Make me understand osteoarthritis vs rheumatoid arthritis
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
Find recent clinical guidelines on both
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
Make me understand osteoarthritis vs rheumatoid arthritis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"osteoarthritis"[MeSH Terms] AND "guidelines"
Searching PubMed
"rheumatoid arthritis"[MeSH Terms] AND "guidelines"
Reading File
Reading File
Searching PubMed
"rheumatoid arthritis"[MeSH Terms] AND treatment AND management
Finding Sources
Searching PubMed
"rheumatoid arthritis" AND "treat to target" AND management
Reading File
Reading File
Loading Image
Reading Article
PMID: 41826212
I now have excellent material from Robbins Pathology, Goldman-Cecil, and the very latest EULAR 2025 guidelines for RA. Let me compile the full comprehensive answer.
Osteoarthritis vs. Rheumatoid Arthritis
Here is a thorough, side-by-side breakdown of both conditions - from mechanism to management - using Robbins Pathology, Goldman-Cecil Medicine, and the freshest clinical guidelines.
The Core Difference
The most important thing to understand upfront: OA is degenerative, RA is autoimmune.
- OA = mechanical wear and tear of articular cartilage, with inflammation playing only a secondary role
- RA = the immune system attacks the synovial membrane, causing primary inflammation that then destroys cartilage and bone
Side-by-Side Comparison (Robbins Pathology Table 19.2)
| Feature | Osteoarthritis (OA) | Rheumatoid Arthritis (RA) |
|---|---|---|
| Primary mechanism | Mechanical injury to cartilage | Autoimmunity |
| Role of inflammation | Secondary - worsens damage | Primary - T cells & antibodies cause destruction |
| Joints involved | Weight-bearing (knees, hips, spine) | Starts in small joints of fingers & toes; spreads to multiple joints symmetrically |
| Pathology | Cartilage degeneration, osteophytes, subchondral cysts; minimal inflammation | Inflammatory pannus invading cartilage; severe chronic inflammation; joint fusion (ankylosis) |
| Serum antibodies | None | Rheumatoid factor (RF), ACPA (anti-CCP) |
| Other organs affected | No | Yes - lungs, heart, blood vessels, skin |
| Age of onset | Typically >50 years | Peak in 3rd-5th decades |
| Sex distribution | Slightly more in women (Heberden nodes) | 3x more common in women |
| Morning stiffness | Brief (<30 min) | Prolonged (>1 hour) |
| Joint fusion | Does NOT occur | Can occur (ankylosis) |
Joint Morphology Comparison
Here is what the joints actually look like in each disease (from Robbins Pathology Fig. 19.33):
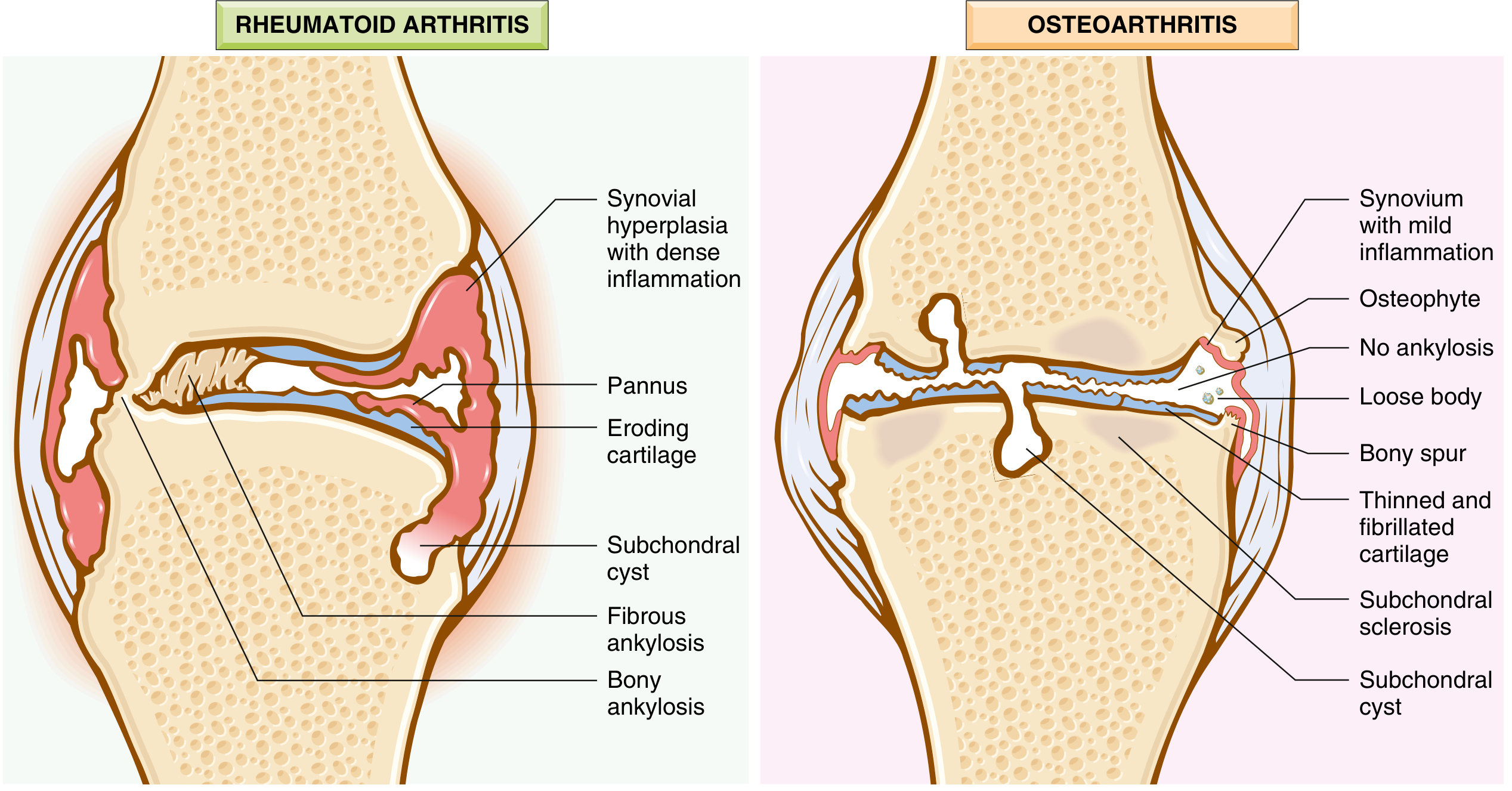
In RA (left): The synovium undergoes massive hyperplasia with dense inflammation. A "pannus" - a destructive tissue made of inflammatory cells and fibroblasts - actively erodes the cartilage. Eventually, fibrous and then bony ankylosis can lock the joint entirely.
In OA (right): Cartilage thins and fibrillates (frays). Osteophytes (bony spurs) grow at joint margins. Loose bodies (fragments of cartilage/bone) float in the joint. The subchondral bone scleroses. The synovium shows only mild inflammation.
Pathogenesis in Detail
Osteoarthritis
Biomechanical stress is the principal driver. Chondrocytes respond to injury by releasing matrix metalloproteinases (MMPs) that degrade type II collagen - the repair response is overwhelmed by continued destruction. Key stages:
- Early OA: Chondrocyte proliferation, MMP secretion, cartilage surface fibrillation
- Late OA: Full-thickness cartilage loss, subchondral bone exposure and eburnation ("polished ivory" appearance), subchondral cysts, osteophyte formation
Risk factors include age (prevalence ~40% in those over 70), obesity, prior joint injury, and genetic susceptibility.
- Robbins & Kumar Basic Pathology, p. 790
Rheumatoid Arthritis
The trigger is CD4+ T cell activation against joint antigens (especially citrullinated peptides). Key mediators:
- TNF, IL-1, IL-6 (from macrophages): activate leukocytes and proteases that destroy cartilage. TNF is the most critical mediator - this is why TNF inhibitors are highly effective.
- IL-17 (from Th17 cells): recruits neutrophils and monocytes
- RANKL (from activated T cells): stimulates osteoclasts causing bone resorption
- ACPA (anti-CCP antibodies): present in up to 70% of patients; the modified citrullinated epitopes come from fibrinogen, type II collagen, alpha-enolase, and vinculin
- Rheumatoid factor (RF): IgM/IgA autoantibodies against the Fc portion of IgG; present in ~80% of patients
Genetic association: HLA-DR4 is strongly linked to ACPA-positive RA. Environmental triggers like smoking and periodontitis can promote citrullination of self-proteins, setting off the autoimmune cascade.
- Robbins & Kumar Basic Pathology, pp. 792-793
Clinical Features
Osteoarthritis
- Pain that worsens with use, improves with rest
- Brief morning stiffness (<30 minutes)
- Crepitus on movement
- Heberden nodes (osteophytes at distal interphalangeal joints) - more common in women
- Bouchard nodes (osteophytes at proximal interphalangeal joints)
- Cervical/lumbar osteophytes can compress nerve roots - causing radicular pain, muscle atrophy, neurological deficits
- X-ray: joint space narrowing, subchondral sclerosis, osteophytes, subchondral cysts
- No systemic features
Rheumatoid Arthritis
- Symmetric polyarthritis of small joints (MCPs, PIPs, wrists) - the classic "squeeze test" is positive
- Prolonged morning stiffness (>1 hour) - a hallmark
- Soft, boggy swelling of joints (from synovial thickening and effusion)
- Systemic features: fatigue, weight loss, low-grade fever
- Extra-articular: rheumatoid nodules (subcutaneous, at pressure points), interstitial lung disease, pericarditis, vasculitis, scleritis, Felty syndrome (splenomegaly + leukopenia)
- X-ray: periarticular osteopenia, joint space narrowing, marginal erosions (classic), no osteophytes
- Labs: elevated ESR/CRP, positive RF and/or anti-CCP (ACPA), possible anemia of chronic disease
Management
Osteoarthritis - Core Recommendations
Per systematic review of clinical practice guidelines (PMID: 37394226 and 36762545), the consistently recommended elements across all major guidelines are:
- Exercise and physical therapy - the single most evidence-based intervention (land-based, aquatic, and resistance training all benefit)
- Weight loss - for hip/knee OA in overweight patients
- NSAIDs - topical (preferred for knee OA, fewer systemic effects) or oral
- Intra-articular corticosteroid injections - for acute flares
- Duloxetine - recommended by many guidelines for pain modulation
- Joint replacement - when functional status is severely impaired and conservative measures fail (Goldman-Cecil Medicine, Chapter 241/255)
There are no disease-modifying treatments for OA - no drug currently prevents or halts cartilage loss.
Rheumatoid Arthritis - EULAR 2025 Guidelines (freshest evidence)
The brand-new EULAR 2025 update (PMID: 41826212, published June 2026) provides the current gold standard. Key recommendations:
Overarching strategy: Treat-to-Target (T2T) - aim for clinical remission or low disease activity
- First line: Methotrexate (MTX), ideally combined with short-term glucocorticoids
- If insufficient response after 3-6 months: Add a biologic DMARD (bDMARD):
- TNF inhibitors (adalimumab, etanercept, infliximab, certolizumab, golimumab)
- IL-6 inhibitors (tocilizumab, sarilumab)
- T-cell co-stimulation blocker (abatacept)
- B-cell depletion (rituximab)
- JAK inhibitors (JAKi) (tofacitinib, baricitinib, filgotinib, upadacitinib) - may be considered after bDMARD, but require careful cardiovascular and malignancy risk assessment (new safety emphasis in 2025 update)
- If first bDMARD or JAKi fails: Switch to any other bDMARD (same or different class) or JAKi
- Tapering: Once sustained remission is achieved, DMARDs may be tapered - but stopping often causes flare, so caution is needed
- Other DMARDs: leflunomide, sulfasalazine also remain options
Quick Memory Aid
| OA | RA | |
|---|---|---|
| Think of it as... | "Worn out joints" | "Immune system attacking joints" |
| Key finding on X-ray | Osteophytes + sclerosis | Marginal erosions + osteopenia |
| Blood tests | Normal | RF+, anti-CCP+, high ESR/CRP |
| Treatment target | Symptom relief only | Remission (T2T with DMARDs) |
| Systemic disease | No | Yes |
Sources:
- Robbins & Kumar Basic Pathology, pp. 789-795 (Table 19.2, Figs. 19.31-19.34)
- Goldman-Cecil Medicine (International Ed.), Chapter 241
- EULAR 2025 RA Management Recommendations - Smolen JS et al., Ann Rheum Dis 2026 Jun (PMID 41826212)
- OA Guidelines Systematic Review - Gibbs AJ et al., Osteoarthritis Cartilage 2023 (PMID 37394226)
- Core OA Recommendations - Conley B et al., Arthritis Care Res 2023 (PMID 36762545)
This is a shared conversation. Sign in to Orris to start your own chat.