Occupational dermatitis for MD Dermatology
Reading File
Finding Sources
Finding Sources
Searching PubMed
"occupational dermatitis" OR "occupational contact dermatitis"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive material from all the major dermatology textbooks. Let me compile the full MD Dermatology-level answer on Occupational Dermatitis.
Occupational Dermatitis
Definition and Scope
Occupational skin disease (OSD) encompasses any skin condition that is caused or significantly worsened by workplace exposures. OSD is one of the most common categories of occupational illness and accounts for approximately 10% of all occupational disease cases. Among OSDs, occupational contact dermatitis (OCD) is the most prevalent form, constituting ~70-90% of all OSD. The total incidence of OSD has declined over the last decade, likely reflecting better prevention measures and earlier management.
- Fitzpatrick's Dermatology, Vol. 1&2, p. 468
Classification
Occupational dermatitis has two major categories based on pathophysiology:
| Type | Mechanism | Key Features |
|---|---|---|
| Irritant Contact Dermatitis (ICD) | Non-immunologic, direct cytotoxic effect | Most common (~80% of OCD); no prior sensitization needed; concentration/duration dependent |
| Allergic Contact Dermatitis (ACD) | Type IV (delayed) hypersensitivity | Requires prior sensitization; only ~3700 chemicals known to act as true allergens |
Note: The North American Contact Dermatitis Group (NACDG) reported 60% ACD vs. 32% ICD among occupationally referred patients - selection bias toward tertiary referral centres may inflate ACD numbers.
- Fitzpatrick's Dermatology, p. 469-470
Etiology - Causative Agents
Physical Causes
- Heat (burns, hot tar, grease)
- Cold (Raynaud phenomenon, frostbite)
- Moisture / wet work (most common occupational exposure)
- Friction, pressure (calluses, corns)
- UV radiation, ionizing radiation
Chemical Causes
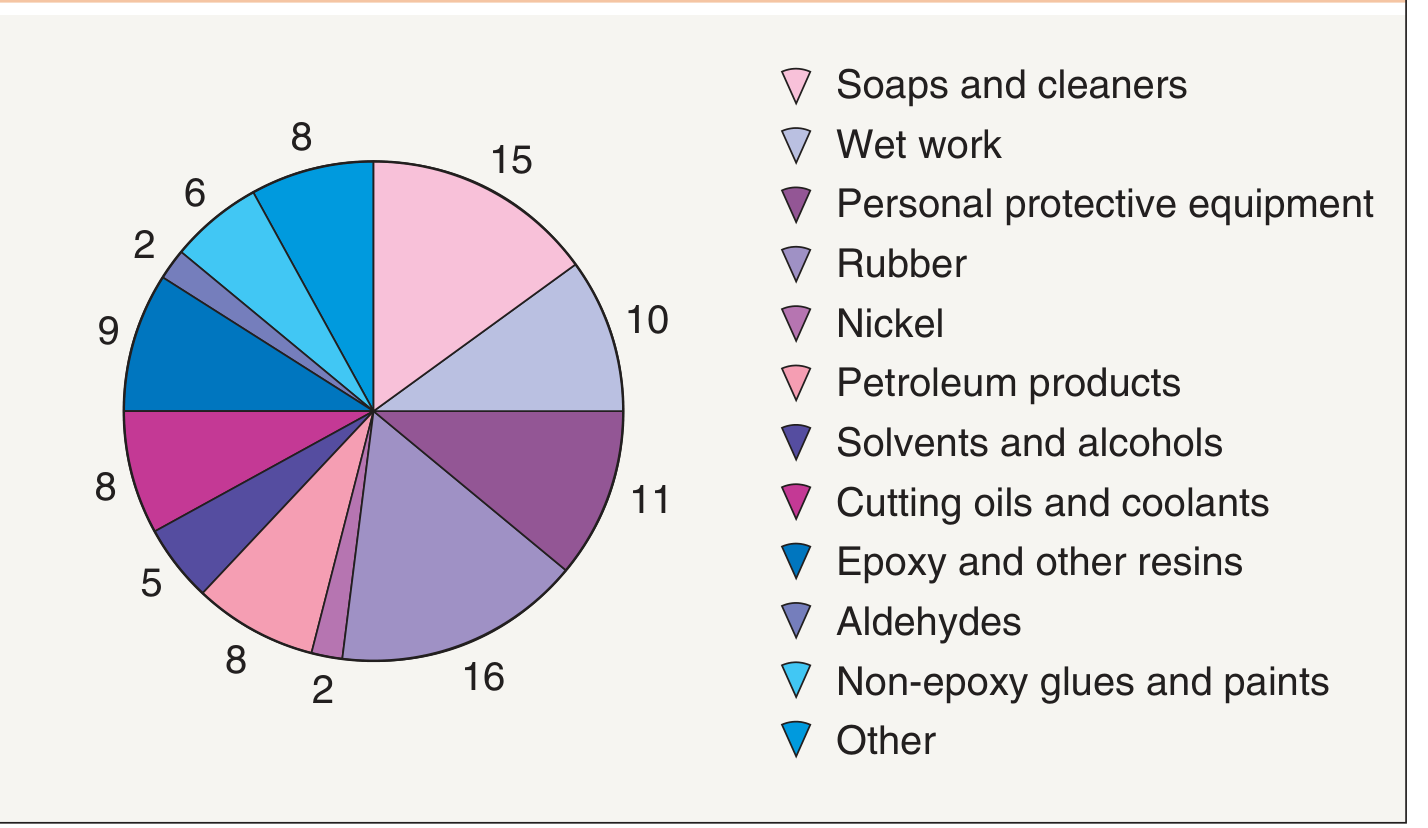
For Irritant CD:
| Causative Agent | % of UK Cases |
|---|---|
| Soaps and cleaners | 15% |
| Wet work | 16% |
| Petroleum products | 9% |
| Solvents and alcohols | 8% |
| Cutting oils and coolants | 8% |
| Epoxy and other resins | 9% |
| Non-epoxy glues/paints | 6% |
| Aldehydes | 5% |
| PPE-related | ~2% |
For Allergic CD - Most common occupational allergens (surveillance data):
- Rubber: 23.4% of cases
- Nickel: 18.2%
- Epoxy and other resins: 15.6%
- Aromatic amines: 8.6%
- Chromate: 8.1%
- Fragrances and cosmetics: 8.0%
- Preservatives: 7.3%
Key allergens by occupation (Andrews'): Carba mix, thiuram mix, epoxy resin, formaldehyde, nickel. Epoxy resin is disproportionately overrepresented in occupational referrals.
- Dermatology 2-Volume Set 5e, p. 341-342; Andrews' Diseases of the Skin
Biological Causes
- Bacteria (Staphylococcus, Erysipelothrix, Bacillus anthracis)
- Fungi (Trichophyton, Candida)
- Mycobacteria (M. marinum - fish tank granuloma)
- Plant products (psoralens - phototoxic; Toxicodendron - ACD)
High-Risk Occupations
| Sector | Common Exposures |
|---|---|
| Healthcare workers | Glutaraldehyde, formaldehyde, quaternium-15, thiuram (rubber gloves), latex |
| Hairdressers | p-Phenylenediamine (PPD), glycerol monothioglycolate, persulfates, thioglycolates |
| Machinists / Construction | Cutting oils, chromate (cement), epoxy resins |
| Food handlers / Bartenders | Wet work, Candida, food proteins (contact urticaria) |
| Agriculture / Forestry | Psoralens (phototoxic), pesticides, plants (urushiol) |
| Nail technicians | Methacrylates (rising prevalence due to artificial nails) |
| Custodians / Housecleaners | Soaps, disinfectants |
| Welders / Outdoor workers | UV radiation, skin cancer risk |
| Pilots / Cabin crew | UV at altitude - 2-3x higher UV exposure; twice the melanoma rate vs. general population |
Statistics: Agriculture, forestry, and fishing have the highest incidence of occupational skin disease. Manufacturing and healthcare sectors contribute many cases.
- Fitzpatrick's, p. 470-474; Andrews', p. 1200
Pathophysiology
Irritant Contact Dermatitis
- Direct disruption of the epidermal barrier by the irritant
- Causes release of cytokines (TNF-α, IL-1β, IL-6, IL-8) from keratinocytes
- Results in non-specific inflammation without immune memory
- Effects can be visible within minutes to hours
- Cumulative ICD: most common occupational pattern - repeated sub-threshold exposures to weak irritants (e.g., wet work) gradually lower the irritation threshold until dermatitis appears
- Filaggrin gene mutations markedly increase risk
- More than 57,000 chemicals known to cause ICD
Allergic Contact Dermatitis
- Type IV (delayed) hypersensitivity reaction
- Sensitization phase: hapten penetrates skin → binds to carrier proteins → processed by Langerhans cells → presented to T-lymphocytes → sensitized T-cells
- Elicitation phase: re-exposure → rapid T-cell response → inflammatory cascade
- Requires prior exposure; reaction appears 12-72 hours after re-exposure
- Only ~3700 chemicals are true sensitizers
Clinical Features
ICD - Clinical Spectrum
| Form | Trigger | Features |
|---|---|---|
| Acute ICD | Single strong irritant (acids, alkalis) | Chemical burn; erythema, vesicles, erosions, ulceration; sharp margins matching contact area |
| Cumulative (chronic) ICD | Repeated weak irritants | Dryness, fissuring, lichenification, scaling; indolent onset; worst on dorsal hands |
| Subjective irritation | Invisible irritants | Stinging/burning without visible changes |
ACD - Clinical Features
- Pruritus (prominent), erythema, vesicles, weeping in acute phase
- Lichenification, fissuring, hyperpigmentation in chronic phase
- Site: Hands affected in 60% of ACD and 80% of ICD cases
- Spread beyond the primary contact site is common in ACD (airborne distribution pattern from paint sprayers, for example)
- Important clue: improvement during holidays/weekends away from work
Both ICD and ACD may present as:
- Acute, subacute, or chronic dermatitis
- Dyshidrotic (pompholyx) pattern (classically described in chromate allergy from cement)
- Discoid pattern
Differential Diagnosis
- Tinea manuum - may mimic hand dermatitis (especially post-steroid use); check KOH
- Scabies - interdigital involvement can simulate ICD
- Psoriasis - keratotic plaques on palms; nail involvement/IPJ plaques are clues; may be exacerbated by workplace trauma (Koebner)
- Porphyria cutanea tarda - blistering on dorsal hands (rarely mistaken for contact dermatitis)
- Endogenous eczema - coexisting atopic/dyshidrotic eczema, often multifactorial
- Dermatology 2-Volume Set 5e, p. 345
Contact Urticaria (Occupational)
A distinct entity from contact dermatitis:
- Immunologic contact urticaria (ICU): IgE-mediated; onset within 15-20 min; can progress to systemic anaphylaxis. Classic example: latex allergy in healthcare workers.
- Non-immunologic contact urticaria (NICU): No prior sensitization; localized; less severe; not inhibited by H1 antihistamines; responds to NSAIDs (prostaglandin pathway).
- Protein contact dermatitis: Chronic eczematous dermatitis with intermittent urticaria from protein exposure (food handlers, veterinary workers).
- SPT/prick testing (not patch testing) is used to diagnose immunologic contact urticaria.
- Fitzpatrick's, p. 474-480
Diagnosis
Occupational History (Key Points)
The diagnosis is fundamentally clinical and historical. Key factors to address:
| History Element | Significance |
|---|---|
| Primary site (hands in 90%) | Consistent with occupational exposure? |
| Time course | Temporal relation to work? |
| Materials handled | MSDS for irritant/sensitizer data |
| Others affected similarly | Suggests ICD (rather than ACD) |
| PPE used | Appropriate? Could PPE itself be the allergen? |
| Improvement on weekends/holidays | Strong clue for occupational cause |
| History of atopy | Increased ICD risk (especially filaggrin mutations) |
| Hobbies | May be the true cause |
- Dermatology 2-Volume Set 5e, Table 16.2
Patch Testing (for ACD)
- Essential for any individual with potentially work-related dermatitis or for whom a job change is being considered
- Standard series + work-specific materials must be included (not all allergens are commercially available; MSDS may not disclose all ingredients)
- Testing 5200 chemicals with appropriate concentrations is feasible (guide published)
- When a reaction occurs to an unknown substance: dilutional series + testing ~20 controls confirms allergic vs. irritant reaction
- Applied to upper back; read at 48h and 96h (D2 and D4)
- Dermatology 2-Volume Set 5e, p. 342
Other Investigations
- KOH preparation - exclude tinea
- Skin biopsy - non-specific eczematous changes (spongiosis); may show birefringent fibers in fiberglass dermatitis under polarized light
- Skin prick test / SPT - for contact urticaria (IgE-mediated)
- RAST / fluorescence enzyme-labeled assay (FELA) - specific IgE measurement (RAST is largely replaced by FELA); used for ICU diagnosis
- Workplace visit - invaluable when occupational cause is suspected but not established from history alone
- Biomonitoring - e.g., urine arsenic speciation for arsenic exposure (inorganic arsenic is toxic; organic arsenobetaine is not)
- Fitzpatrick's, p. 479-481
Special Topics
Fiberglass Dermatitis
- Mechanism: direct mechanical penetration (proportional to fiber diameter >3.5 µm; inversely proportional to length)
- Features: pruritus, erythematous papules with follicular accentuation on exposed/forearm areas; paronychia common
- Diagnosis: tape stripping or KOH examination of skin scrapings
- Rapidly resolves after cessation of exposure; hardening occurs in most workers within weeks
- Dermatology 2-Volume Set 5e, p. 344
Chemical Burns (Occupational)
- Strong acids (sulfuric, nitric, HCl): coagulative necrosis; form barrier limiting penetration
- Hydrofluoric acid: liquefactive necrosis; penetrates to bone; pain lasting days; systemic toxicity if >1% BSA affected; treat with 2.5% calcium gluconate gel
- Strong alkalis (NaOH, wet cement): saponification of fatty acids → penetrate deeper than most acids; severe damage
- Phenolic compounds: nerve damage causing anesthesia without visible injury
- Initial treatment: copious irrigation with water; soap solution for water-insoluble chemicals; specific antidotes where available
- Dermatology 2-Volume Set 5e, p. 343-344
Occupational Skin Cancer
- UV radiation (natural + artificial) is the dominant cause
- UV increases 10-12% per 1000m altitude - airline pilots/cabin crew have 2-3x UV exposure at cruising altitude and twice the melanoma rate vs. general population
- Outdoor workers (agriculture, construction, fishing, landscaping) at highest risk
- Arsenic: occupational carcinogen; inorganic arsenic in urine is the reliable biomarker
- Fitzpatrick's, p. 477-478
Phototoxic Dermatitis
- Most occupational photosensitivity is phototoxic (not photoallergic)
- Common scenario: outdoor workers exposed to plant psoralens ("strimmer dermatitis" - plant sap splatter on inadequately protected skin)
- Coal tar/creosote: "tar/pitch smarts" - burning/stinging within 15 min of sun exposure
- Resolves with hyperpigmentation
- Dermatology 2-Volume Set 5e, p. 344
Management
Primary Prevention (Avoid Disease Onset)
- Engineering measures: enclose processes, improve ventilation, substitute less hazardous chemicals
- Chemical substitution: replace strong sensitizers/irritants with safer alternatives
- Pre-employment screening: exclude workers with severe childhood atopic dermatitis (especially with hand involvement) from "wet work" jobs; recommend "dry" work
- Education: workforce education in skin care reduces skin disease incidence (evidence-based)
Secondary Prevention (Early Detection)
- Health surveillance: periodic medical examination of all workers for early detection
- Prompt reporting of any skin irritation, however mild
Tertiary Prevention (Treatment of Active Disease)
General measures:
- Eliminate or reduce exposure - most important step
- Appropriate PPE: gloves (select correct type per MSDS/manufacturer; replace regularly; each glove type has a defined penetration time for specific chemicals)
- Acrylate glues, PPD (hair dye), glycerol monothioglycolate - rapidly penetrate latex gloves
- Cotton inner liner if prolonged glove wear
- Avoid rings (chemicals accumulate underneath)
- Hand washing: use lukewarm water, dry thoroughly, attend to fingerweb spaces
- Barrier creams: for wet work (against acids, alkalis, water-based fluids) and dry work (against oils, greases, resins)
- Emollients: frequent application throughout the day
Medical treatment:
- Acute phase: topical corticosteroids (mainstay)
- Dry, fissured hands: soak in water 20 min at night → apply triamcinolone 0.1% ointment immediately (without drying) → hydrates and heals
- Maintenance: topical tacrolimus ointment, pimecrolimus cream + high-lipid content moisturizing creams
- Oral corticosteroids for severe acute ACD
- Andrews', p. 1207-1208; Dermatology 2-Volume Set 5e, Table 16.4-16.5
Prognosis
The prognosis for occupational contact dermatitis is poor once established:
| Outcome | Proportion |
|---|---|
| Heal completely | ~1/4 to 1/3 |
| Improve | ~1/3 to 1/2 |
| Same or worse | Remainder |
- ~10% develop persistent post-occupational dermatitis despite no identifiable ongoing cause
- Job change improves prognosis but does not guarantee resolution (new workplace may have same exposures; domestic exposure may perpetuate ACD)
- Prognosis is worse when allergen is present in both occupational AND domestic environments
Factors predicting poor prognosis:
- Atopic patients
- Males with chromate allergy
- Females with nickel allergy
- Delay in diagnosis before treatment
- Construction industry workers
Factors predicting better prognosis:
- ICD from metalworking fluids
- Urushiol ACD in foresters
- ACD to acrylic monomers or amine curing agents
- Andrews', p. 1212; Dermatology 2-Volume Set 5e, p. 345
Medicolegal Aspects
- Occupational dermatitis has significant compensation and workers' disability implications
- Material Safety Data Sheets (MSDS) are legal documents that must disclose chemical composition and hazards (irritant, corrosive, sensitizer)
- Limitations of MSDS: may not list all relevant ingredients; manufacturer communication may be necessary
- Workplace visits and patch testing with work materials may be required for legal proceedings
- Systematic health surveillance in industry is often a statutory obligation (e.g., under the Factories Act - adequate washing facilities)
- Park's Textbook of Preventive and Social Medicine; Dermatology 2-Volume Set 5e
Summary Table: ICD vs. ACD at a Glance
| Feature | ICD | ACD |
|---|---|---|
| Mechanism | Non-immunologic; cytotoxic | Type IV (delayed) hypersensitivity |
| Prior sensitization | Not required | Required |
| Incidence | More common | Less common |
| Pruritus | Less prominent | Prominent |
| Progression | Within minutes to hours | 12-72 hours after exposure |
| Affected individuals | Anyone; compromised barrier at higher risk | Only genetically susceptible individuals |
| Patch test | Negative (may give irritant reaction) | Positive |
| Spread beyond contact area | Unusual | Common (esp. airborne) |
| No. of causative chemicals | >57,000 irritants | ~3700 allergens |
| Hands affected | 80% | 60% |
Sources: Fitzpatrick's Dermatology Vol. 1&2, p. 468-481; Dermatology 2-Volume Set 5e, p. 341-346; Andrews' Diseases of the Skin, p. 1200-1213; Park's Textbook of Preventive and Social Medicine, p. 4891-4903
This is a shared conversation. Sign in to Orris to start your own chat.