placenta completely covers the cervix - demonstrating why TVS is required for definitive diagnosis. - Creasy & Resnik's Maternal-Fetal Medicine
What to Measure and Report on TVS
- The distance in millimeters from the leading (inferior) edge of the placenta to the internal os.
- If the placenta overlaps the os, report the degree of overlap in mm.
- Include assessment for a marginal sinus (which should be included in the measurement).
- Note the placental location (anterior/posterior).
- Assess for placenta accreta spectrum (PAS): look for loss of the retroplacental clear zone, placental lacunae, and bulging of placenta toward the bladder - especially in women with prior uterine scars.
When to Diagnose and Follow Up
| Timing | Action |
|---|---|
| < 16 weeks | Do not label as previa - placental migration is expected |
| 16-20 weeks (routine anomaly scan) | Screen; report distance to os |
| Second trimester (if low-lying/previa) | Follow-up TVS at 32 weeks |
| 32 weeks - previa persists | Repeat TVS at 34-36 weeks before finalizing delivery route |
| > 36 weeks, previa confirmed | Plan cesarean delivery |
Key facts about migration:
- Up to 90-98% of low-lying placentas detected in the second trimester resolve by the third trimester.
- The placenta "migrates" at approximately 5.4 mm/week as the lower uterine segment expands.
- The likelihood of persistence to term is related to degree of overlap and thickness of the placental edge at the os.
- An anterior placenta overlapping by up to 4.5 mm in the second trimester is likely to resolve; posterior placentas with an internal os distance > 15.5 mm in the second trimester are very unlikely to persist as previa.
Important Safety Rules
- Never perform digital or speculum examination until placenta previa is excluded by ultrasound.
- In an emergency without ultrasound, the old "double setup" examination is still valid - done in the operating room with cesarean capability immediately available.
- All women with painless vaginal bleeding after 20 weeks must be assumed to have placenta previa until proven otherwise.
Sources: Creasy & Resnik's Maternal-Fetal Medicine, 8th ed., Chapter 43; Multisociety Fetal Imaging Forum 2014 guidelines; BCM clinical protocol on placenta previa and vasa previa
This is a shared conversation. Sign in to Orris to start your own chat.