Explain and give notes of coronary circulation from guyton and hall textbook of physiology
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have all the content needed from Guyton and Hall. Let me compile the comprehensive notes.
Coronary Circulation
Guyton and Hall Textbook of Medical Physiology - Chapter 21
1. Introduction
About one-third of all deaths in industrialized Western countries result from coronary artery disease, and most older adults have at least some impairment of the coronary circulation. Understanding the physiology of coronary circulation is therefore one of the most important subjects in medicine.
2. Physiological Anatomy of the Coronary Blood Supply
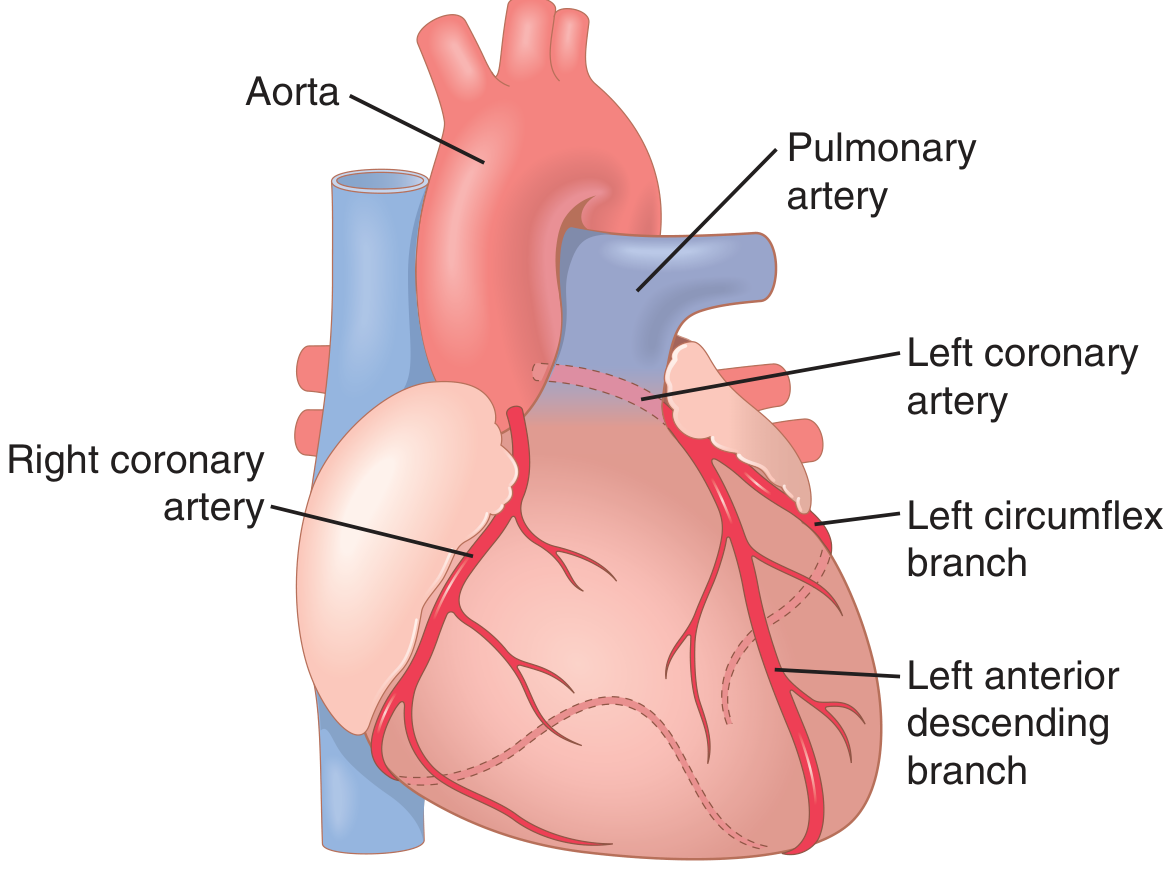
Key anatomical points:
- The main coronary arteries lie on the surface of the heart (epicardial). Smaller arteries penetrate from the surface into the muscle mass.
- Only the inner 0.1 mm of the endocardial surface can obtain nutrition directly from blood inside the cardiac chambers - this source is miniscule.
Left Coronary Artery (LCA)
- Supplies the anterior and left lateral portions of the left ventricle
- Divides into:
- Left anterior descending (LAD) branch
- Left circumflex branch
Right Coronary Artery (RCA)
- Supplies most of the right ventricle
- Supplies the posterior part of the left ventricle in 80-90% of people (right dominance)
Coronary Venous Drainage
| Vessel | Source | Drains Into |
|---|---|---|
| Coronary sinus | ~75% of LV venous blood | Right atrium |
| Anterior cardiac veins | RV muscle | Right atrium directly |
| Thebesian veins | Minute, all areas | All chambers of the heart |
3. Normal Coronary Blood Flow
- Resting coronary blood flow: ~70 mL/min/100 g of heart weight = approximately 225 mL/min total
- This is about 4-5% of total cardiac output
- Coronary blood flow per gram heart weight is typically higher in women than in men
During strenuous exercise:
- Cardiac output increases 4- to 7-fold
- Work output of the heart may increase 6- to 9-fold
- Coronary blood flow must increase proportionately to supply the needed oxygen
4. Phasic Changes in Coronary Blood Flow (Systole vs Diastole)
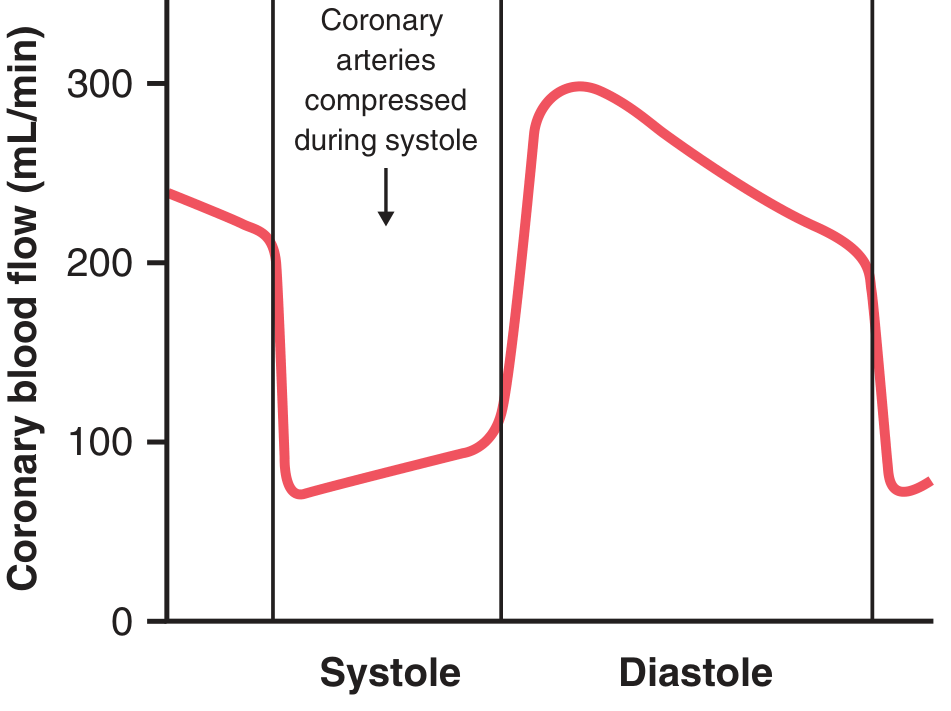
- During systole: LV coronary capillary flow falls to a low value - opposite to other vascular beds. This is because the intramuscular blood vessels are compressed by left ventricular contraction.
- During diastole: Muscle relaxes, no longer obstructs flow - blood flows rapidly throughout diastole.
- Right ventricle: Also shows phasic changes, but only partial because RV contraction force is much less than LV.
Key Exam Point: Unlike most other organs, the left ventricle is perfused primarily during diastole, not systole.
5. Epicardial vs Subendocardial Blood Flow
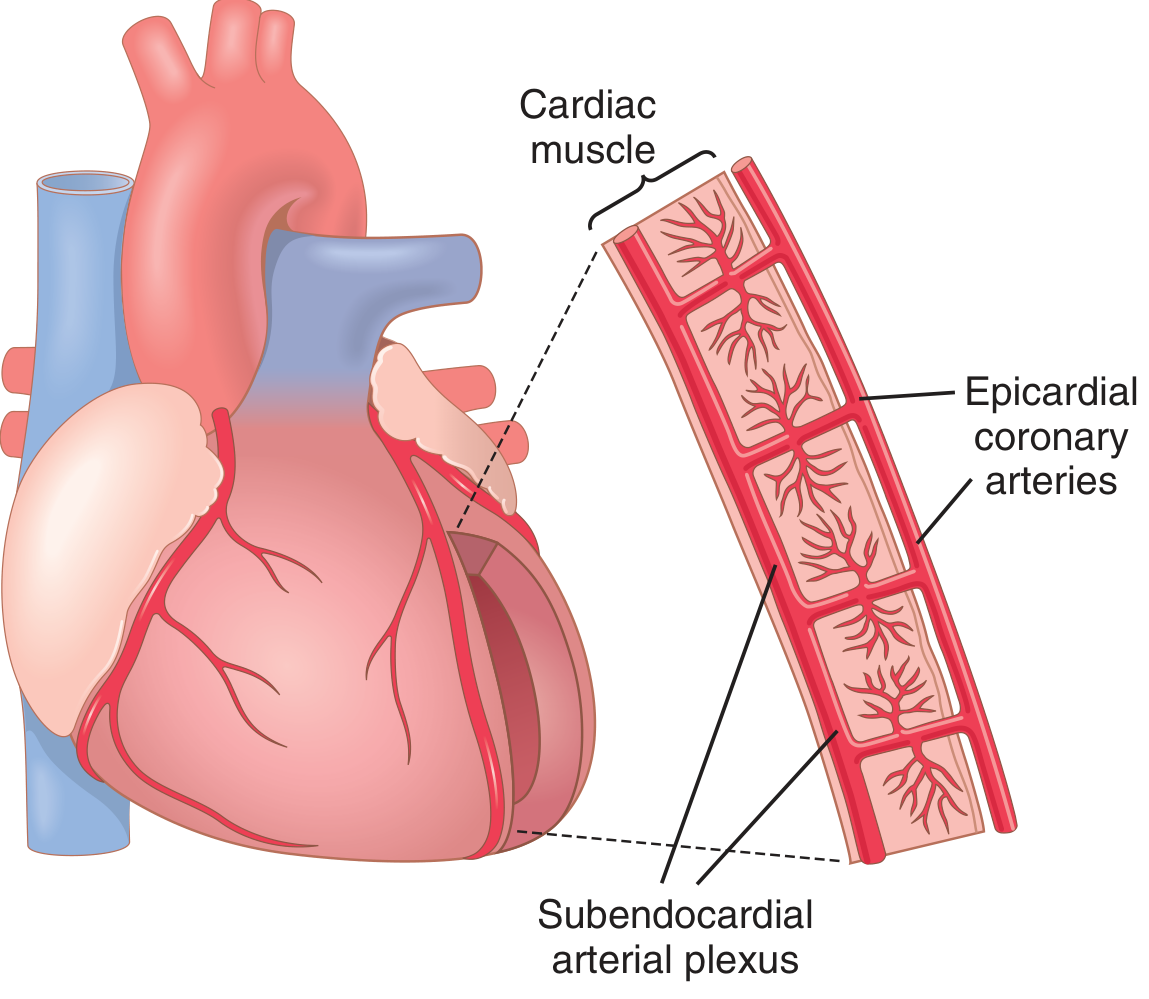
- Epicardial coronary arteries - on the outer surface, supply most of the muscle
- Intramuscular arteries - penetrate the muscle from epicardial vessels
- Subendocardial arterial plexus - lies immediately beneath the endocardium
During systole, subendocardial vessels are more susceptible to compression. The extra vessels of the subendocardial plexus normally compensate for this. This difference plays a key role in certain types of coronary ischemia (subendocardial infarction).
6. Control of Coronary Blood Flow
6a. Local Metabolic Control (PRIMARY Mechanism)
Coronary blood flow is regulated mainly by local arteriolar vasodilation in response to myocardial metabolic needs.
Oxygen demand is the major factor:
- Normally, about 70% of oxygen in coronary arterial blood is extracted as blood passes through the heart (very high extraction ratio compared to other organs)
- Because so little oxygen remains, the only way to supply more O2 is to increase blood flow
- Coronary blood flow increases almost directly proportional to oxygen consumption
Vasodilator substances released by metabolic activity:
| Substance | Mechanism |
|---|---|
| Adenosine (most important) | ATP degrades → AMP → adenosine; potent vasodilator |
| Adenosine phosphate compounds | Direct vasodilation |
| Potassium ions | Hyperpolarize smooth muscle |
| Hydrogen ions | Local vasodilation |
| Carbon dioxide | Vasodilation |
| Prostaglandins | Vasodilation |
| Nitric oxide | Direct vasodilator via smooth muscle relaxation |
Note: Adenosine, after causing vasodilation, is largely reabsorbed into cardiac cells to be reused for ATP production. In severe ischemia (lasting >30 minutes), about half of the adenine base can be lost from affected cells, and new synthesis is only ~2%/hour - this is a major cause of cellular death in myocardial infarction.
6b. Nervous Control of Coronary Blood Flow
Autonomic nerves have direct and indirect effects:
Indirect effects (more important):
- Sympathetic stimulation → increases heart rate and contractility → increases cardiac metabolism → causes local vasodilation → increases coronary flow proportional to metabolic needs
- Vagal stimulation → slows heart, depresses contractility → decreases O2 consumption → indirectly constricts coronary arteries
Direct effects:
- Parasympathetic (vagal): Parasympathetic distribution to ventricular coronary system is sparse. Acetylcholine has a direct vasodilatory effect on coronary vessels.
- Sympathetic (alpha-adrenergic): Norepinephrine activates alpha-adrenergic receptors → slight coronary vasoconstriction
- Sympathetic (beta-adrenergic): Also activates beta-adrenergic receptors → coronary vasodilation
- Net result: In the normal heart, indirect metabolic effects dominate, so sympathetic stimulation overall increases coronary flow.
7. Ischemic Heart Disease
The most common cause of death in men and women in Western countries. About 35% of Americans aged 65 and older die of ischemic heart disease. It encompasses both obstructive and nonobstructive coronary artery disease.
7a. Atherosclerosis
- Most common cause of diminished coronary flow
- Gradual cholesterol deposition beneath the endothelium, invaded by fibrous tissue, often calcified
- Forms atherosclerotic plaques that protrude into vessel lumens
- Common site: first few centimeters of major coronary arteries
- Women have lower prevalence of obstructive atherosclerosis than men, but sex differences are attenuated in older adults
- Coronary microvascular dysfunction and coronary vasospasm are also causes when no obstruction is detectable
7b. Acute Coronary Artery Occlusion
Acute occlusion usually occurs in a person with underlying atherosclerotic disease. Two main causes:
-
Thrombosis: Atherosclerotic plaque breaks through endothelium → platelets adhere → fibrin deposited → thrombus forms and occludes vessel. If the clot breaks away and travels distally = coronary embolus
-
Coronary artery spasm: Smooth muscle spasm due to:
- Irritation by atherosclerotic plaque edges
- Local nervous reflexes
- Extreme emotional stress
- Stimulant drugs (cocaine, amphetamines)
- Tobacco use
- Cold exposure
- Spasm may lead to secondary thrombosis
- Treated with calcium channel blockers or nitrate drugs
7c. Collateral Circulation - Lifesaving Value
- Normal hearts have almost no large communications between major coronary arteries
- Many anastomoses exist among smaller arteries (20-250 micrometers diameter)
Time course of collateral development after acute occlusion:
| Time | Collateral Response |
|---|---|
| Within seconds | Small anastomoses begin to dilate |
| First 8-24 hours | Little enlargement - flow still <50% of needs |
| Day 2-3 | Collateral flow begins doubling |
| ~1 month | Near-normal coronary flow restored |
When atherosclerosis develops slowly over years, collaterals can develop simultaneously - the patient may never experience an acute episode. However, when the sclerotic process exceeds the collateral supply, severe cardiac failure results.
8. Myocardial Infarction (MI)
8a. Immediate Effects
- Small ischemic area: Little or no muscle cell death; muscle becomes temporarily nonfunctional
- Large ischemic area:
- Center: cells die within 1-3 hours (total cessation of blood supply)
- Around dead area: nonfunctional zone (failure of contraction and impulse conduction)
- Outer rim: weakly contracting zone (mild ischemia)
8b. Stages of Recovery
- Dead muscle fibers at center → area enlarges over days as marginal fibers succumb
- Developing collaterals supply the outer rim → some nonfunctional muscle recovers
- After a few days to 3 weeks: nonfunctional muscle either recovers or dies
- Fibroblasts grow into dead tissue → fibrous scar forms (ischemia stimulates fibroblast growth)
- Fibrous scar undergoes progressive contraction over months to a year
- Normal heart areas gradually hypertrophy to compensate
8c. Role of Rest in Recovery
- Excessive cardiac activity causes vessels of normal muscle to dilate greatly
- This diverts blood away from the ischemic area through small anastomotic channels - this is called the coronary steal syndrome
- Therefore, absolute body rest during the initial acute phase is critical
- However, progressive physical activity (cardiac rehabilitation) during recovery improves coronary blood flow and promotes formation of new collateral vessels
8d. Loss of Adenine in Ischemia (Cellular Mechanism)
In severe coronary ischemia:
- ATP → ADP → AMP → adenosine (leaks out of cells)
- Within 30 minutes, ~50% of adenine base can be lost from ischemic cells
- New adenine synthesis = only 2%/hour
- Once ischemia persists >30 minutes, relief may be too late to prevent cell death
9. Summary of Key Numbers to Remember
| Parameter | Value |
|---|---|
| Resting coronary blood flow | ~225 mL/min (~70 mL/min/100 g) |
| % of cardiac output | 4-5% |
| O2 extraction from coronary blood | ~70% |
| Endocardial direct nutrition depth | 0.1 mm |
| Time to significant cell death in total occlusion | 1-3 hours |
| Adenine loss after 30 min ischemia | ~50% |
| Adenine synthesis rate | ~2%/hour |
| Collateral flow normalization time | ~1 month |
| Cardiac output increase during strenuous exercise | 4- to 7-fold |
| Cardiac work increase during severe exercise | 6- to 9-fold |
Source: Guyton and Hall Textbook of Medical Physiology, Chapter 21 - "Coronary Circulation and Ischemic Heart Disease"
This is a shared conversation. Sign in to Orris to start your own chat.