Explain the lymphatic drainage of breast in details and how it relates to the spread of breast cancer
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full detailed answer.
Lymphatic Drainage of the Breast - Detailed Overview and Relation to Breast Cancer Spread
1. Overview of the Lymphatic System of the Breast
The breast has a rich lymphatic network that can be divided into three functional layers:
- Superficial (cutaneous) system - drains the skin overlying the breast
- Subcutaneous system - drains the subcutaneous tissue
- Deep parenchymal system - originates at the acinar (lobular) level and travels along the ducts; this is the route most relevant to tumor metastasis
Lymph from the nipple, areola, lobules, and stroma converges centrally into the subareolar lymphatic plexus (also called the Sappey plexus, described by the anatomist Sappey in 1874/1885). From this plexus, lymph is propelled outward along several drainage routes.
- Fischer's Mastery of Surgery, 8th ed., p.1396
- Sabiston Textbook of Surgery, p.1748
2. Primary Drainage Routes
A. Axillary Route (Major - ~75%)
Approximately 75-80% of all breast lymphatic drainage flows laterally and superiorly into the axillary lymph nodes. This is the dominant and clinically most important route.
The flow path is:
Subareolar plexus → external mammary (anterior/pectoral) nodes → deeper axillary levels
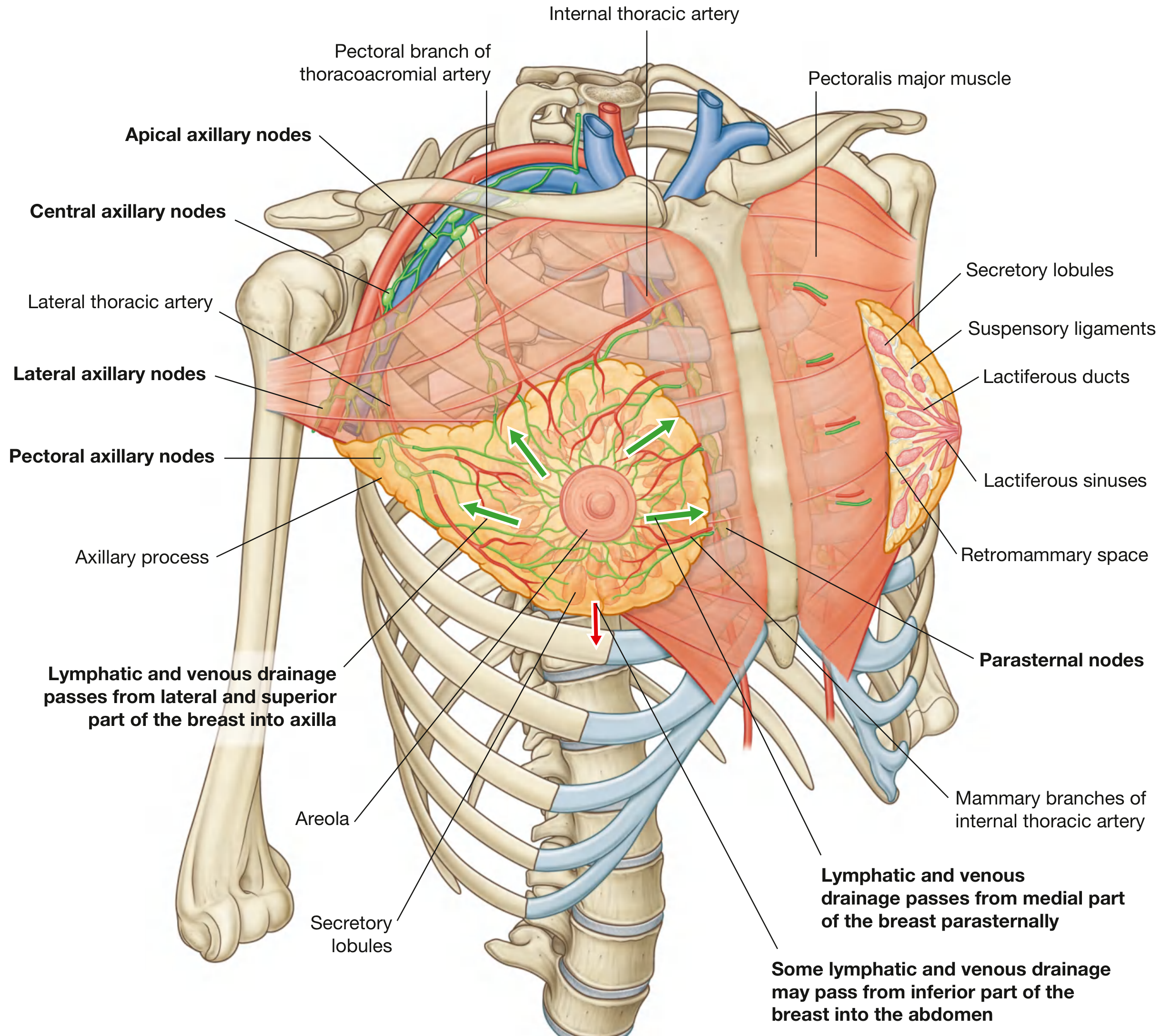
Lymphatic drainage pathways of the breast - note the dominant lateral/superior flow into axillary nodes and medial flow into parasternal nodes (Gray's Anatomy for Students)
B. Internal Mammary (Parasternal) Route (~20-25%)
The internal mammary lymph nodes (parasternal nodes) run along the internal thoracic vessels deep to the parietal pleura. They preferentially drain:
- The medial quadrants of the breast
- The deep parenchyma of the breast
- The medial and inferior portions
This route is the primary drainage route in 2-3% of patients and a secondary route in approximately 20% of patients (typically alongside axillary drainage). Tumors in the medial half or deep locations are more likely to drain here.
C. Intercostal Route (Minor)
Some lymphatic vessels follow the lateral branches of the posterior intercostal arteries and connect with intercostal nodes near the heads and necks of ribs. These nodes drain either into the thoracic duct or into bronchomediastinal trunks.
D. Minor/Accessory Routes
-
Interpectoral (Rotter's) nodes - located between pectoralis major and minor; not typically a primary drainage site but can be involved
-
Deltopectoral nodes - along the deltopectoral groove
-
Supraclavicular nodes - receive drainage upstream from the axilla (beyond Level III)
-
Contralateral breast - via cross-midline connections from medial lymphatics
-
Abdominal lymphatics - inferior drainage to subdiaphragmatic/inferior phrenic nodes (from the inferior pole of the breast)
-
Gray's Anatomy for Students, p.175
-
Fischer's Mastery of Surgery, p.1396
-
THIEME Atlas of Anatomy, p.230
3. Axillary Lymph Node Levels (Berg's Classification)
The axillary lymph nodes are organized into three anatomic levels defined by their relationship to the pectoralis minor muscle - this is the most important classification in breast cancer surgery.
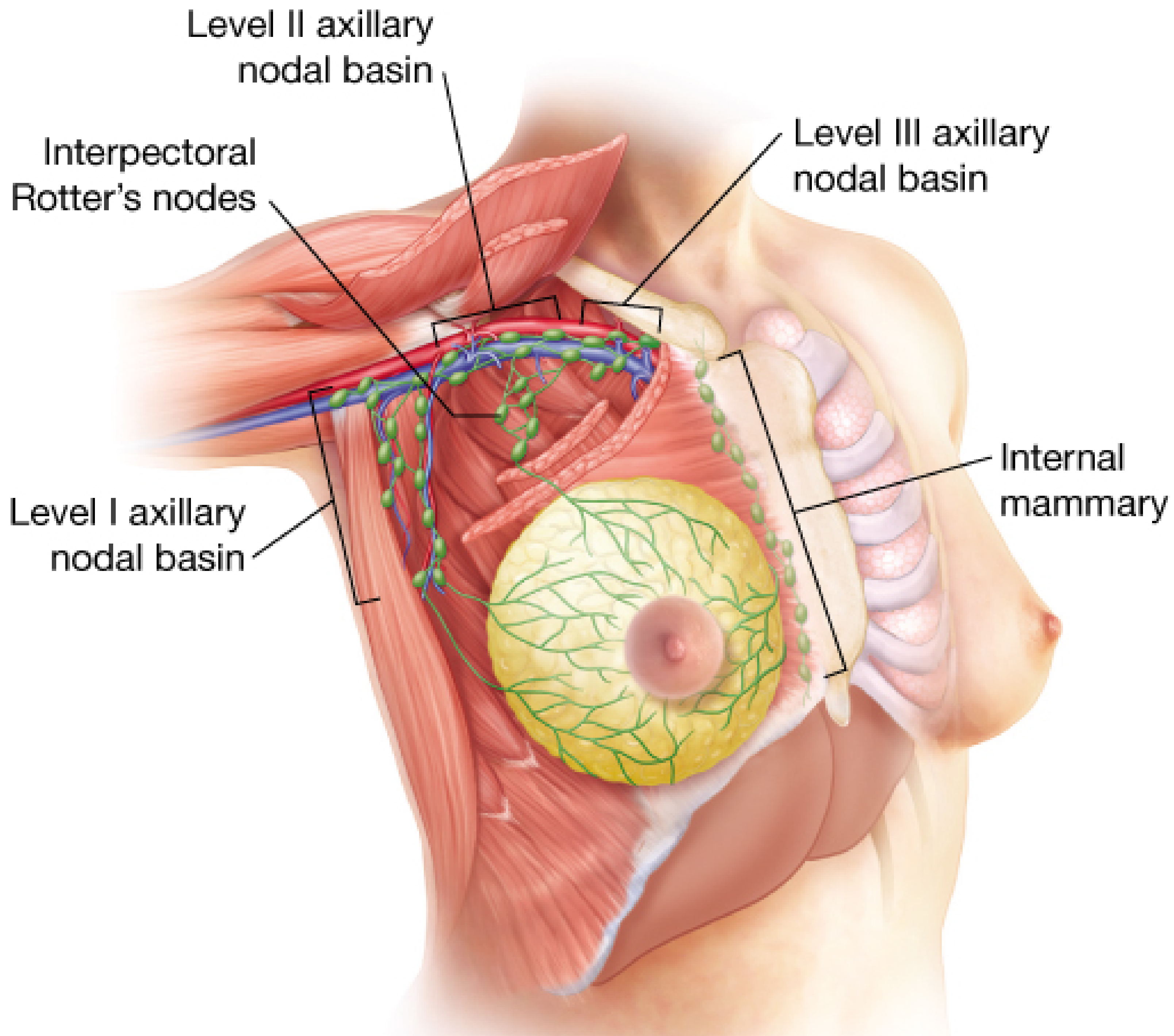
Axillary nodal levels in relation to pectoralis minor - the surgical map for breast cancer staging (Fischer's Mastery of Surgery)
| Level | Location | Node Groups |
|---|---|---|
| Level I (lower axilla) | Lateral to the lateral border of pectoralis minor | Pectoral (anterior) nodes, subscapular nodes, lateral axillary nodes, paramammary nodes |
| Level II (middle axilla) | At the level of / posterior to pectoralis minor | Central axillary nodes, interpectoral (Rotter's) nodes |
| Level III (upper axilla / infraclavicular) | Medial to the medial border of pectoralis minor | Apical axillary nodes, infraclavicular nodes |
Lymph flows sequentially: Level I → Level II → Level III → Supraclavicular nodes → Subclavian trunk → Thoracic duct / Right lymphatic duct
The apex of the axilla is defined by the costoclavicular (Halsted) ligament, where the axillary vein becomes the subclavian vein.
- Sabiston Textbook of Surgery, p.1750-1751
- THIEME Atlas of Anatomy, p.230
4. Quantitative Distribution of Drainage
Radiocolloid mapping studies provide the following approximate distribution of breast lymphatic drainage:
| Nodal Basin | Frequency |
|---|---|
| Axillary nodes | 98% of cases |
| Internal mammary nodes | 35% (as a secondary or co-primary route) |
| Supraclavicular nodes | 3% |
| Infraclavicular nodes | 1.1% |
| Interpectoral (Rotter's) nodes | 0.7% |
(Fischer's Mastery of Surgery, 8th ed.)
5. Relation to Breast Cancer Spread
5.1 Why Lymphatics Are So Important in Breast Cancer
The basement membrane surrounding breast ducts is the critical boundary between non-invasive cancer (DCIS) and invasive breast cancer. Once tumor cells breach the basement membrane, they gain access to the lymphatic channels and blood vessels surrounding the ducts. This is what gives invasive breast cancer its metastatic potential.
"Invasion or infiltration of the wall of the duct gives tumor cells access to the lymphatics and blood vessels that twine around the outside of the ducts, giving it metastatic potential." - Sabiston Textbook of Surgery
Lymphatic spread is the most common initial pathway for carcinoma dissemination, as stated in Robbins' Pathologic Basis of Disease. Tumors do not contain functional lymphatics internally, but vessels at the tumor margins are sufficient to permit lymphatic invasion.
5.2 Quadrant-Specific Spread
Because approximately 50% of breast cancers arise in the upper outer quadrant (the quadrant with the greatest volume of breast tissue), the axillary lymph nodes are the first regional basin to be involved in the majority of cases. This has direct surgical implications.
Medial quadrant tumors, however, have a higher predilection for internal mammary node involvement, which carries different staging and treatment implications.
5.3 Prognostic Significance of Nodal Level Involvement
Axillary nodal status remains the single most powerful prognostic indicator in breast cancer. The pattern of nodal involvement corresponds directly to survival:
| Level of Axillary Involvement | Approximate 5-Year Survival |
|---|---|
| Level I only | ~65% |
| Level II involvement | ~31% |
| Level III involvement | Approaches 0% |
Factors that increase the risk of nodal metastasis include: ER/PR-positive tumors, HER2-amplified tumors, tumor size ≥T2, presence of lymphovascular invasion (LVI), ductal/lobular histology, and multifocality.
- THIEME Atlas of Anatomy, p.230
- Fischer's Mastery of Surgery, 8th ed.
5.4 Histological Appearance: Axillary Node with Metastatic Carcinoma
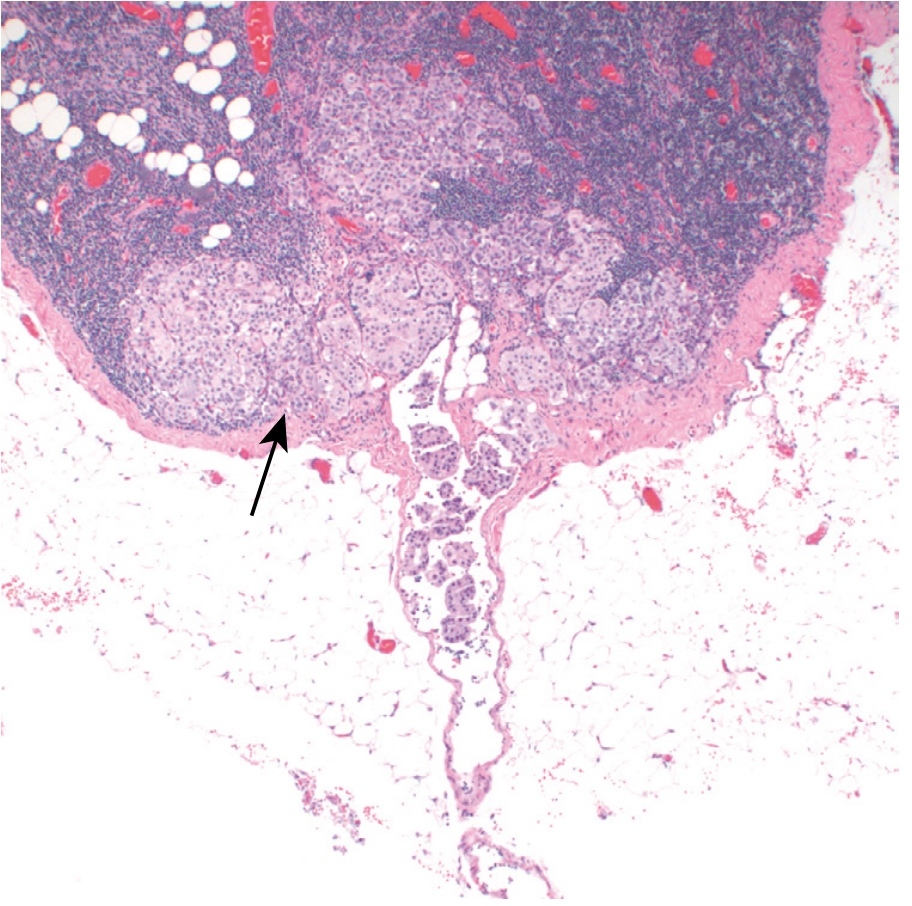
Histology: Axillary lymph node replaced by metastatic breast carcinoma (Robbins). The arrow points to tumor cell aggregates; note the dilated afferent lymphatic channel below.
5.5 Skip Metastasis
Occasionally, tumor cells bypass lower-level nodes (skip metastasis) and appear at Level II or III without Level I involvement. This may occur due to variation in individual lymphatic patterns or because micrometastases were missed at lower levels.
5.6 Parasternal Node Involvement and Contralateral Spread
When tumor cells reach the parasternal (internal mammary) nodes, they can:
- Travel further along the mediastinum
- Cross the midline and spread to the contralateral breast or contralateral axillary nodes
This is one mechanism of bilateral breast cancer or late contralateral recurrence.
5.7 Hematogenous Spread (Beyond the Lymphatics)
Once tumor cells enter the lymphatic system and reach the venous circulation (via the thoracic duct or subclavian vein), hematogenous spread occurs. The three most common distant metastatic sites for breast cancer are:
- Bone (most common - particularly vertebrae, pelvis, femur)
- Lung
- Liver
This organotropism is partly explained by the chemokine receptor-ligand axis: breast cancer cells highly express CXCR4, which is attracted by CXCL12 secreted by bone marrow, liver, lymph nodes, and lung - explaining the preferential colonization of these organs.
- Sabiston Textbook of Surgery, p.2765
- Creasy & Resnik's Maternal-Fetal Medicine
6. Sentinel Lymph Node Biopsy (SLNB) - Clinical Application
The concept of the sentinel lymph node (SLN) is rooted directly in this anatomy. The SLN is defined as the first node in the regional lymphatic basin to receive direct lymph flow from the primary tumor - and therefore the first node likely to harbor metastatic cells.
Technique:
- Injection of radiolabeled colloid (⁹⁹ᵐTc sulfur microcolloid) and/or patent blue vital dye into the subareolar plexus or peritumoral tissue
- The first node to light up on scintigraphic mapping or turn blue = the sentinel node
- The SLN is selectively excised and examined by frozen section and permanent histology
Why it works: 98% of breast lymphatic drainage goes to the axillary nodes, so SLNB reliably samples the first echelon of axillary drainage. If the SLN is negative for tumor, the remaining axillary nodes are almost certainly negative - with 98% accuracy.
This has replaced routine axillary lymph node dissection (ALND) in clinically node-negative patients, significantly reducing surgical morbidity (particularly lymphedema of the ipsilateral arm, which results from disruption of arm lymphatics coursing through the axilla).
- THIEME Atlas of Anatomy, p.230
- Robbins Pathologic Basis of Disease
- Fischer's Mastery of Surgery, 8th ed.
Summary: Drainage Pathway and Cancer Spread at a Glance
Breast parenchyma/nipple/areola
↓
Sappey Subareolar Plexus
↙ ↘
Axillary (75-80%) Parasternal/Internal Mammary (~20-25%)
↓ ↓
Level I nodes Mediastinum → contralateral
↓
Level II nodes
↓
Level III (apical) nodes
↓
Supraclavicular nodes
↓
Subclavian trunk → Thoracic duct → Venous circulation
↓
Distant organs: Bone > Lung > Liver (via hematogenous spread)
Key Clinical Points
- Upper outer quadrant tumors → predominantly axillary spread (most common scenario)
- Medial/inner quadrant tumors → more likely internal mammary node involvement; may be missed on routine axillary dissection
- Nodal level involvement is the strongest single prognostic factor in breast cancer
- SLNB exploits the predictable lymphatic anatomy to stage the axilla with minimal morbidity
- Lymphedema after axillary surgery results from disruption of arm lymphatics that travel alongside or below the axillary vein through the same nodal basin
- Parasternal involvement enables midline crossing and contralateral spread
- Distant metastasis to bone, lung, and liver is driven by both anatomical (venous drainage patterns) and molecular factors (CXCR4/CXCL12 axis)
Sources:
- Gray's Anatomy for Students, p.175
- Fischer's Mastery of Surgery, 8th ed., pp.1396, 1524-1525
- Sabiston Textbook of Surgery, pp.1747-1751, 2762-2765
- Robbins, Cotran & Kumar Pathologic Basis of Disease, pp.259-260
- THIEME Atlas of General Anatomy and Musculoskeletal System, p.230
- Schwartz's Principles of Surgery, 11th ed.
This is a shared conversation. Sign in to Orris to start your own chat.