Portal hypertension
Reading File
Finding Sources
Searching PubMed
"portal hypertension"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Searching Images
portal hypertension pathophysiology diagram varices ascites
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the complete answer.
Portal Hypertension
Definition
Portal hypertension is defined as a pathological increase in portal venous pressure, specifically a hepatic venous pressure gradient (HVPG) ≥6 mmHg (normal 1–5 mmHg). Clinically significant portal hypertension is defined as HVPG ≥10 mmHg (threshold for varices and decompensation), and variceal hemorrhage risk rises sharply once HVPG exceeds 12 mmHg. — Yamada's Textbook of Gastroenterology, Current Surgical Therapy 14e
Anatomy of the Portal System
The portal vein forms behind the neck of the pancreas from the junction of the superior mesenteric vein (SMV) and splenic vein. The left gastric (coronary) vein drains into the confluence, and the inferior mesenteric vein joins the splenic vein. The portal vein supplies ~75% of hepatic blood flow and ~50% of hepatic oxygen delivery. The liver receives 25–30% of total cardiac output. — Yamada's Textbook of Gastroenterology
Classification of Causes
| Level | Causes |
|---|---|
| Presinusoidal | Schistosomiasis, extrahepatic portal vein thrombosis, splenic vein thrombosis, splanchnic arteriovenous fistula, idiopathic portal hypertension |
| Sinusoidal | Cirrhosis (all causes — most common), alcoholic hepatitis, nodular regenerative hyperplasia, sarcoidosis, hereditary hemorrhagic telangiectasia |
| Postsinusoidal | Budd-Chiari syndrome, IVC malformation/web, constrictive pericarditis, right heart failure |
In North America, cirrhosis is the leading cause, accounting for ~90% of cases. Worldwide, schistosomiasis, portal vein thrombosis, and Budd-Chiari are more frequent. — Current Surgical Therapy 14e, Yamada's
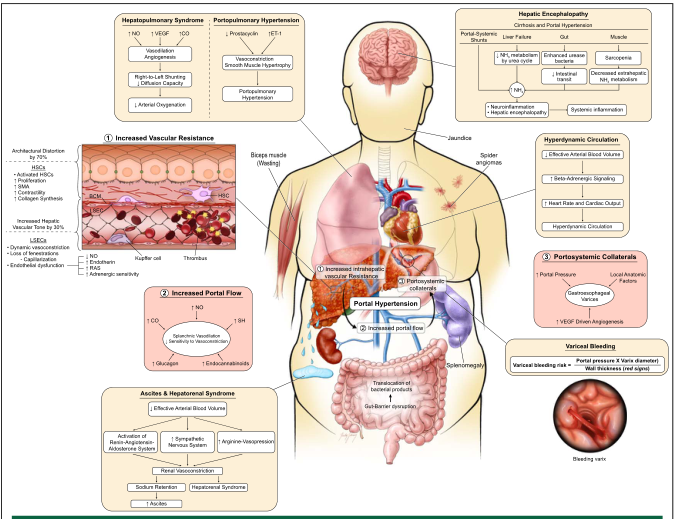
Pathophysiology
Two Core Mechanisms
1. Increased intrahepatic resistance (the primary driver):
- Cirrhosis causes progressive collagen deposition, nodule formation, and architectural distortion of sinusoidal flow
- Both structural (passive): fibrosis, nodule compression
- And dynamic (reversible, ~30% of resistance): hepatic stellate cell (HSC) contraction, endothelial dysfunction
- In the cirrhotic liver, endothelial NO synthase (eNOS)-derived NO is paradoxically reduced → intrahepatic vasoconstriction. ET-1 binding to ET-A receptors on HSCs promotes further vasoconstriction
2. Increased portal venous inflow:
- Splanchnic arteriolar vasodilation (mediated by excess NO, glucagon, endocannabinoids in the splanchnic circulation) increases flow into the portal system — a hemodynamic paradox: NO is deficient intrahepatically but overproduced systemically
Downstream Consequences
The resulting hemodynamic syndrome includes:
- Hyperdynamic circulation: ↑ cardiac output, ↑ total blood volume, ↓ systemic vascular resistance
- Splanchnic vasodilation → effective arterial hypovolemia → activation of RAAS, sympathetic nervous system, and ADH → sodium and water retention → ascites
- Portosystemic collateral formation: blood diverts through low-resistance anastomoses at the esophagus, umbilicus, rectum, and retroperitoneum — forming varices
— Sleisenger & Fordtran's, Medical Physiology, Yamada's
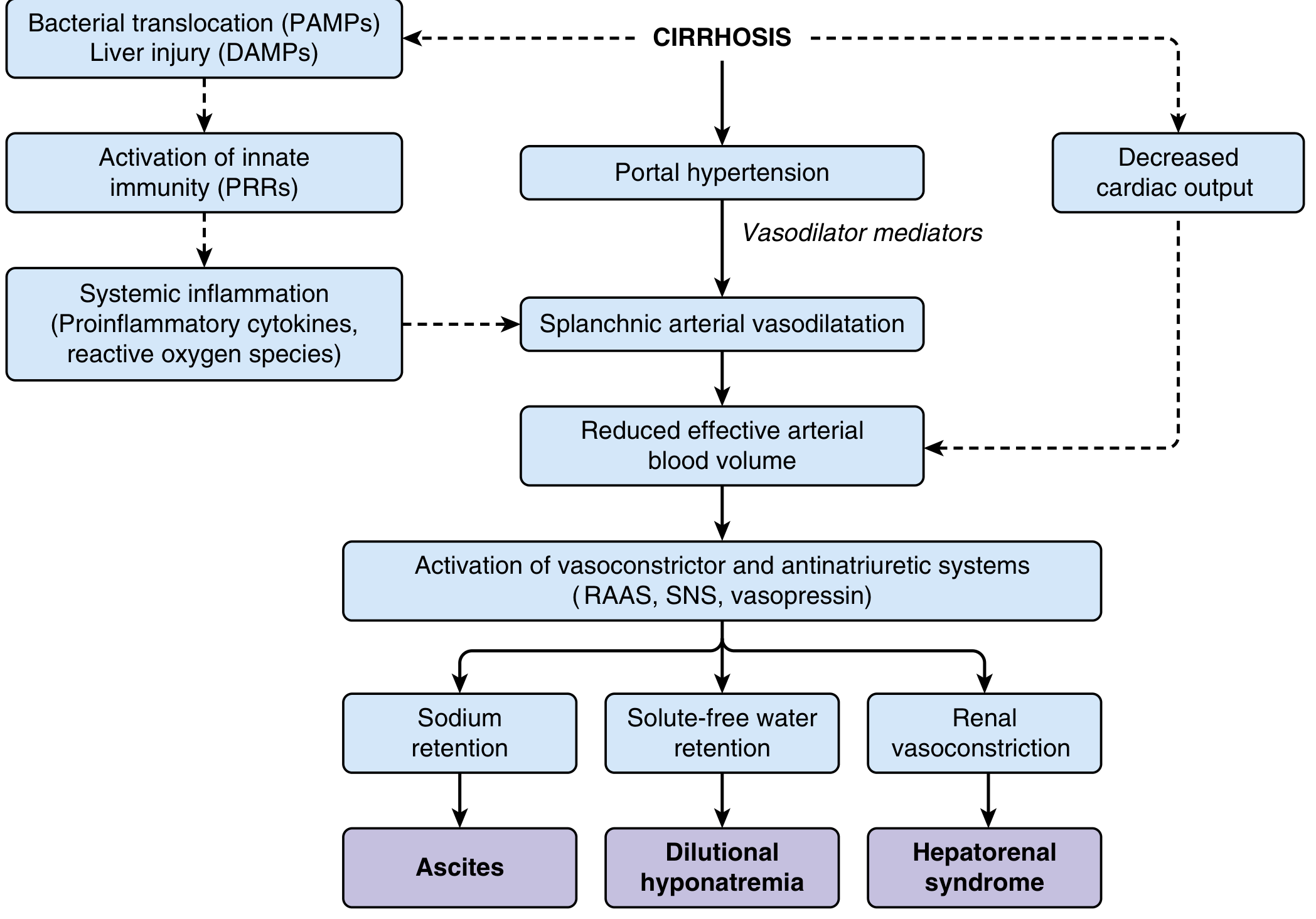
Fig: Systemic circulatory dysfunction in cirrhosis. Splanchnic arterial vasodilation → effective arterial hypovolemia → RAAS/SNS activation → renal sodium retention, ascites, dilutional hyponatremia, and hepatorenal syndrome.
Complications
| System | Complication |
|---|---|
| GI / Vascular | Esophageal varices, gastric varices, ectopic varices, portal hypertensive gastropathy, variceal hemorrhage |
| Renal | Hepatorenal syndrome, renal sodium retention |
| CNS | Hepatic encephalopathy (NH₃ bypasses liver via portosystemic shunts) |
| Abdominal | Ascites, spontaneous bacterial peritonitis (SBP) |
| Pulmonary | Hepatopulmonary syndrome, portopulmonary hypertension, hepatic hydrothorax |
| Hematologic | Hypersplenism (cytopenia), impaired coagulation, hypercoagulability |
| Metabolic | Hyponatremia, adrenal insufficiency, malnutrition |
50% of cirrhotic patients have esophageal varices; ~1/3 will bleed within the first year. Mortality from variceal bleeding ranges from 5% (Child-Pugh A) to 68% (Child-Pugh C). — Current Surgical Therapy 14e
HVPG Thresholds (Clinical Significance)
| HVPG | Significance |
|---|---|
| <5 mmHg | Normal |
| 6–9 mmHg | Portal hypertension (subclinical) |
| ≥10 mmHg | Clinically significant; varices/decompensation risk ↑ |
| ≥12 mmHg | Threshold for variceal formation and hemorrhage |
| ≥20 mmHg | High risk of treatment failure, early rebleeding, death |
HVPG is measured via transjugular catheterization: HVPG = wedged hepatic venous pressure (WHVP) − free hepatic venous pressure (FHVP). — Yamada's, Washington Manual
Diagnosis
- Ultrasound + Doppler: First-line; evaluates portal vein patency, direction and velocity of flow, splenomegaly, ascites, collaterals
- CT/MRI with contrast: Better characterization of vascular anatomy, portal vein thrombosis, tumor thrombus
- Upper GI endoscopy: Gold standard for detecting esophageal varices (confirms portal hypertension clinically)
- HVPG measurement: Gold standard for quantifying pressure; guides risk stratification and treatment response
- Liver biopsy: Gold standard for diagnosing/staging cirrhosis; often combined with HVPG measurement via transjugular route
- Elastography: Non-invasive liver stiffness assessment (note: overestimated in postprandial state, hepatic inflammation, or right heart failure)
— Yamada's Textbook of Gastroenterology
Management
Goals
- Treat underlying etiology (if reversible)
- Reduce portal pressure (medical, interventional, or surgical)
- Prevent and treat complications
- Liver transplantation (definitive for cirrhotic portal hypertension)
Medical Therapy
| Drug | Mechanism | Use |
|---|---|---|
| Non-selective β-blockers (propranolol, nadolol, carvedilol) | ↓ cardiac output (β1) + splanchnic vasoconstriction (β2) → ↓ portal flow | Primary & secondary prophylaxis of variceal bleeding |
| Diuretics (spironolactone ± furosemide) | Counter RAAS activation | Ascites management |
| Terlipressin / Vasopressin | Splanchnic vasoconstriction | Acute variceal bleeding |
| Octreotide / Somatostatin | ↓ splanchnic blood flow | Acute variceal bleeding |
A target HVPG reduction of ≥20% from baseline or to <12 mmHg with β-blockers predicts reduced bleeding risk.
Endoscopic Therapy
- Endoscopic variceal ligation (EVL): First-line for esophageal varices (primary prophylaxis and acute bleeding)
- Endoscopic sclerotherapy: Injection of sclerosing agents; less favored due to complications (perforation, stricture, infection)
- Screening endoscopy recommended at diagnosis of cirrhosis, repeated every 6–12 months
Transjugular Intrahepatic Portosystemic Shunt (TIPS)
A stent placed between a hepatic vein branch and a portal vein branch (via jugular vein approach), creating a low-resistance intrahepatic shunt. TIPS has largely replaced surgical shunts in current practice.
- Indications: Refractory ascites, recurrent variceal bleeding, hepatorenal syndrome, Budd-Chiari
- Advantages: Reduces portal pressure effectively, minimally invasive
- Complications: Hepatic encephalopathy (most common), shunt dysfunction/stenosis
- A covered (PTFE-coated) stent is preferred for improved patency
Surgical Shunts
Reserved for patients not suitable for TIPS or liver transplantation.
Non-selective shunts (portacaval, mesocaval):
- Decompress the entire portal system
- Effective at controlling bleeding (>90%) but high rate of encephalopathy and worsened liver failure
- Side-to-side portacaval: also relieves ascites by decompressing sinusoidal pressure
Selective shunts — Distal Splenorenal Shunt (Warren shunt):
- Anastomosis of the distal splenic vein to the left renal vein (end-to-side)
- Decompresses gastroesophageal varices via vasa brevia while preserving mesenteric portal flow to the liver
- Controls bleeding in >90% of patients with lower encephalopathy rates
- Does NOT relieve ascites (portal flow maintained); contraindicated in massive ascites
- Preferred over non-selective shunts; does not require porta hepatis dissection → suitable as a bridge to transplant
Rex shunt (meso-left portal bypass):
- Jugular vein graft from SMV to intrahepatic left portal vein
- Primarily used in children with extrahepatic portal vein thrombosis
- Restores physiological portal flow; success rate 91–93%
Devascularization procedures (e.g., Sugiura): Ligate gastroesophageal venous drainage; largely historical.
Liver Transplantation
Gold standard for cirrhotic portal hypertension — cures both the underlying disease and all complications. — Current Surgical Therapy 14e
Portosystemic Collateral Sites
When portal pressure rises, blood diverts through pre-existing venous anastomoses:
| Location | Clinical Manifestation |
|---|---|
| Lower esophagus | Esophageal varices (most dangerous) |
| Stomach | Gastric varices |
| Umbilicus (falciform ligament) | Caput medusae |
| Rectum | Rectal varices (distinguish from hemorrhoids) |
| Retroperitoneum | Retroperitoneal collaterals |
— Medical Physiology, Sleisenger & Fordtran's
Special Scenarios
Sinistral (left-sided) portal hypertension: Caused by isolated splenic vein thrombosis (e.g., from pancreatitis). Portal vein pressure is normal; isolated gastric varices form via short gastric vein collaterals. Treated by splenectomy.
Portopulmonary hypertension: Pulmonary arterial hypertension complicating portal hypertension; mediated by ↑ ET-1 and ↑ prostacyclin imbalance → pulmonary vasoconstriction and smooth muscle hypertrophy.
Hepatopulmonary syndrome: Intrapulmonary vascular dilatation due to ↑ NO and ↑ VEGF → right-to-left shunting → hypoxemia. Characterized by the orthodeoxia-platypnea triad (↓ PaO₂ upright, improved supine).
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Yamada's Textbook of Gastroenterology, 7th ed.; Current Surgical Therapy, 14th ed.; Medical Physiology (Boron & Boulpaep); Washington Manual of Medical Therapeutics.
This is a shared conversation. Sign in to Orris to start your own chat.