Megaloblastic anemia
Reading File
Finding Sources
Finding Sources
Searching PubMed
"megaloblastic anemia"[MeSH Terms] AND ("vitamin B12" OR "folate")
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the information needed for a comprehensive, well-structured answer. Let me compile it.
Megaloblastic Anemia
Definition
Megaloblastic anemia is an anemia (or pancytopenia) resulting from failure of DNA synthesis, which causes an imbalance between nuclear and cytoplasmic maturation in hematopoietic precursors. The impaired DNA synthesis affects all rapidly dividing cells, but the most visible consequence is the production of abnormally large erythroid precursors ("megaloblasts") and large oval red cells in the peripheral blood. - Goldman-Cecil Medicine, p. 1117
Pathophysiology
The common mechanism underlying all forms is defective synthesis of thymidine monophosphate (dTMP), a DNA building block. Here is how it works:
- Folate cycle: Tetrahydrofolate (THF) is the ultimate one-carbon donor required to convert dUMP → dTMP (via thymidylate synthase). Adequate THF depends on vitamin B12.
- B12's role - the "methylfolate trap": Methyl-THF (the main plasma form of folate) can only be converted back to THF via methionine synthase, which requires vitamin B12 (methylcobalamin). When B12 is absent, methyl-THF accumulates and cannot be recycled into usable THF - this is the methylfolate trap. The result is secondary folate deficiency even when folate stores are adequate.
- Second B12 reaction: Adenosylcobalamin is required for L-methylmalonyl-CoA mutase, which converts methylmalonyl-CoA → succinyl-CoA. When blocked, methylmalonic acid (MMA) accumulates - this is the basis of the most specific lab test for B12 deficiency.
- Net effect: Defective dTMP synthesis → uracil incorporation into DNA → chromosomal damage, prolonged cell cycle, maturation arrest, and apoptosis of hematopoietic precursors (ineffective hematopoiesis). - Robbins Pathology & Goldman-Cecil Medicine
Causes
Vitamin B12 (Cobalamin) Deficiency
| Category | Examples |
|---|---|
| Lack of intrinsic factor | Pernicious anemia (autoimmune type A gastritis), gastrectomy, gastric bypass, congenital IF deficiency |
| Food cobalamin malabsorption | Atrophic gastritis (type B), achlorhydria, pancreatic exocrine dysfunction |
| Ileal disease | Surgical resection, Crohn disease, ileal conduit, Imerslund-Gräsbeck syndrome (cubam receptor mutation) |
| Intestinal organisms | Bacterial overgrowth, blind loops, Diphyllobothrium latum (fish tapeworm), Giardia |
| Dietary deficiency | Veganism, strict lacto-vegetarianism, breastfed infant of deficient mother |
| Drug-induced | Metformin, PPIs, H2 blockers, nitrous oxide (oxidizes cobalamin), antiretrovirals |
| Inborn errors | Transcobalamin deficiency, CblC-J mutations |
Note: Daily requirement is 2.4 µg; hepatic stores last several years. Purely dietary B12 deficiency takes years to manifest. - Goldman-Cecil Medicine
Folate Deficiency
| Category | Examples |
|---|---|
| Decreased intake | Alcoholism (most common clinical cause), poor diet, anorexia nervosa, infancy |
| Malabsorption | Celiac disease, tropical sprue, Crohn disease |
| Increased demand | Pregnancy, hemolytic anemia, leukemia, hemodialysis, proliferative skin disease |
| Drug-induced (antifolates) | Methotrexate, pemetrexed, pyrimethamine, trimethoprim, sulfasalazine, anticonvulsants (phenytoin, carbamazepine, valproate) |
Folate stores are modest (months vs. years for B12). Countries with folic acid food fortification have nearly eliminated nutritional folate deficiency except in alcoholics. - Goldman-Cecil Medicine
Other Causes (Not Responsive to B12/Folate)
- Chemotherapy agents: hydroxyurea, azathioprine, cytarabine
- Antiretrovirals: zidovudine, stavudine
- Tyrosine kinase inhibitors: imatinib
- Inborn errors: hereditary orotic aciduria, Lesch-Nyhan syndrome, thiamine-responsive megaloblastic anemia (SLC19A2 mutation)
Morphology
Peripheral Blood Smear
Characteristic findings:
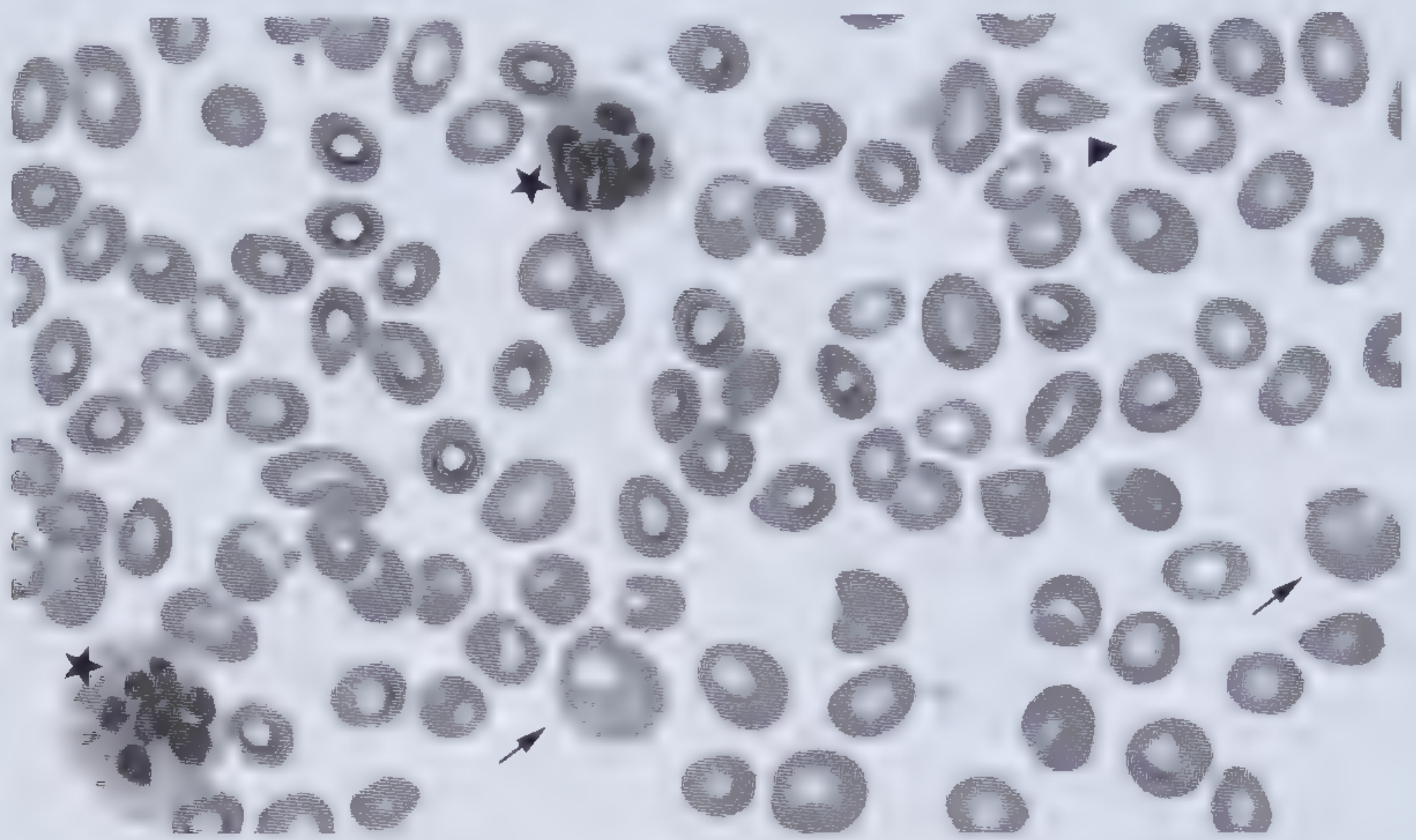
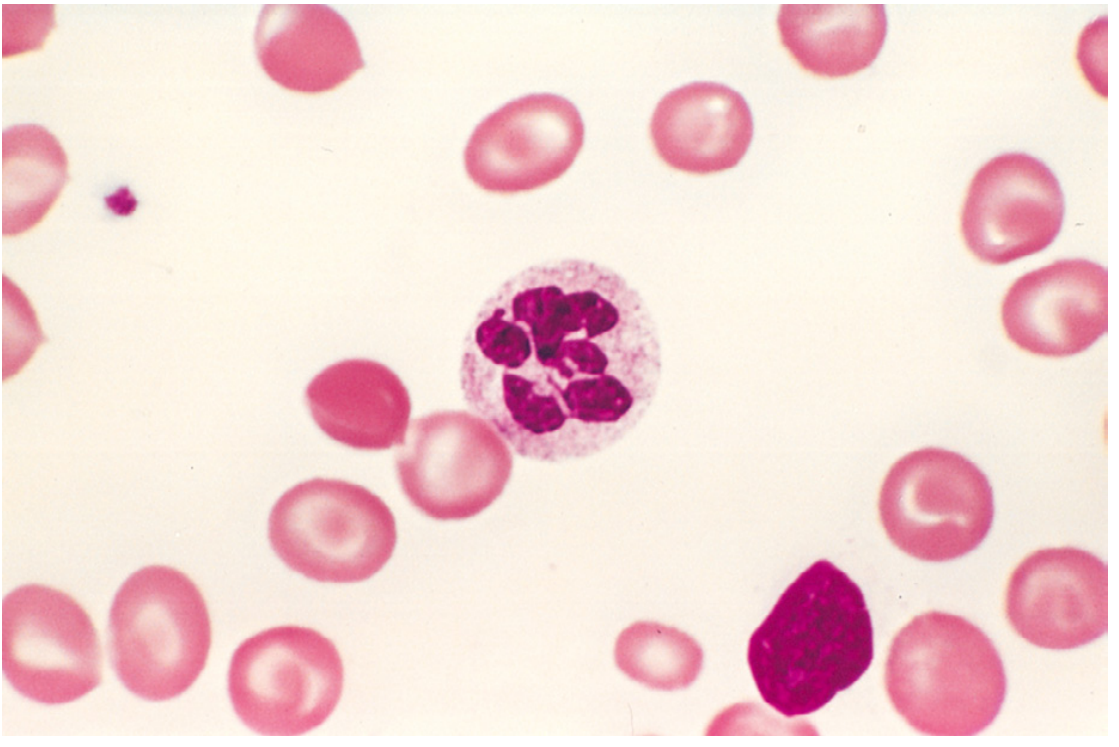
Peripheral blood smear showing macro-ovalocytes (arrows), hypersegmented neutrophils (stars), and teardrop-shaped RBCs (arrowhead) in B12 deficiency. - Frameworks for Internal Medicine
- Macro-ovalocytes - large oval red cells, MCV often >115 fL, appear "hyperchromic" (but MCHC is not elevated)
- Hypersegmented neutrophils - 5+ nuclear lobes (normal: 3-4 lobes); >5% neutrophils with ≥5 lobes, or any neutrophil with ≥6 lobes is pathological
- Anisocytosis and poikilocytosis (teardrop cells)
- Low reticulocyte count (ineffective erythropoiesis)
- Pancytopenia in severe cases
Bone Marrow
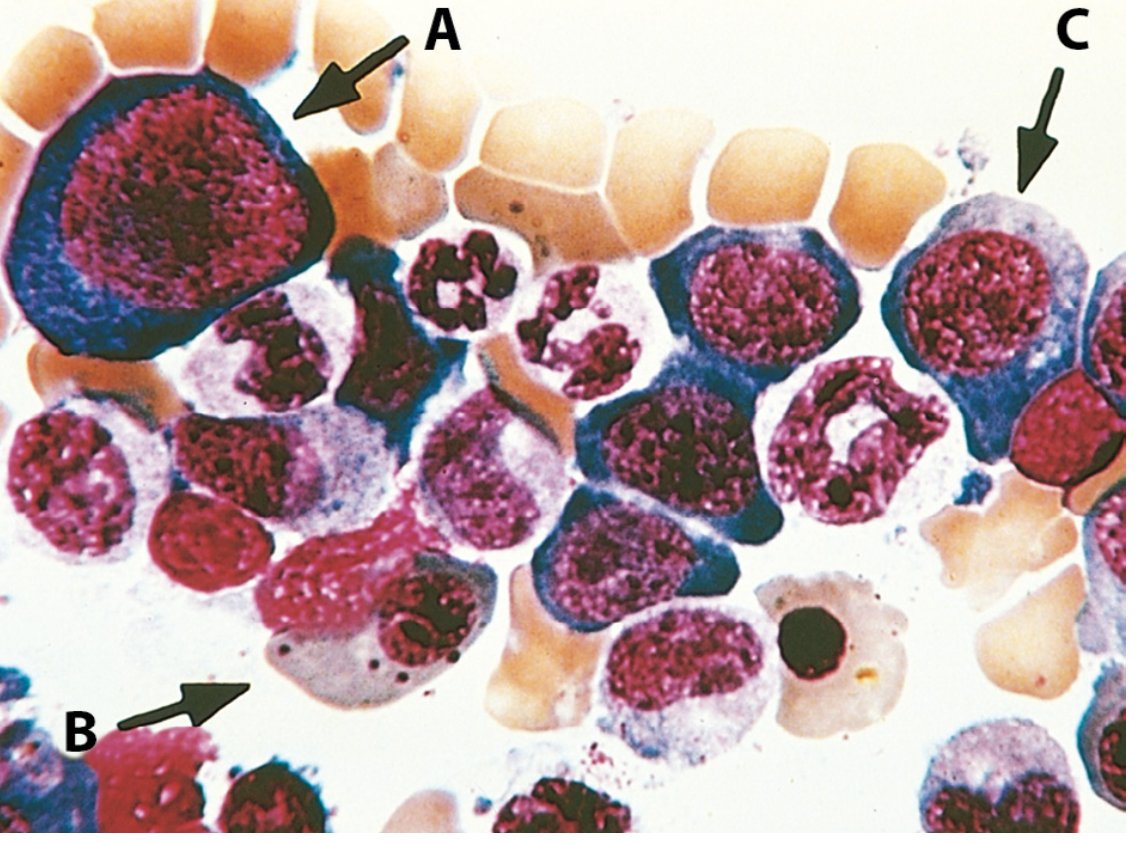
- Hypercellular marrow (response to elevated erythropoietin)
- Megaloblasts - large erythroid precursors with finely distributed ("open") chromatin, cytoplasm matures normally while nucleus lags
- Nuclear-cytoplasmic asynchrony - the hallmark: cytoplasm is hemoglobinized but nucleus remains immature (non-pyknotic)
- Giant metamyelocytes and band forms (granulocytic dysmaturation)
- Hypersegmented megakaryocytes
Despite marrow hypercellularity, most precursors undergo apoptosis → ineffective hematopoiesis → pancytopenia. - Robbins Pathology, p. 608-609
Pernicious Anemia (the Classic B12 Deficiency Syndrome)
Definition: Autoimmune destruction of gastric parietal cells (type A gastritis) → loss of intrinsic factor (IF) secretion → B12 malabsorption.
Autoantibodies:
- Anti-intrinsic factor (blocking) antibodies - 50-70% sensitive, highly specific
- Anti-parietal cell antibodies - 90% sensitive, less specific (also positive in other autoimmune gastritis)
Extra-hematologic features:
- Subacute combined degeneration of the cord - demyelination of dorsal and lateral columns
- Symptoms: peripheral neuropathy, loss of vibration and position sense, ataxia, upper motor neuron signs, psychiatric disturbances ("megaloblastic madness")
- Key point: neurological complications can occur with minimal or no anemia, and folate supplementation does NOT improve (and may worsen) the neuropathy
- Glossitis - smooth, beefy-red tongue
- Jaundice - mild, from intramedullary hemolysis (elevated LDH, indirect bilirubin)
- Increased risk of gastric carcinoma and gastric carcinoids - gastric mucosa atrophy and metaplasia persist even with B12 treatment
Laboratory Diagnosis
| Test | Findings |
|---|---|
| CBC | Macrocytic anemia (MCV often >115 fL), leukopenia, thrombocytopenia |
| Peripheral smear | Macro-ovalocytes, hypersegmented neutrophils |
| Reticulocyte count | Low (inappropriate) |
| Serum B12 | Low (<200 pg/mL), but sensitivity only ~60% |
| Serum folate | Low in folate deficiency |
| Serum methylmalonic acid (MMA) | Elevated in B12 deficiency; sensitivity ~98% - the most specific marker |
| Serum homocysteine | Elevated in both B12 AND folate deficiency (95% of folate-deficient patients); not discriminatory |
| Anti-IF antibodies | Positive in pernicious anemia (50-70%) |
| Anti-parietal cell antibodies | Positive in 90% of pernicious anemia |
| Serum gastrin | Elevated in pernicious anemia |
| Pepsinogen-1 | Low in pernicious anemia |
| Serum LDH | Markedly elevated (intramedullary destruction) |
| Serum bilirubin (indirect) | Mildly elevated |
Key diagnostic point: MMA is elevated only in B12 deficiency (not folate), making it the test to distinguish between the two. Homocysteine rises in both. Both markers should be measured before starting treatment as they normalize rapidly. - Goldman-Cecil Medicine
Note: The Schilling test (radiolabeled B12 absorption) is no longer available.
B12 Deficiency vs. Folate Deficiency: Key Differences
| Feature | B12 Deficiency | Folate Deficiency |
|---|---|---|
| Neurological complications | Yes (subacute combined degeneration) | No |
| MMA elevated | Yes | No |
| Homocysteine elevated | Yes | Yes |
| Serum B12 | Low | Normal |
| Common causes | Pernicious anemia, veganism, malabsorption | Alcoholism, poor diet, pregnancy, antifolates |
| Body stores | Years | Weeks to months |
| Folate treatment safe? | Corrects anemia but WORSENS neuropathy | Yes |
Treatment
Vitamin B12 Deficiency
- Parenteral B12 (cyanocobalamin or hydroxocobalamin): IM injections, typically 1000 µg daily × 7 days, then weekly × 4, then monthly for life (in pernicious anemia)
- High-dose oral B12: 1000-2000 µg/day - effective even in pernicious anemia because passive diffusion (IF-independent) absorbs ~1% of large oral doses. This is now widely used as an alternative to injections.
- Response: Reticulocyte crisis begins within 3-5 days; hematocrit improves over weeks; neurological improvement occurs if treated early (may be irreversible if delayed)
- Gastric mucosal changes in pernicious anemia are NOT reversed by treatment
Folate Deficiency
- Folic acid: 1-5 mg/day orally
- Must never give folate alone when B12 deficiency is suspected or untreated - this corrects the anemia and masks the diagnosis while neurological damage continues
- Supplementation in pregnancy (400 µg/day) prevents neural tube defects
Acute Megaloblastic Anemia
- Can be precipitated by nitrous oxide anesthesia in subclinically B12-deficient patients
- Treat underlying cause; consider cofactor replacement
Key Clinical Pearls
- Severity of anemia is inversely related to severity of neuropathy in B12 deficiency - patients with severe neurological disease may have mild or no anemia.
- Folate supplementation cannot substitute for B12 in pernicious anemia - the neurological lesion (related to methylmalonyl-CoA pathway) is folate-independent.
- Pancytopenia - megaloblastic anemia can affect all cell lines; do not assume isolated marrow disease.
- Alcoholism - macrocytosis in alcoholics may be masked by coexisting iron deficiency; think of combined deficiencies.
- Drugs - metformin, PPIs, and anticonvulsants are common iatrogenic causes to remember.
- Pernicious anemia patients need at least one screening endoscopy for gastric adenocarcinoma and carcinoid tumors.
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease (9th/10th ed.); Goldman-Cecil Medicine, International Ed.; Frameworks for Internal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.