Adrenergic receptors function
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Searching the Web
adrenergic receptor subtypes function pharmacology 2024 review
I now have comprehensive information from Braunwald's Heart Disease and Goodman & Gilman's to write a thorough answer. Let me compile the complete response.
Adrenergic Receptors: Structure, Subtypes, and Function
Adrenergic receptors (ARs) are G protein-coupled receptors (GPCRs) activated by the catecholamines norepinephrine (NE) and epinephrine (Epi). They are the molecular targets of sympathetic nervous system signaling and form the basis for a vast range of pharmacologic agents.
Overview and Classification
Adrenergic receptors are broadly divided into two families based on pharmacology and signal transduction:
| Family | Subtypes | G Protein | Primary Effector |
|---|---|---|---|
| Alpha-1 (α1) | α1A, α1B, α1D | Gq | Phospholipase C → IP3/DAG → PKC |
| Alpha-2 (α2) | α2A, α2B, α2C | Gi | ↓ Adenylyl cyclase → ↓ cAMP |
| Beta-1 (β1) | - | Gs | ↑ Adenylyl cyclase → ↑ cAMP → PKA |
| Beta-2 (β2) | - | Gs + Gi (dual) | ↑ cAMP (also inhibitory pathway) |
| Beta-3 (β3) | - | Gs | ↑ cAMP → lipolysis, thermogenesis |
Alpha-1 Adrenergic Receptors (α1-AR)
Location: Postsynaptic on vascular smooth muscle, heart, liver, urinary sphincter, skin.
Agonist potency: NE > Epi > Isoproterenol
Signal transduction:
- Coupled to Gq protein → activates phospholipase C (PLC)
- PLC cleaves PIP2 into IP3 (inositol trisphosphate) and DAG (diacylglycerol)
- IP3 triggers intracellular Ca2+ release from the SR
- DAG activates protein kinase C (PKC)
- Also activates mitogen-activated protein kinase (MAPK)
Key functional effects:
- Vasoconstriction - the dominant α1 effect in peripheral arterioles
- Fine-tuning of cardiac contractility and Ca2+ transients in myocytes
- Modulation of cardiac remodeling (both adaptive and maladaptive)
- Contraction of the urinary sphincter, vas deferens, and uterine smooth muscle
- Hepatic glycogenolysis
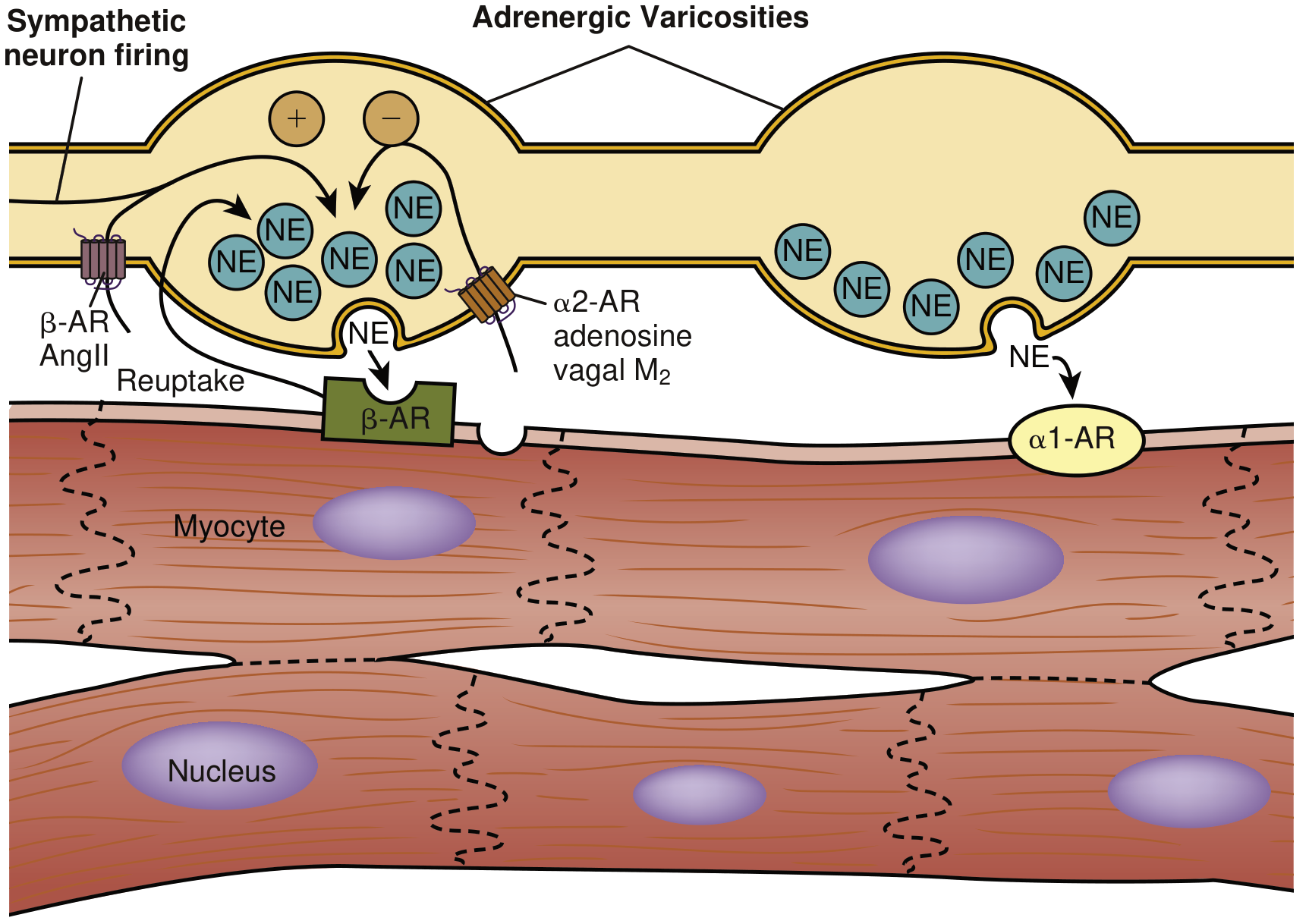
Alpha-2 Adrenergic Receptors (α2-AR)
Location: Primarily presynaptic on adrenergic nerve terminals; also on platelets, vascular smooth muscle, CNS neurons.
Signal transduction:
- Coupled to Gi protein → inhibits adenylyl cyclase → ↓ cAMP
Key functional effects:
- Presynaptic autoreceptor feedback - when NE accumulates in the synapse, it binds α2-AR on the terminal varicosity and inhibits further NE release (negative feedback loop)
- Platelet aggregation
- CNS: decreased sympathetic outflow, sedation (exploited by clonidine)
- Vascular α2 receptors contribute to some vasoconstriction
This is shown clearly in the diagram below:
Beta-1 Adrenergic Receptors (β1-AR)
Location: Predominantly heart (~80% of cardiac β-ARs), kidney (juxtaglomerular cells), adipose tissue.
Signal transduction:
- Coupled exclusively to Gs protein → activates adenylyl cyclase → ↑ cAMP → activates protein kinase A (PKA)
- PKA phosphorylates key cardiac proteins:
- L-type Ca2+ channels (increased Ca2+ influx)
- Ryanodine receptor 2 (RyR2) - increased SR Ca2+ release
- Phospholamban (PLB) - relieves SERCA2a inhibition, speeds Ca2+ uptake → lusitropy
- Troponin I - reduces myofilament Ca2+ sensitivity, aids relaxation
Key functional effects (the "4 chronies"):
- Chronotropy - increased heart rate
- Inotropy - increased contractile force
- Lusitropy - enhanced relaxation
- Dromotropy - accelerated conduction through the AV node
The main positive inotropic response to adrenergic activation in humans is mediated via β1-ARs (Braunwald's Heart Disease, p. 481).
Beta-2 Adrenergic Receptors (β2-AR)
Location: Bronchial smooth muscle, vascular smooth muscle (especially in skeletal muscle), uterus, liver, mast cells. Also ~20% of cardiac β-ARs in the left ventricle.
Signal transduction (dual pathway):
- Coupled to both Gs AND Gi - signal bifurcates at the first postreceptor step
- Gs activation: ↑ cAMP → bronchodilation, vasodilation, uterine relaxation
- Gi activation: ↓ cAMP (partially counters Gs effects; more prominent in failing heart)
Key functional effects:
- Bronchodilation - major therapeutic use (salbutamol/albuterol in asthma, COPD)
- Vasodilation in skeletal muscle vasculature
- Uterine relaxation (tocolysis)
- Some cardiac inotropy (partly indirect - β2 on sympathetic terminals promotes NE release, which then acts on β1-ARs)
- Hepatic glycogenolysis
- Hypokalemia (K+ uptake into skeletal muscle)
Beta-3 Adrenergic Receptors (β3-AR)
Location: Adipose tissue, bladder detrusor muscle, heart (minor).
Key functional effects:
- Lipolysis in adipose tissue
- Thermogenesis in brown adipose tissue
- Bladder relaxation (pharmacologic target: mirabegron for overactive bladder)
- In the heart: β3-AR is coupled to Gi/eNOS pathway and has a mild negative inotropic effect (contrasts with β1/β2)
G Protein Signaling Cascade in Detail
The G protein itself is a heterotrimer (Gα, Gβ, Gγ). On receptor stimulation:
- Agonist binds receptor → conformational change
- Receptor acts as guanine nucleotide exchange factor (GEF) for Gα
- GDP is exchanged for GTP on Gα → Gα-GTP dissociates from Gβγ
- Gαs-GTP activates adenylyl cyclase → converts ATP to cAMP
- cAMP activates PKA (protein kinase A)
- PKA phosphorylates downstream effectors (see above)
- Intrinsic GTPase activity of Gα hydrolyzes GTP → GDP → G protein reassembles (signal terminates)
The inhibitory Gi pathway (α2-AR, some β2 in failing heart): Gαi inhibits adenylyl cyclase; the freed Gβγ activates inward-rectifying K+ channels (GIRK), slowing SA node firing. Adenosine receptors also use this pathway.
Receptor Desensitization
A potent feedback mechanism prevents overstimulation (Braunwald's Heart Disease, p. 601):
- Sustained β-agonist stimulation recruits GRK2 (G protein-coupled receptor kinase 2; formerly BARK1)
- GRK2 phosphorylates the carboxyl-terminal of the β-AR
- This increases receptor affinity for β-arrestin
- β-Arrestin uncouples the receptor from Gs → ↓ adenylyl cyclase activation
- β-Arrestin can also shift coupling from Gs to Gq and trigger receptor internalization
- Resensitization occurs when phosphatases dephosphorylate the receptor, restoring surface expression
In heart failure, this GRK2-arrestin pathway is chronically activated, resulting in profound β-AR downregulation and uncoupling - a key contributor to reduced contractile reserve.
Comparative Cardiovascular Effects
| Effect | α1-mediated | β-mediated |
|---|---|---|
| Heart rate | ± | ++ (↑) |
| Contractility (inotropy) | ± | ++ (↑) |
| Relaxation (lusitropy) | - | ++ (↑) |
| AV conduction | ± | ++ (↑) |
| Coronary arterioles | ++ vasoconstriction | Vasodilation |
| Peripheral arteries | ++ vasoconstriction | Vasodilation |
| Second messenger | GPCR → PKC + MAPK | GPCR → cAMP → PKA |
Source: Braunwald's Heart Disease, Table 46.2
Pharmacologic Relevance
| Drug Class | Receptor Target | Clinical Use |
|---|---|---|
| Phenylephrine | α1 agonist | Vasopressor, nasal decongestant |
| Clonidine | α2 agonist | Hypertension, ADHD, opioid withdrawal |
| Prazosin | α1 antagonist | Hypertension, BPH, PTSD |
| Salbutamol/Albuterol | β2 agonist | Asthma, COPD |
| Dobutamine | β1 agonist | Acute heart failure, stress echo |
| Propranolol | β1 + β2 antagonist | HTN, arrhythmia, tremor, migraine |
| Metoprolol | β1 selective antagonist | HTN, heart failure, post-MI |
| Mirabegron | β3 agonist | Overactive bladder |
| Carvedilol | α1 + β1 + β2 antagonist | Heart failure, HTN |
Key Summary Points
- All adrenergic receptors are 7-transmembrane GPCRs
- α1: Gq → IP3/DAG/PKC → vasoconstriction and smooth muscle contraction
- α2: Gi → ↓cAMP → presynaptic feedback inhibition of NE release
- β1: Gs → ↑cAMP/PKA → cardiac stimulation (chronotropy, inotropy, lusitropy, dromotropy)
- β2: Gs + Gi (dual) → bronchodilation, vasodilation; Gi pathway becomes more prominent in pathologic states
- β3: Gs → lipolysis, thermogenesis; Gi in heart → mild negative inotropy
- Desensitization via GRK2/β-arrestin is critical in limiting responses and is dysregulated in heart failure
Sources: Braunwald's Heart Disease (2-Vol Set), Ch. 46 | Goodman & Gilman's The Pharmacological Basis of Therapeutics, Ch. 3-4 | 2024 review on β-AR regulation in Cells
This is a shared conversation. Sign in to Orris to start your own chat.