Here is a complete explanation of pulmonary ventilation, drawn from Guyton and Hall Textbook of Medical Physiology.
Pulmonary Ventilation
Pulmonary ventilation is the process of moving air in and out of the lungs - i.e., breathing. It depends on pressure gradients generated by the respiratory muscles acting on the thoracic cage.
1. Mechanics of Breathing
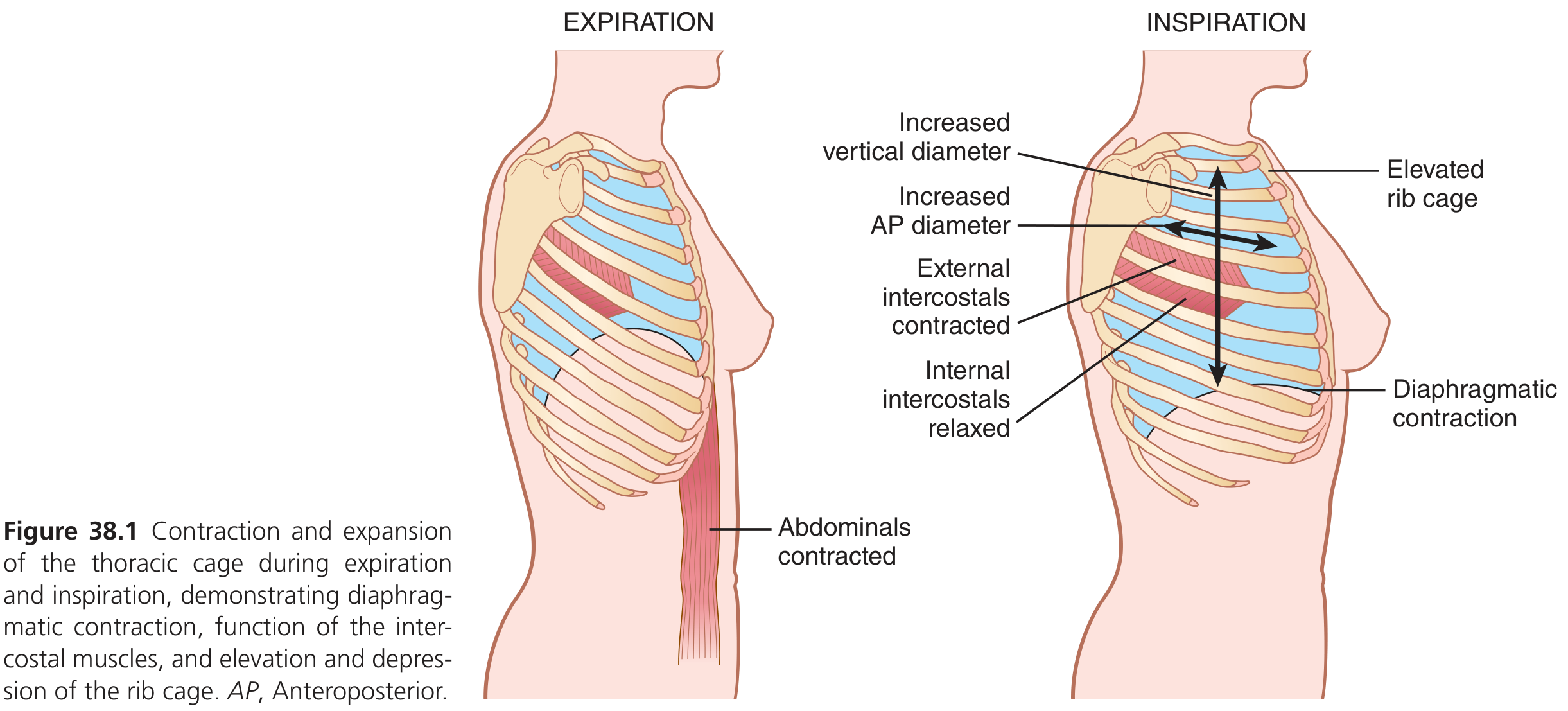
Muscles of Inspiration
The diaphragm is the primary muscle of inspiration. When it contracts, it descends and increases the vertical diameter of the thoracic cavity. Simultaneously, the external intercostals contract and pull the ribs upward and forward, increasing the anteroposterior (AP) diameter by about 20%.
Accessory muscles that assist during forceful inspiration include:
- Sternocleidomastoid - lifts the sternum
- Anterior serrati - lift many ribs
- Scaleni - lift the first two ribs
Muscles of Expiration
Normal (quiet) expiration is largely passive - driven by elastic recoil of the lungs and chest wall when inspiratory muscles relax. Forceful expiration recruits:
- Abdominal recti - pull down on the lower ribs and compress abdominal contents upward against the diaphragm
- Internal intercostals - angle opposite to external intercostals, depressing the rib cage
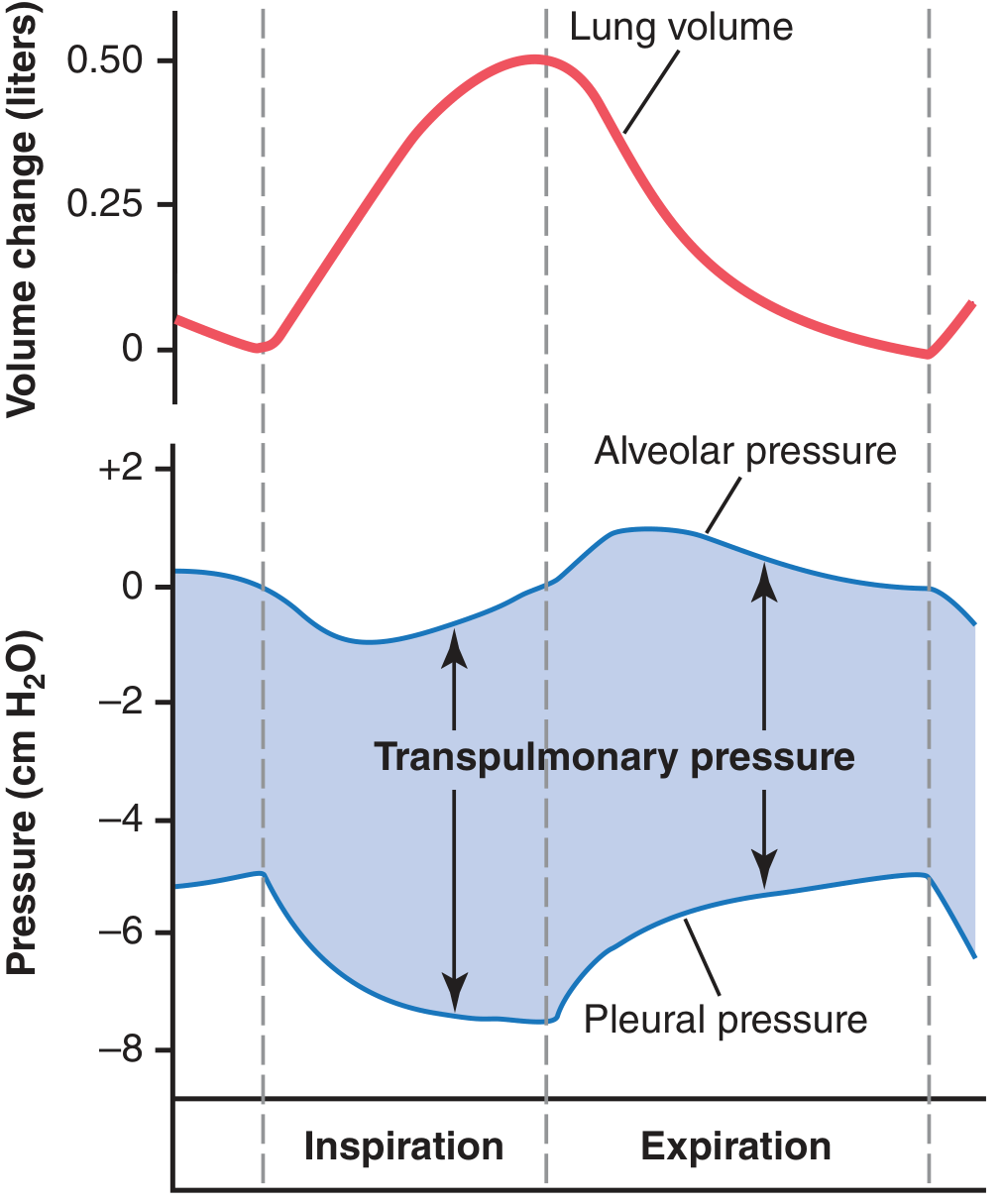
2. Pressures That Drive Air Movement
Three pressures are key:
| Pressure | Definition | Normal Values |
|---|
| Pleural pressure | Pressure in the thin fluid layer between visceral and parietal pleura | -5 cm H₂O at rest; -7.5 cm H₂O at peak inspiration |
| Alveolar pressure | Air pressure inside the alveoli | 0 at rest; -1 cm H₂O during inspiration; +1 cm H₂O during expiration |
| Transpulmonary pressure | Alveolar pressure minus pleural pressure; represents elastic recoil force | ~5 cm H₂O at FRC |
Inspiration: The chest wall expands, pleural pressure falls from -5 to -7.5 cm H₂O, the lung is pulled outward, alveolar pressure drops to -1 cm H₂O below atmosphere, and air flows in.
Expiration: Respiratory muscles relax, the chest recoils, pleural pressure rises back toward -5 cm H₂O, alveolar pressure rises to +1 cm H₂O, and air flows out.
3. Lung Compliance
Compliance is the expandability of the lungs - defined as the volume increase per unit increase in transpulmonary pressure.
Normal compliance = 200 mL/cm H₂O
This means for every 1 cm H₂O increase in transpulmonary pressure, the lungs expand by 200 mL (once equilibrium is reached in 10-20 seconds).
Two elastic forces oppose lung expansion:
- Elastic tissue in the lung parenchyma (collagen and elastin fibers)
- Surface tension of fluid lining the alveoli (~2/3 of total elastic recoil)
Surfactant (secreted by type II alveolar cells) reduces surface tension dramatically, preventing alveolar collapse (atelectasis) and reducing the work of breathing. Without surfactant (as in neonatal respiratory distress syndrome), surface tension is very high and the lungs resist expansion.
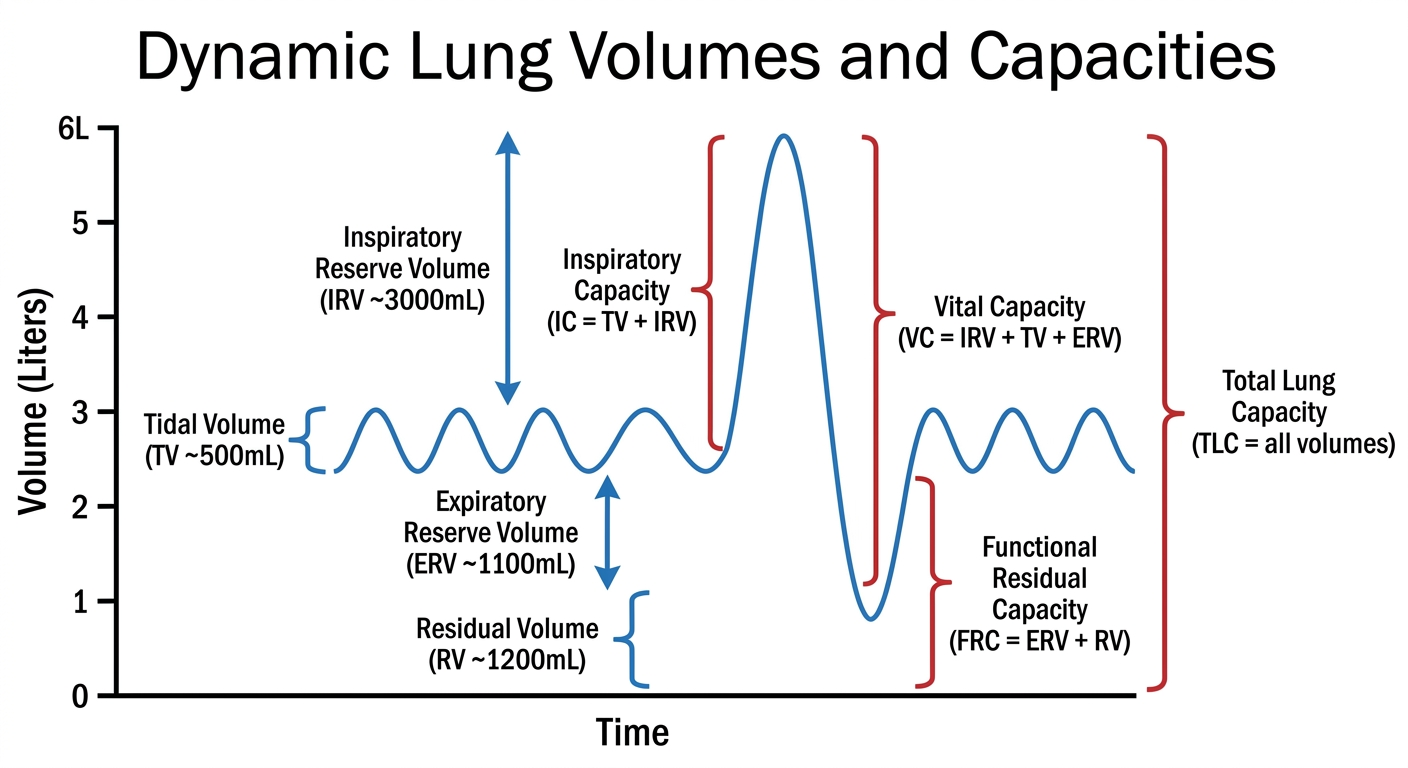
4. Pulmonary Volumes and Capacities
Pulmonary ventilation is quantified using spirometry:
Four primary volumes (non-overlapping):
| Volume | Value (Men) | Value (Women) |
|---|
| Tidal Volume (TV) | 500 mL | 400 mL |
| Inspiratory Reserve Volume (IRV) | 3,000 mL | 1,900 mL |
| Expiratory Reserve Volume (ERV) | 1,100 mL | 700 mL |
| Residual Volume (RV) | 1,200 mL | 1,100 mL |
Four capacities (combinations of volumes):
| Capacity | Formula | Value (Men) |
|---|
| Inspiratory Capacity (IC) | TV + IRV | 3,500 mL |
| Functional Residual Capacity (FRC) | ERV + RV | 2,300 mL |
| Vital Capacity (VC) | IRV + TV + ERV | 4,600 mL |
| Total Lung Capacity (TLC) | All volumes | 5,800 mL |
Women's values are about 20-30% less than men's. Values are larger in athletic and taller individuals.
5. Dead Space and Alveolar Ventilation
Not all inhaled air reaches the alveoli. Some fills conducting airways where no gas exchange occurs.
Types of dead space:
- Anatomical dead space - volume of conducting airways (nose, pharynx, trachea, bronchi) = ~150 mL
- Physiological dead space - anatomical dead space + any non-functional alveoli (in healthy lungs, these are approximately equal; in disease, physiological dead space can reach 1-2 L)
Alveolar Ventilation Rate
The formula is:
V̇A = Respiratory rate × (Tidal Volume - Dead Space)
V̇A = 12 breaths/min × (500 mL - 150 mL) = 4,200 mL/min
This shows why rapid, shallow breathing is inefficient - if rate doubles but TV halves, minute ventilation stays the same but alveolar ventilation falls because dead space is wasted per breath.
6. Functions of the Respiratory Passageways
The trachea is held open by cartilage rings (C-shaped). Bronchi have cartilage plates. Bronchioles (< 1.5 mm diameter) lack cartilage and remain open due to radial traction from surrounding lung tissue. The alveoli themselves have a thin fluid lining, gas exchange surface area of ~70 m², and a blood-gas barrier of only ~0.6 µm thick - optimized for rapid diffusion.
Source: Guyton and Hall Textbook of Medical Physiology, Chapter 38 - Pulmonary Ventilation