Teach me on neonatal jaundice
Reading File
Finding Sources
Finding Sources
Searching PubMed
"neonatal jaundice" OR "neonatal hyperbilirubinemia"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Searching the Web
AAP 2022 neonatal jaundice hyperbilirubinemia guidelines updated phototherapy thresholds
I now have all the material I need for a comprehensive, well-illustrated teaching session. Let me compile the full response.
Neonatal Jaundice - Complete Teaching Guide
1. Overview and Epidemiology
Neonatal jaundice (neonatal hyperbilirubinemia) is the yellow discoloration of skin and sclera in newborns caused by elevated bilirubin. It is extremely common:
- Nearly every newborn develops an unconjugated serum bilirubin >1 mg/dL (the adult upper limit) in the first week of life
- Clinical jaundice (visible discoloration) appears when total bilirubin rises above ~5 mg/dL
- Physiologic jaundice affects approximately 50% of all normal newborns
- Unconjugated hyperbilirubinemia is the dominant form in neonates; conjugated hyperbilirubinemia is less common and always pathologic
2. Bilirubin Metabolism - The Biochemical Foundation
Understanding why newborns are so prone to jaundice requires knowing the normal bilirubin pathway:
| Step | Normal Process | Neonatal Problem |
|---|---|---|
| Production | Heme (from hemoglobin) → unconjugated bilirubin | Neonates have a large RBC mass with rapid turnover, generating more bilirubin |
| Transport | Unconjugated bilirubin binds albumin, travels to liver | Reduced albumin binding capacity in preterm infants |
| Hepatic uptake | Bilirubin taken up by hepatocytes via Y and Z proteins | Immature transporter expression |
| Conjugation | Glucuronyl transferase converts to conjugated (water-soluble) bilirubin | Enzyme activity is reduced at birth; doesn't fully mature until ~2 weeks |
| Excretion | Conjugated bilirubin excreted into bile | Reduced |
| Enterohepatic | Gut bacteria deconjugate some bilirubin → reabsorbed | Neonates lack gut flora → increased enterohepatic recirculation |
Three core physiologic factors drive neonatal jaundice:
- Increased bilirubin production (fetal hemoglobin breakdown, polycythemia)
- Decreased hepatic clearance/conjugation (immature glucuronyl transferase)
- Increased enterohepatic resorption (minimal gut flora, slow gut motility)
"The unconjugated hyperbilirubinemia of neonatal 'physiologic jaundice' results from accelerated hemolysis and an immature hepatic system for the uptake, conjugation, and secretion of bilirubin." - Harper's Illustrated Biochemistry, 32nd Ed.
3. Classification of Neonatal Jaundice
A. Unconjugated (Indirect) Hyperbilirubinemia
Benign/Physiologic:
| Cause | Key Features |
|---|---|
| Physiologic jaundice | Appears days 2-3; peaks day 4-5; rarely rises >5 mg/dL/day; usually resolves by 2 weeks; bilirubin rarely >12 mg/dL in term infants |
| Breast milk jaundice | Second most common cause; peaks later (days 10-21); may persist 3-10 weeks; likely due to bilirubin-deconjugating enzymes in breast milk or increased enterohepatic circulation |
Pathologic - Hemolytic:
- Hemolytic disease of the fetus/newborn (HDFN): ABO incompatibility (most common), Rh incompatibility, Kell/Duffy/C/E antigens. Jaundice appears within the first few hours of life; bilirubin exceeds safe limits within 48 hours.
- Hereditary RBC disorders: G6PD deficiency, hereditary spherocytosis, hemoglobinopathies
- Polycythemia: excess RBC breakdown
Pathologic - Non-hemolytic:
- Sepsis (bacterial infection impairs hepatic conjugation)
- Hypothyroidism
- Cephalhematoma (resorption of blood)
- Crigler-Najjar syndrome (type I: absent glucuronyl transferase, fatal; type II: reduced activity, treatable)
- Gilbert syndrome (mild, benign, reduced UGT1A1 promoter activity)
Increased enterohepatic circulation:
- Hirschsprung disease
- Pyloric stenosis
- Cystic fibrosis
- Biliary atresia (paradoxically raises unconjugated as well)
B. Conjugated (Direct) Hyperbilirubinemia - Always Pathologic
| Cause | Notes |
|---|---|
| Biliary atresia | Most important - requires urgent surgery (Kasai procedure); conjugated bili >2 mg/dL or >20% of total bili is the diagnostic threshold |
| Neonatal hepatitis (idiopathic) | Most common cause of neonatal cholestasis |
| TORCH infections | CMV, toxoplasmosis, rubella, herpes, syphilis |
| Sepsis | |
| Metabolic: galactosemia, hereditary fructose intolerance, glycogen storage disease, alpha-1-antitrypsin deficiency, Wilson disease | |
| Total parenteral nutrition (TPN) | |
| Dubin-Johnson syndrome / Rotor syndrome | Benign inherited defects in conjugated bilirubin transport |
4. Clinical Features
Physiologic Jaundice Timeline
- First 24 hours: Jaundice in the first 24 hours is almost always pathologic (TSB >5 mg/dL at <24 h = red flag)
- Days 2-5: Typical peak for physiologic jaundice (~6 mg/dL average in term infants)
- Day 10-21: Breast milk jaundice peak
- >2 weeks in term infants (>3 weeks in preterm): Prolonged jaundice - warrants investigation
Clinical Assessment
Jaundice progresses in a cephalocaudal pattern (face → trunk → extremities → palms/soles). However, visual estimation is unreliable and must be confirmed with TSB (total serum bilirubin) or TcB (transcutaneous bilirubin).
Risk Factors for Severe Hyperbilirubinemia
- Prematurity (gestational age <38 weeks)
- Isoimmune hemolytic disease (ABO, Rh incompatibility)
- G6PD deficiency
- Sepsis
- Acidosis, asphyxia
- Cephalhematoma
- East Asian ethnicity
- Previous sibling with jaundice requiring treatment
- Exclusive breastfeeding with poor intake/weight loss
- Albumin <3.0 g/dL
5. The Danger: Bilirubin-Induced Neurologic Dysfunction (BIND)
Unconjugated bilirubin is lipid-soluble and crosses the blood-brain barrier. It deposits preferentially in:
- Basal ganglia (globus pallidus, subthalamic nuclei)
- Cerebellar vermis and dentate nuclei
- Hippocampus
- Cranial nerve nuclei (especially CN III and CN VIII - oculomotor and auditory)
Acute Bilirubin Encephalopathy (ABE) - Early Stage (Potentially Reversible)
- Poor feeding, somnolence/lethargy
- Hypotonia or hypertonia
- High-pitched cry
Progressing ABE - Late Stage
- Marked hypertonia
- Opisthotonos (backward arching of neck and trunk)
- Retrocollis
- Fever
- Irritability, apnea
- Seizures → Death
Kernicterus (Chronic, Irreversible Sequelae)
The classic tetrad:
- Choreoathetoid cerebral palsy
- Sensorineural hearing loss (high-frequency)
- Gaze abnormalities (upward gaze palsy)
- Intellectual disability
Risk increases significantly when TSB exceeds 20-25 mg/dL in term infants. About 70% of affected infants die in the first week; survivors have severe neurologic damage.
More recently, the term kernicterus spectrum disorders (KSDs) has been proposed to capture the full range, including subtle presentations like learning deficits, mild motor/cognitive/behavioral disorders identified later in childhood. - Bradley & Daroff's Neurology
6. Diagnosis and Investigations
Initial Workup
| Test | Rationale |
|---|---|
| Total serum bilirubin (TSB) | Gold standard |
| Direct (conjugated) vs. indirect bilirubin fractionation | Direct bili >2 mg/dL or >20% of total = conjugated jaundice = always pathologic |
| Blood type and Coombs test | Screen for isoimmune hemolysis |
| Complete blood count + peripheral smear | Anemia, polycythemia, RBC morphology |
| Reticulocyte count | Elevated in hemolysis |
| G6PD screen | Especially in at-risk ethnicities (African, Mediterranean, Asian) |
| Urinalysis + urine culture | Sepsis workup |
| Thyroid function tests | If prolonged jaundice |
| LFTs, GGT, alkaline phosphatase | If conjugated hyperbilirubinemia suspected |
Predischarge Risk Assessment (AAP 2022 Guideline)
The 2022 AAP guideline uses the hour-specific bilirubin nomogram (Bhutani curve) to predict risk: bilirubin levels are plotted against postnatal age in hours and classified into risk zones (low, low-intermediate, high-intermediate, high). The difference between the measured bilirubin and the phototherapy threshold (the "phototherapy gap") guides follow-up intensity.
7. Treatment
A. Phototherapy
Mechanism: Blue light (~460-490 nm wavelength) converts unconjugated bilirubin to lumirubin (a water-soluble structural isomer) that can be excreted in bile and urine without conjugation.
Indications: Based on age-specific and risk-stratified TSB thresholds (AAP 2022 - slightly higher thresholds than the 2004 guideline, considered safe by the guideline committee):
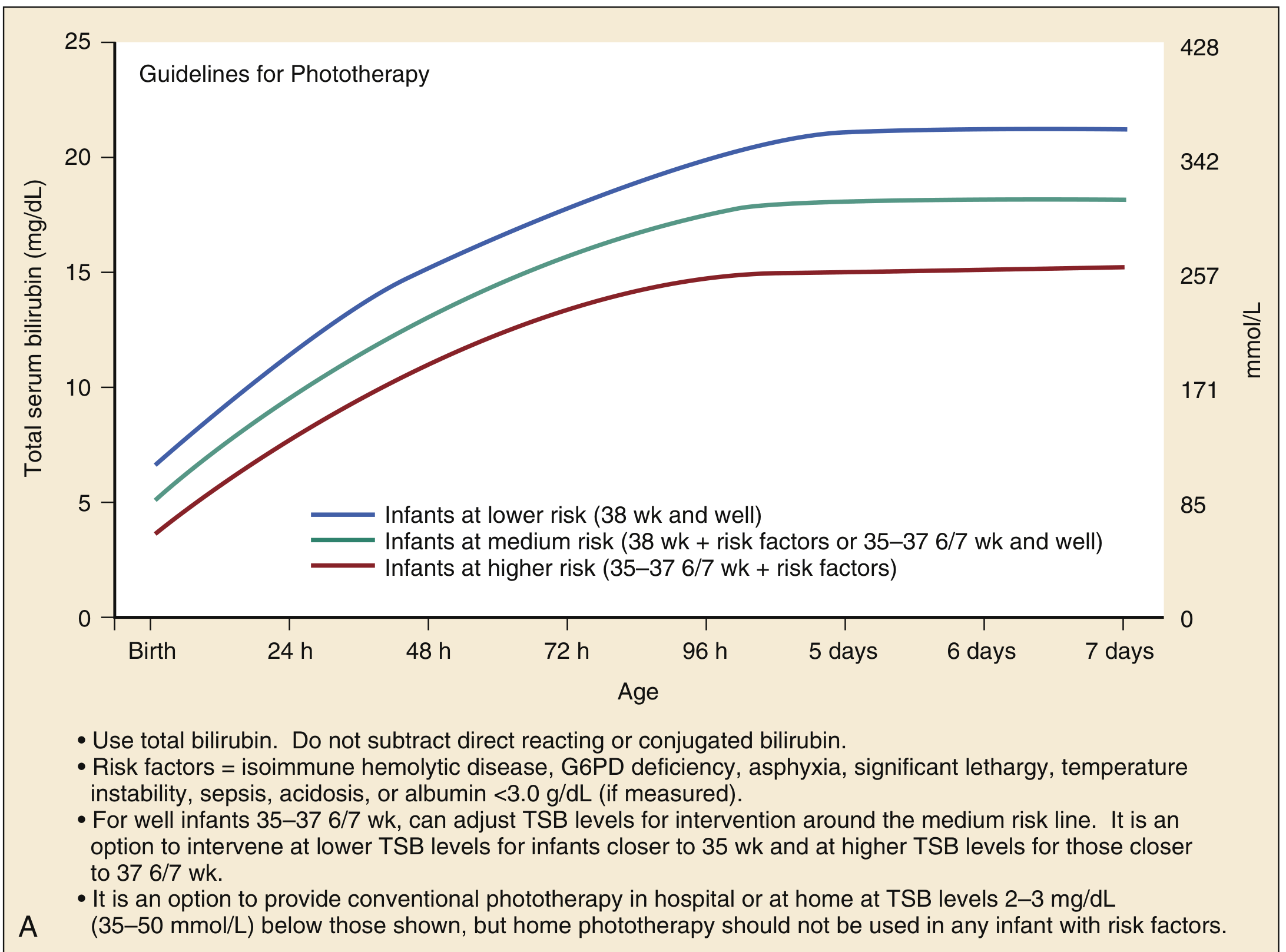
Fig A: AAP phototherapy guidelines for infants ≥35 weeks gestation. Thresholds stratified by risk: lower risk (38 wk, well) = highest threshold; higher risk (35-37 6/7 wk + risk factors) = lowest threshold. Risk factors include isoimmune hemolytic disease, G6PD deficiency, asphyxia, lethargy, temperature instability, sepsis, acidosis, albumin <3.0 g/dL. - Rosen's Emergency Medicine
Practical Phototherapy Points:
- Use total bilirubin - do not subtract direct bilirubin
- Intensive phototherapy: irradiance ≥30 µW/cm²/nm at ~475 nm wavelength (2022 AAP specification, using narrow-spectrum LED blue lights)
- Eye protection is mandatory
- Maximize skin exposure
- Monitor TSB every 4-12 hours depending on clinical status
- Adequate hydration is important (consider IV fluids if oral intake poor)
- Home phototherapy is an option for well-appearing infants without risk factors who have reliable caregivers and can be followed within 24 hours
Key Point from 2022 AAP update: Phenobarbital enhances bilirubin metabolism (induces glucuronyl transferase and UDP-glucuronate synthesis) and is occasionally used in Crigler-Najjar type II. It is not beneficial in Crigler-Najjar type I.
B. Exchange Transfusion
Indications:
- TSB above age-specific exchange transfusion threshold (see graph below) despite intensive phototherapy
- Failure of phototherapy (bilirubin continues to rise)
- Jaundiced infants with any signs of BIND/ABE
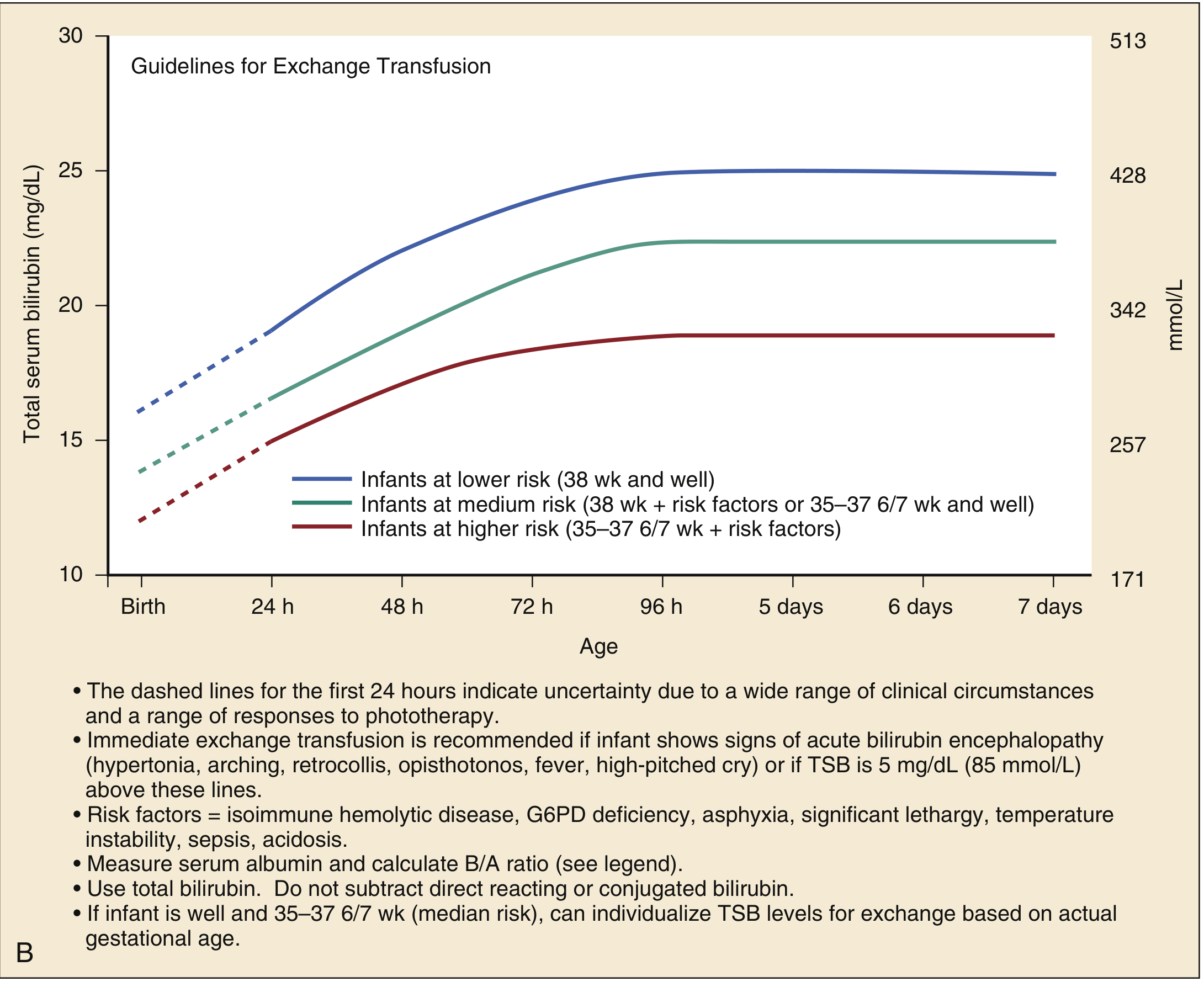
Fig B: AAP exchange transfusion guidelines for infants ≥35 weeks gestation. Dashed lines in first 24 hours reflect clinical uncertainty. Immediate exchange transfusion is recommended for any signs of ABE (hypertonia, arching, retrocollis, opisthotonos, fever, high-pitched cry) or TSB ≥5 mg/dL above threshold lines. - Rosen's Emergency Medicine
Procedure:
- Double-volume exchange transfusion: 180-190 mL/kg packed RBCs
- Replaces approximately 85% of the infant's blood volume
- Reduces total bilirubin by at least 50%
- Performed by serially removing small aliquots (≤5-10 mL/kg) and replacing with packed RBCs until total volume achieved
- Must be done in NICU with continuous hemodynamic monitoring
C. Other Measures
| Intervention | Indication/Notes |
|---|---|
| Adequate hydration/feeding | Reduces enterohepatic resorption; encourage breastfeeding frequency |
| Treat underlying cause | Sepsis → antibiotics; hypothyroidism → levothyroxine |
| IVIG | May reduce need for exchange transfusion in isoimmune hemolytic disease |
| Tin-mesoporphyrin | Inhibits heme oxygenase (blocks bilirubin production) - investigational |
| Zinc sulfate | Recent meta-analyses (2024-2025) suggest some benefit in reducing bilirubin levels in neonatal hyperbilirubinemia, though not yet standard of care |
| Kasai portoenterostomy | For biliary atresia - must be performed before 8-10 weeks of life for best outcome |
8. Disposition
- Admit to hospital: Infants who are ill-appearing, below expected weight for day of life, unable to maintain oral intake, require exchange transfusion, or have any direct (conjugated) hyperbilirubinemia
- Home phototherapy: Suitable for otherwise well infants with reliable caregivers and 24-hour follow-up available
- Outpatient follow-up: All newborns discharged before 72 hours should have bilirubin follow-up within 24-48 hours
9. Summary Table: Physiologic vs. Pathologic Jaundice
| Feature | Physiologic | Pathologic |
|---|---|---|
| Onset | After 24 hours | Within first 24 hours |
| Rate of rise | <5 mg/dL/day | >5 mg/dL/day |
| Peak bilirubin | <12 mg/dL (term) | >12-15 mg/dL |
| Duration | <2 weeks (term) | >2 weeks (term) |
| Bilirubin type | Unconjugated only | May be conjugated |
| Direct bili | Normal (<2 mg/dL) | May be elevated |
| Clinical signs | Well, feeding well | May be ill, signs of BIND |
| Treatment needed | Rarely (observation/phototherapy if near threshold) | Yes |
10. High-Yield Points for Exams and Clinical Practice
- Any jaundice in first 24 hours is pathologic until proven otherwise - check TSB immediately
- Conjugated hyperbilirubinemia is always pathologic - never "physiologic"
- The threshold for neurotoxicity is approximately 20-25 mg/dL in term infants, lower in preterm
- Kernicterus preferentially damages the basal ganglia, auditory nuclei (CN VIII), and oculomotor nuclei
- G6PD deficiency is the most common enzyme defect causing hemolytic jaundice; always screen in at-risk populations
- RhoGAM (anti-D immunoglobulin) within 72 hours of delivery has dramatically reduced Rh hemolytic disease
- Phototherapy uses blue light to create lumirubin (a water-soluble bilirubin isomer) - it does not conjugate bilirubin
- Exchange transfusion (double volume, 180-190 mL/kg) reduces bilirubin by ~50% and replaces ~85% of blood volume
- 2022 AAP guideline raised phototherapy thresholds slightly vs. 2004, uses the bilirubin-phototherapy-threshold gap for risk stratification, and introduced the concept of "escalation of care" for rapidly rising levels
- Home phototherapy is an evidence-based option (confirmed by 2025 systematic review, PMID 40715357) for low-risk, well-appearing infants
Sources: Rosen's Emergency Medicine (9th Ed.) | Robbins & Kumar Basic Pathology | Harper's Illustrated Biochemistry (32nd Ed.) | Quick Compendium of Clinical Pathology (5th Ed.) | Bradley & Daroff's Neurology in Clinical Practice | Tietz Textbook of Laboratory Medicine (7th Ed.) | AAP 2022 Clinical Practice Guideline
This is a shared conversation. Sign in to Orris to start your own chat.