Teach me pitrysis rosea
"pityriasis rosea"[MeSH Terms]
Pityriasis Rosea
Definition
Epidemiology
- Worldwide distribution; all races affected
- Incidence: ~160 cases per 100,000 person-years (US data); 0.64 per 100 dermatologic patients globally
- Peak age: 10 to 35 years (cases reported from 3 months to 83 years)
- Slight female predominance (F:M ratio ~1.39:1)
- Possible seasonal clustering (some studies show more cases in spring and autumn)
- Relapse is uncommon: 1.8-3.7%
Etiology and Pathogenesis
- HHV-7 DNA has been found in lesional skin, peripheral blood mononuclear cells, and plasma of PR patients, but not controls
- HHV-7 may trigger reactivation of latent HHV-6
- Both viruses are virtually universal in adults (HHV-6 seropositivity 80-100%; HHV-7 >85%), making causality difficult to prove definitively
- The eruption may represent either primary infection or reactivation leading to viremia
- HHV-2 and hepatitis C virus have also been implicated in isolated cases
Note: Case clustering, possible seasonal variation, and the resemblance to other viral exanthems all support an infectious cause.
Clinical Features
The Herald Patch (Primary Lesion)

- Present in 50-90% of patients
- A single, 3-5 cm oval erythematous scaly plaque on the trunk (rarely an extremity)
- Has a collarette of fine scale just inside the periphery (scale points inward)
- Precedes the generalized eruption by ~1-2 weeks in adults, ~4 weeks in children
- Commonly mistaken for tinea corporis because it appears as an isolated scaling plaque
Secondary Eruption
- Follows the herald patch by 1-2 weeks
- Smaller (0.5-1.5 cm) salmon-pink oval patches and plaques, mainly on the trunk and proximal extremities
- Long axis of lesions oriented parallel to skin cleavage lines (Langer's lines)
- On the back, this creates the classic "Christmas tree" or "fir tree" pattern
- Collarette of scale with the open (free) edge pointing inward - the "hanging curtain sign"
- Palms and soles are typically spared
- Face is usually spared (exception: children with darker skin)
Systemic Symptoms
- Mild pruritus (can be moderate-severe in some)
- Mild prodromal flu-like symptoms may precede the eruption in some patients
- These symptoms are transient
Atypical Variants
| Variant | Description |
|---|---|
| Papular variant | More common in children with darker skin; also more facial/scalp involvement |
| Vesicular variant | Vesicular lesions; can mimic chickenpox |
| Erythema multiforme-like | Target-like lesions |
| Purpuric variant | Petechiae/ecchymoses along Langer lines - may rarely be a sign of underlying leukemia |
| Inverse/localized | Confined to neck, axillae, groin, thighs |
| Unilateral | Asymmetric distribution |
| Giant PR | Very large plaques |
In darker-skinned patients, lesions often resolve leaving post-inflammatory hypopigmentation.
Histopathology
- Epidermal changes: Mounded parakeratosis with "liftoff," mild acanthosis, spongiosis
- Dermal changes: Superficial perivascular lymphocytic infiltrate, red blood cell extravasation (erythrocyte extravasation is a hallmark)
- Inflammatory infiltrate: predominantly lymphocytes, with neutrophils, histiocytes; occasional eosinophils
- Herald patch may show slightly deeper infiltrate and more acanthosis compared to secondary lesions
- Biopsy is non-specific but can help exclude other diagnoses
Diagnosis
- Herald patch
- Christmas tree distribution on trunk
- Oval lesions along skin cleavage lines
- Collarette of scale (free edge inward)
- Self-limited, 4-8 week course
Differential Diagnosis
| Condition | Key Distinguishing Features |
|---|---|
| Secondary syphilis (most important!) | Involves palms and soles, no herald patch, more widespread lymphadenopathy, condylomata lata; RPR positive |
| Tinea corporis | Scale at periphery (not collarette), KOH positive |
| Guttate psoriasis | Lesions don't follow cleavage lines; scale thick and silvery; no herald patch |
| Nummular dermatitis | More circular (not oval), tiny vesicles, no collarette |
| Pityriasis lichenoides chronica | More chronic, persistent crops, no herald patch, more confluent scale, extremity-predominant |
| Lichen planus | More pruritic, Wickham striae, distal extremity and mucous membrane involvement |
| Seborrheic dermatitis | Face and scalp involvement |
| Drug reaction | No herald patch, temporal relation to drug exposure |
Clinical pearl: Always rule out secondary syphilis, especially when palms and soles are involved - order a serology (RPR or VDRL).
Drug-Induced PR-like Eruptions
- ACE inhibitors (captopril, lisinopril)
- Imatinib mesylate
- Interferons
- Gold, bismuth, arsenicals
- Clonidine, barbiturates
- Ketotifen
- Adalimumab, lithium, acyclovir, ergotamine
Special Situation: PR in Pregnancy
- Associated with adverse pregnancy outcomes, particularly in the first trimester
- In PR onset before 15 weeks gestation: ~62% resulted in miscarriage in one study
- Can also be associated with premature delivery and neonatal hypotonia/hyporeactivity
- Women who develop PR during pregnancy, especially in the first trimester, should be monitored closely
Treatment
| Treatment | Role |
|---|---|
| Reassurance | Explain self-limited nature (6-8 weeks) |
| Topical corticosteroids (e.g., triamcinolone 0.1% cream) | Reduce pruritus |
| Oral antihistamines | Reduce pruritus |
| Emollients (petroleum jelly-based) | Skin barrier support |
| UVB phototherapy or natural sunlight | May speed resolution of lesions |
| Acyclovir (high-dose) | May hasten recovery and reduce symptoms in severe or widespread cases; most evidence is for 400-800 mg 5x/day for 1 week |
| Macrolides (e.g., erythromycin) | NOT indicated - earlier evidence was not confirmed |
Acyclovir is considered when: widespread eruption, severe pruritus, significant systemic symptoms, or pregnancy (to potentially reduce adverse outcomes). It is most beneficial if started early in the course.
Prognosis and Complications
- Complete resolution in 6-8 weeks in most patients (range 4-16 weeks)
- No long-term complications in healthy individuals
- Can cause anxiety and depression in ~30% of cases due to uncertainty about the diagnosis
- Recurrence is uncommon (1.8-3.7%)
- Post-inflammatory hyperpigmentation or hypopigmentation may persist, especially in darker skin tones
Summary Table
| Feature | Details |
|---|---|
| Cause | Likely HHV-6/HHV-7 reactivation |
| Age | Peaks 10-35 years |
| First lesion | Herald patch (3-5 cm oval, collarette of scale) |
| Distribution | Trunk, proximal extremities; Christmas tree pattern |
| Duration | 4-8 weeks (self-limited) |
| Key DDx | Secondary syphilis (always rule out!) |
| Treatment | Symptomatic; acyclovir for severe cases |
| Pregnancy | Watch closely - risk of miscarriage in 1st trimester |
- Fitzpatrick's Dermatology (Chap. 31), pp. 550-554
- Andrews' Diseases of the Skin, p. 1915
- Goldman-Cecil Medicine, p. 4280
- Tintinalli's Emergency Medicine, p. 1679
Hey there was a patient whose mesotherapy was being done by an insulin syringe and the syringe accidently pricked on the fingertip of doc.the pt was hep c positive but she took treatment of it and according to her she does her tests every 3 months and her tests are negative right now.what are teh chances the doctor will get the hepatitis
"hepatitis C" AND "needlestick" AND "sustained virologic response" AND transmission
HCV Transmission Risk After This Needlestick: Breakdown
The Key Factor: The Patient's HCV Status
- Completed treatment for Hepatitis C
- Tests every 3 months
- Is currently HCV RNA negative
Risk Calculation
Scenario A: Patient is genuinely cured (SVR, HCV RNA negative)
Scenario B: Patient's test results are accurate but you are uncertain
- Average: 1.8% per injury (range 0% to 7%)
- This is already quite low compared to HBV (~30%) or even HIV (~0.3%)
Factors that would increase risk (none of which apply here ideally):
| Risk Factor | Present Here? |
|---|---|
| Deep injury (hollow-bore needle, large gauge) | Insulin syringe = small gauge, low-volume - lower risk |
| Visible blood on needle | Unknown, but mesotherapy uses small volumes |
| High viral titer in source patient | No - patient is HCV RNA negative |
| Source patient with advanced liver disease | Not indicated here |
What Should the Doctor Do Right Now?
Immediate (within minutes):
- Wash the wound with soap and water for at least 15 minutes
- Do NOT squeeze or suck the wound
Within 24-48 hours - Report and test:
- Report to occupational health (mandatory in most institutions)
- Test the source patient - confirm anti-HCV and ideally HCV RNA (don't just take her word for it - get documented lab results)
- Baseline blood work on the doctor: anti-HCV antibody + ALT/AST today
Follow-up testing for the doctor:
- Repeat anti-HCV + ALT at 4-6 months post-exposure
- If desired (for earlier detection): HCV RNA at 4-6 weeks post-exposure (RNA becomes detectable before antibodies)
- All positive anti-HCV results must be confirmed with nucleic acid testing (HCV RNA)
Post-Exposure Prophylaxis (PEP):
- No PEP exists for HCV - unlike HIV, there is no recommended post-exposure antiviral prophylaxis for HCV
- Immunoglobulin is also not recommended (no evidence of efficacy)
- If infection is documented later, treat immediately with highly effective direct-acting antivirals (DAAs) - cure rates >95%
Bottom Line
| Question | Answer |
|---|---|
| Will the doctor get Hepatitis C? | Almost certainly NO |
| Why? | Patient has undetectable HCV RNA (SVR = cured) |
| Baseline risk even if viremic? | Only ~1.8% average |
| What to do now? | Wash wound, report to occupational health, document source patient's labs, get baseline and follow-up testing |
| Any preventive drug to take? | No - no PEP for HCV exists |
| If somehow infected? | DAA therapy cures >95% of HCV cases |
- Yamada's Textbook of Gastroenterology, 7th ed., p. 1908
The mesotherapy was done on face
Does "Face Mesotherapy" Change the Risk?
What actually determines HCV transmission risk:
| Factor | In This Case |
|---|---|
| Viral load in source patient's blood | Undetectable (SVR) - this is the dominant factor |
| Type of needle | Insulin syringe = fine gauge (30G or 31G), small dead space, low blood volume retained - actually lower risk than large hollow-bore needles |
| Depth of injury | Fingertip prick from a small insulin needle = superficial |
| Volume of blood inoculated | Very small with a fine insulin needle |
| Site on patient where needle was used | Does NOT affect HCV content of the blood on the needle |
What Face Mesotherapy Does Tell Us (Practically)
- Facial mesotherapy typically uses 30G or 31G insulin syringes with very short needles (4-6 mm)
- These are intradermal/subcutaneous injections - very superficial
- The blood volume retained in the needle dead space is minimal (insulin syringes are designed as low dead-space devices)
- The fingertip prick from such a needle carries less inoculum than a phlebotomy needle or IV cannula would
Reassurance Summary
Risk to the doctor = effectively zero, because the patient is cured of HCV (SVR, RNA negative). The needle gauge, injection site, and small blood volume all further reduce any residual theoretical concern.
- Wash the wound with soap and water
- Report to occupational health
- Get the source patient's HCV RNA documented from an actual lab result (not just verbal history)
- Get baseline anti-HCV + ALT, and repeat at 4-6 months
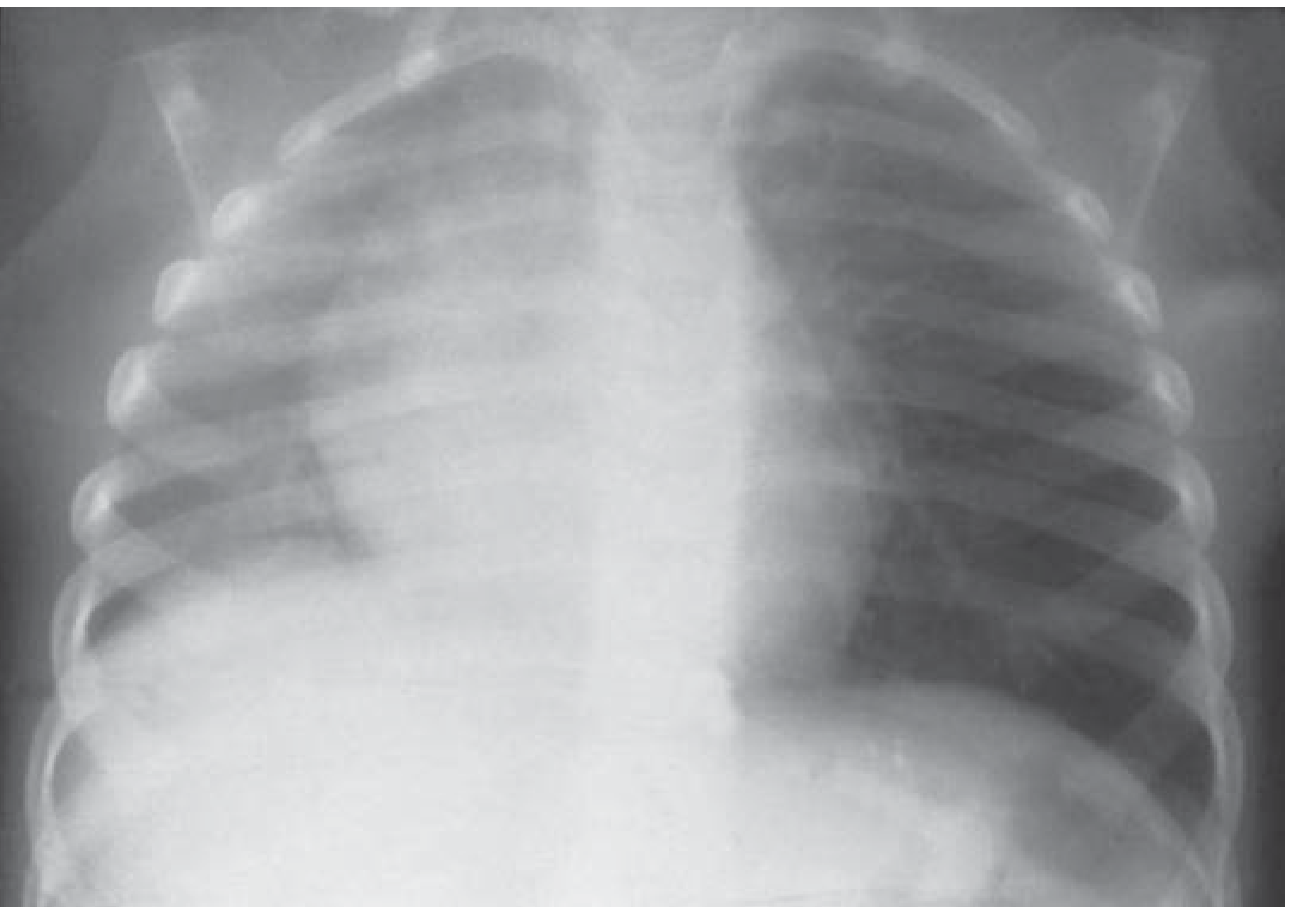
Teach me this. 4 yr asthmatic came to ed, after sob not resolved by bronchodilator and her right-side air entry was reduced had ronchi. Ask what inv to do? 1. CX-ray – can it be foreign body 2. ABG FBA causes either: • Complete obstruction: collapse (atelectasis) of distal lung tissue due to absorbed air 1. • Partial obstruction: "ball-valve" mechanism with air trapping and hyperinflation distal to the blockage 1. Most foreign bodies lodge in the right main bronchus because of its steeper vertical course 1. Clinical features Presentation depends on obstruction completeness and duration since aspiration 1: • Complete: silent cough, paradoxical chest/abdominal movement, cyanosis, loss of consciousness. • Partial: choking, coughing, wheeze (location-specific: inspiratory for laryngeal, expiratory for bronchial obstruction), or diminished breath sounds. • Chronic retention: persistent/recurrent cough, purulent sputum, wheeze unresponsive to bronchodilators, or fever Diagnostic approach Imaging and endoscopy are chosen according to suspected site and stability 1. Diagnostic hallmarks include focal hyperinflation or atelectasis; however, some cases show normal radiographs. Suspicion First-line test Upper airway FB Lateral neck x- ray Key findings Radiopaque FB, prevertebral soft tissue widening Next test if inconclusive Laryngoscopy © AMC4IMGs. All rights reserved. Unauthorised use, recording, reproduction, or distribution of content is strictly prohibited under international copyright law. 8 Suspicion First-line test Key findings Lower airway FB Chest x- ray (PA, lateral, expiratory or decubitus) Hyperinflation, mediastinal shift, atelectasis, pneumonia 1 Next test if inconclusive CT chest (≈100% sensitivity) or bronchoscopy Imaging overview Bronchoscopy—flexible or rigid—is the gold standard for both diagnosis and therapy, allowing visualization of granulation tissue or lodged objects 1. Management Management prioritizes airway clearance, oxygenation, and definitive removal 1. Emergency steps • Unresponsive patients: start CPR; attempt laryngoscopy-guided retrieval. If unsuccessful, proceed to emergency surgical airway (cricothyroidotomy or tracheotomy depending on age) 1. • Responsive with complete obstruction: sequential back blows followed by abdominal thrusts (children ≥1 year/adults) or chest thrusts (infants) until expelled or unresponsiveness occurs 1. • Partial obstruction: encourage coughing and provide oxygen support; monitor closely 1. These maneuvers correspond to AHA/AAP 2025 pediatric BLS guidance recommending alternating 5 back blows and 5 thrusts for severe pediatric FBAO 2. Planned removal • Upper airway: laryngoscopic extraction, with local or general anesthesia depending on cooperation. Avoid positive-pressure ventilation to prevent distal displacement of the FB 1. • Lower airway: bronchoscopy for extraction (choice of flexible vs rigid depends on patient age and stability). Rigid bronchoscopy is preferred in children or respiratory distress; flexible bronchoscopy in stable adults 1. • Surgery (thoracotomy/bronchotomy/resection): indicated when bronchoscopic removal fails or delayed obstruction leads to irreversible lung injury (e.g., bronchiectasis) 1. © AMC4IMGs. All rights reserved. Unauthorised use, recording, reproduction, or distribution of content is strictly prohibited under international copyright law. 9 Adjunctive management • Corticosteroids may reduce inflammation and facilitate removal when granulation tissue is present (off-label) 1. • Post-removal care: antibiotics for secondary pneumonia and evaluation for underlying swallowing dysfunction in adults 1. Complications Delayed or incomplete removal may lead to atelectasis, postobstructive pneumonia, lung abscess, or—if complete obstruction persists—hypoxic injury or death
Foreign Body Aspiration Masquerading as Asthma - Full Teaching Case
The Clinical Trap in This Case
Step 1: Reframe the Diagnosis
| Feature | Asthma Exacerbation | Foreign Body Aspiration |
|---|---|---|
| Wheeze | Bilateral, diffuse | Unilateral (bronchial FB) |
| Air entry | Reduced bilaterally | Asymmetric reduction |
| Response to bronchodilator | Improves | Does NOT improve |
| Age | Any | Peak 1-3 years, but up to school age |
| History | Triggers (URTI, allergen) | Often choking episode (may be unwitnessed) |
| CXR | Hyperinflation bilaterally | Unilateral hyperinflation or atelectasis |
This child has three features pointing away from simple asthma: age 4, unilateral findings, and bronchodilator failure.
Why the Right Side?
- It is wider in diameter
- It has a steeper, more vertical course from the trachea (more in line with the tracheal axis)
- The carina is slightly to the left, directing objects rightward
The Two Investigations to Order
1. Chest X-Ray (CXR) - PA + Lateral + Expiratory/Decubitus Views
A normal CXR does NOT rule out FBA.
- Plain films are normal in >25% of bronchial FBs
- >75% of FBs in children <3 years are radiolucent (organic material: peanuts, seeds, carrots)
- The absence of a radiopaque object means nothing
| CXR Finding | Mechanism | What it Means |
|---|---|---|
| Unilateral hyperinflation / obstructive emphysema | Ball-valve: air enters on inspiration, trapped on expiration | Partial bronchial obstruction (most common) |
| Mediastinal shift to LEFT | Right lung overinflated, pushes mediastinum away | Partial obstruction right bronchus |
| Atelectasis / collapse of right lung | Complete obstruction, absorbed air | Complete obstruction |
| Consolidation / pneumonia | Post-obstructive infection | Delayed/chronic presentation |
| Radiopaque foreign body | Dense object (coin, metal) | Directly visible |
- On inspiration, both lungs expand - may look normal
- On expiration, the obstructed lung cannot deflate - remains hyperinflated while the normal lung deflates
- The mediastinum shifts AWAY from the obstructed side on expiration
- In a normal lung, the dependent lung compresses (deflates) when the child lies on that side
- With an FB causing air trapping, the affected lung stays hyperinflated regardless of position
- However: bilateral decubitus films increase false positives without increasing true positives - use judiciously
2. Arterial Blood Gas (ABG)
| ABG Pattern | Interpretation | Action |
|---|---|---|
| Low PaCO2 (<35) + Low PaO2 | Early respiratory distress - compensated, hyperventilating | Watch closely, continue management |
| Normal or HIGH PaCO2 (≥40) + hypoxia + retractions | Impending respiratory failure - child is tiring, can no longer compensate | Escalate urgently - PICU |
| High PaCO2 + child suddenly "calms down" | Hypercarbia, exhaustion, altered mental status - NOT improvement | Immediate intervention |
The "calm child" trap: A child in severe respiratory distress who suddenly becomes quiet is NOT getting better - they may be developing CO2 narcosis. An ABG here is life-saving.
The Two Obstruction Patterns (Expanded)
FOREIGN BODY IN RIGHT BRONCHUS
|
─────┴─────
| |
PARTIAL COMPLETE
OBSTRUCTION OBSTRUCTION
| |
Ball-valve Absorbed air
mechanism distal to FB
| |
AIR TRAPPING ATELECTASIS
HYPERINFLATION COLLAPSE
| |
Right lung Right lung
BIGGER than SMALLER than
left on CXR left on CXR
Mediastinum Mediastinum
shifts LEFT shifts RIGHT
The Diagnostic Pathway
Unilateral wheeze / reduced air entry not responding to bronchodilator
↓
SUSPECT FBA
↓
Is child stable? ────────── NO → Emergency airway maneuvers
| (BLS, laryngoscopy, intubate)
YES
↓
CXR (PA + lateral)
+ Expiratory film
↓
┌───────────┴──────────────┐
Abnormal Normal
(hyperinflation, (but high clinical
atelectasis, FB) suspicion remains)
↓ ↓
CT CHEST FLEXIBLE BRONCHOSCOPY
(~100% sensitivity) (diagnostic + therapeutic)
↓
If confirmed → RIGID BRONCHOSCOPY for removal
Management Decision Tree
Immediate (if child is in distress):
- Oxygen - high flow
- DO NOT give more bronchodilators (will not help; may waste time)
- DO NOT attempt sedation or RSI if maintaining airway - partial obstruction becomes complete with loss of tone
If responsive with partial obstruction (this child's likely scenario):
- Encourage coughing
- Supplemental oxygen
- Do NOT do back blows/Heimlich - these are for acute complete obstruction
- Arrange urgent bronchoscopy
Definitive removal:
| Patient | Preferred Approach |
|---|---|
| Child in distress | Rigid bronchoscopy under general anesthesia - gold standard in pediatrics |
| Stable adult | Flexible bronchoscopy |
| FB cannot be removed bronchoscopically | Thoracotomy / bronchotomy / surgical resection |
- Allows simultaneous ventilation through the scope
- Better control and suction
- Can remove large objects that flexible scope cannot grasp
- Preferred in any age <12 years or with respiratory compromise
Adjuncts and Post-Removal Care
- Corticosteroids: reduce edema and granulation tissue around the FB (especially in delayed presentations) - facilitates removal
- Antibiotics: post-obstructive pneumonia is common, especially if FB was present for days
- Evaluate for recurrence: if FB was in right bronchus and not recovered, it can be coughed up and cause sudden upper airway obstruction later
Complications of Missed/Delayed FBA
| Timeframe | Complication |
|---|---|
| Hours | Atelectasis, post-obstructive pneumonia |
| Days-weeks | Lung abscess, empyema |
| Months | Bronchiectasis, irreversible lung damage |
| Any time | Hypoxic injury, death (if complete obstruction unrecognized) |
This is why FBA must be on your differential in ANY child with unilateral wheeze or bronchodilator-unresponsive wheeze - even if they carry a diagnosis of asthma. The two can coexist.
Summary: Key Teaching Points
- Unilateral findings = think FBA, not asthma, even in a known asthmatic
- Right bronchus is involved more often due to its steeper vertical course
- CXR is the first-line investigation - look for indirect signs (hyperinflation, atelectasis, mediastinal shift); a normal CXR does NOT exclude FBA
- Expiratory film is the most helpful CXR view - reveals air trapping on the obstructed side
- ABG is indicated here because bronchodilators failed - you must assess ventilatory status and exclude impending respiratory failure
- A "normalizing" PaCO2 in a tachypneic distressed child is a danger sign
- Bronchoscopy is gold standard - both diagnostic and therapeutic; use rigid scope in children
- Do not paralyze a child maintaining their airway - you may convert partial to complete obstruction
- Rosen's Emergency Medicine, p. 3175
- Tintinalli's Emergency Medicine, p. 836
Teach me. confirmed in a pt with CKD, (long stem) asking next appropriate investigation? 1. D dimer 2. VQ © AMC4IMGs. All rights reserved. Unauthorised use, recording, reproduction, or distribution of content is strictly prohibited under international copyright law. 10 Need to see the complete question as may need to start Mx This system guides management using hemodynamic parameters and markers of RV dysfunction. • Nonmassive PE o Stable blood pressure (SBP > 90 mm Hg) o No RV dysfunction o Normal cardiac biomarkers • Submassive PE o Stable blood pressure (SBP > 90 mm Hg) PLUS ≥ 1 of the following: § RV dysfunction § Evidence of myocardial necrosis (elevated troponin) • Massive PE: hemodynamic instability (due to right heart failure) o Systolic BP < 90 mm Hg for > 15 minutes o Acute decrease in systolic BP ≥ 40 mm Hg o Hemodynamic support is needed. Initial anticoagulation (first 5–10 days) The selection of the initial anticoagulant depends on the severity of the PE, patient comorbidities, and/or planned concurrent treatment. [48] • LMWH (e.g., enoxaparin DOSAGE) or fondaparinux DOSAGE [64][70] © AMC4IMGs. All rights reserved. Unauthorised use, recording, reproduction, or distribution of content is strictly prohibited under international copyright law. 11 o Preferred over UFH in most patients with normal renal function [22] o Anticoagulant of choice for PE in pregnant patients [22] o LMWH is recommended over UFH for patients with cancer. [71] • UFH o Preferred in patients with renal failure o Preferred if thrombolysis, embolectomy, or mechanical circulatory support are planned o Preferred in patients with unpredictable subcutaneous absorption (e.g., patients with obesity, hypoperfusion) • Initial oral anticoagulation o Consider as initial therapy for low-risk PE. o Agents: rivaroxaban or apixaban Long-term anticoagulation (up to 3 months) • Direct oral anticoagulant (DOAC) o Preferred over vitamin K antagonist (VKA) for most patients o No initial parenteral anticoagulation is required with rivaroxaban DOSAGE or apixaban DOSAGE o Initial parenteral anticoagulation is required with dabigatran DOSAGE or edoxaban DOSAGE • VKA: warfarin o Therapeutic target: INR 2–3 [64] o Preferred over LMWH when a DOAC cannot be used • Long-term parenteral anticoagulation with LMWH o Preferred over VKA in patients with cancer if a DOAC cannot be used [71] o Preferred in pregnant patients [62] Extended anticoagulation (> 3 months) • Reassess the need for anticoagulation after 3 months, then annually. • Indications for extended anticoagulation o Unprovoked PE with a low to moderate risk of bleeding o Provoked PE secondary to a chronic risk factor with a low to moderate risk of bleeding o Patients with active cancer with any level of bleeding risk [71]
PE Confirmed in CKD - Next Appropriate Investigation: VQ Scan vs D-Dimer
First: Read the Question Carefully
Part 1: Why the Answer is VQ Scan (Not D-Dimer)
Why D-Dimer is Wrong Here
- Renal failure causes impaired fibrinolysis
- Inflammatory state of CKD raises D-Dimer
- CKD patients often have comorbidities (infection, malignancy, immobility) that all elevate D-Dimer independently
A positive D-Dimer in CKD is essentially meaningless. A negative D-Dimer is the only useful result - but again, PE is already confirmed, so this is a moot point.
| D-Dimer Result | Utility |
|---|---|
| Negative | Rules OUT PE (high sensitivity) |
| Positive | Non-specific - means nothing definitive |
| In CKD | Almost always falsely elevated - useless as a screening tool |
Why VQ Scan is the Answer
PE is confirmed clinically/by initial workup, but CTPA (CT Pulmonary Angiography) cannot be used because the patient has CKD.
- Acute contrast-induced nephropathy (CIN)
- Accelerating progression to end-stage renal disease
- In advanced CKD (GFR <30), this is a significant risk
- Uses radiolabelled tracers (technetium-99m) - NOT nephrotoxic
- No contrast agent required
- Safe in renal failure
- Can confirm/characterize PE without harming kidneys
The Full Diagnostic Logic for PE (So You Understand Where VQ Fits)
Suspected PE
↓
Wells Score / Clinical Probability
↓
┌─────────────────────────────┐
LOW/INTERMEDIATE HIGH
PROBABILITY PROBABILITY
↓ ↓
D-DIMER Image DIRECTLY
(if negative → PE excluded)
(if positive → Image)
↓
┌──────────────────────────────────────────┐
| IMAGING OPTIONS |
├──────────────────────────────────────────┤
| Normal renal function → CTPA (1st line) |
| CKD / contrast allergy → VQ SCAN |
| Pregnancy → VQ SCAN (normal CXR) or |
| CTPA (abnormal CXR) |
| Inconclusive → Pulmonary angiography |
| (gold standard, invasive) |
└──────────────────────────────────────────┘
CTPA vs VQ Scan - Head to Head
| Feature | CTPA | VQ Scan |
|---|---|---|
| Sensitivity | Very high (>95%) | ~80-90% (high prob scan) |
| Specificity | High | Moderate (intermediate scans common) |
| First-line for PE? | YES (most patients) | Second-line (specific indications) |
| Contrast required? | YES - iodinated contrast | NO |
| Safe in CKD? | NO (contrast nephrotoxicity) | YES |
| Safe in pregnancy? | Avoid if possible (fetal radiation/contrast) | Preferred (lower fetal dose) |
| Also shows alternative diagnoses? | YES (17-19% of cases) | NO |
| Interpretation affected by lung disease? | Less so | YES - COPD, pneumonia reduce accuracy |
| Availability | Widely available, fast | Requires nuclear medicine |
VQ Scan - How It Works and How to Read It
- Ventilation (V): Patient inhales radioactive gas (e.g., Xenon-133 or Tc-99m DTPA aerosol) - shows where air goes
- Perfusion (Q): IV injection of Tc-99m MAA particles - shows where blood goes
PIOPED Criteria for Interpretation:
| Result | PE Probability | Action |
|---|---|---|
| Normal | <2% | PE excluded |
| Low probability | ~4% | Safe to withhold treatment if low clinical probability |
| Intermediate (indeterminate) | ~30% | Further imaging needed |
| High probability (≥2 segmental mismatches) | ~87% | PE confirmed - treat |
Important: In patients with underlying lung disease (COPD, pneumonia), VQ scans are more often intermediate/indeterminate - reducing their usefulness. This is when CTPA (if kidneys allow) or pulmonary angiography is needed.
Part 2: Management in CKD - The Critical Changes
The Central Problem with CKD and Anticoagulation
Initial Anticoagulation (First 5-10 days)
| Drug | CKD Consideration | Verdict |
|---|---|---|
| LMWH (enoxaparin) | Renally cleared - accumulates in CKD, high bleeding risk; needs anti-Xa monitoring | Avoid or use with caution in severe CKD (GFR <30) |
| Fondaparinux | Contraindicated if GFR <30 | Avoid in severe CKD |
| UFH (Unfractionated Heparin) | Hepatically cleared, NOT renally dependent; easily reversible with protamine | PREFERRED in renal failure |
| Rivaroxaban / Apixaban (oral) | Both are partially renally cleared; avoid if GFR <15-25 | Caution in moderate-severe CKD |
Key teaching point: UFH is the anticoagulant of choice for initial treatment of PE in CKD/renal failure. It is also preferred if thrombolysis or embolectomy is being planned (easy reversal).
Long-Term Anticoagulation (Up to 3 months and beyond)
| Drug | CKD Consideration |
|---|---|
| DOACs (rivaroxaban, apixaban, dabigatran, edoxaban) | All partially renally cleared; dose adjustment or avoidance in GFR <25-30; dabigatran highly renally cleared - avoid in CKD |
| Warfarin (VKA) | NOT renally cleared - actually becomes the preferred long-term option in advanced CKD (GFR <25-30) or dialysis when DOACs are contraindicated; target INR 2-3 |
| LMWH | Preferred in cancer patients or pregnancy but requires anti-Xa monitoring in CKD |
- Mild-moderate CKD (GFR 30-60): DOACs with caution; avoid dabigatran
- Severe CKD (GFR <30): UFH acutely → transition to warfarin for long-term
- Dialysis: Warfarin (though evidence is limited and controversial; some guidelines now suggest no anticoagulation for provoked PE in dialysis patients due to bleeding risk)
Severity Stratification - Why It Matters for Management
CONFIRMED PE
↓
Check hemodynamics + RV function + troponin
↓
┌─────────────────────────────────────────────────┐
│ MASSIVE PE (SBP <90 or drop ≥40 mmHg >15 min) │
│ → UFH immediately │
│ → Thrombolysis (if no contraindication) │
│ [CKD is NOT a contraindication to tPA] │
│ → Surgical/catheter embolectomy if thrombolysis │
│ fails or is contraindicated │
├─────────────────────────────────────────────────┤
│ SUBMASSIVE PE (stable BP + RV dysfunction │
│ or elevated troponin) │
│ → UFH (preferred in CKD) │
│ → Consider thrombolysis if deteriorating │
│ → Monitor closely │
├─────────────────────────────────────────────────┤
│ NONMASSIVE PE (stable, no RV dysfunction) │
│ → Anticoagulation alone │
│ → UFH initially in CKD │
│ → Transition to warfarin long-term in severe CKD│
└─────────────────────────────────────────────────┘
Summary: The Entire Concept on One Page
| Question | Answer in CKD |
|---|---|
| Next investigation after confirmed PE with CKD? | VQ scan (CTPA contraindicated due to contrast nephrotoxicity) |
| Why not D-Dimer? | PE already confirmed; D-Dimer is chronically elevated in CKD (false positives); it is a screening tool only |
| Initial anticoagulant of choice? | UFH (not renally cleared; easily reversible) |
| Why not LMWH? | Accumulates in CKD; anti-Xa monitoring needed; avoid if GFR <30 |
| Why not DOACs initially? | Partially renally cleared; most require GFR >25-30 |
| Long-term anticoagulation in severe CKD? | Warfarin (INR 2-3) when DOACs contraindicated |
| Massive PE in CKD - treat differently? | No - thrombolysis still indicated; CKD is not a contraindication to tPA |
- Grainger & Allison's Diagnostic Radiology
- Fishman's Pulmonary Diseases and Disorders
- Murray & Nadel's Textbook of Respiratory Medicine
Teach me this the topic as well.
Teach me this the topic as well.Q. Pt with cough hand small muscle wasting invest Pancoast tumour 1. Xray 2. 3. NCS – will not find the cause Ct – we need to see lower branchial plexus Best is MRI
Pancoast Tumour (Superior Sulcus Tumour) - Complete Teaching
The Clinical Scenario Decoded
Anatomy First - Why Pancoast Tumour Does What It Does
APEX OF LUNG (Superior Sulcus)
↓
Tumour grows upward and outward
↓
Invades adjacent structures:
┌──────────────────────────────────────────────────────┐
│ Structure Invaded → Clinical Feature │
├──────────────────────────────────────────────────────┤
│ Lower brachial plexus → Arm/hand pain + wasting │
│ (C8, T1, T2 roots) → Ulnar distribution pain │
│ → Small muscle atrophy │
├──────────────────────────────────────────────────────┤
│ Paravertebral sympathetic → Horner's syndrome │
│ chain + stellate ganglion │ (Ptosis, Miosis, │
│ │ Anhidrosis, Enophthalmos)│
├──────────────────────────────────────────────────────┤
│ Parietal pleura + ribs → Shoulder/chest wall pain │
│ (1st, 2nd, 3rd ribs) │ │
├──────────────────────────────────────────────────────┤
│ Subclavian vessels → Vascular compromise │
├──────────────────────────────────────────────────────┤
│ Vertebral bodies → Spinal cord compression │
│ (late) → Paraplegia (rare) │
└──────────────────────────────────────────────────────┘
Pancoast Syndrome - The Full Picture
- Shoulder and arm pain - along C8/T1/T2 distribution - often radiates to axilla and down the ulnar border of arm (ring and little fingers)
- Weakness and atrophy of intrinsic hand muscles - ulnar nerve distribution (most hand intrinsics = C8/T1)
- Horner's syndrome - ipsilateral ptosis, miosis, anhidrosis (±enophthalmos)
Important: Pancoast syndrome is present in only ~1/3 of patients with superior sulcus tumours. The rest may have the tumour without all three components.
- Cough (pulmonary primary)
- Small muscle wasting (lower brachial plexus T1 involvement)
What Type of Tumour is a Pancoast Tumour?
- Mostly NSCLC (non-small cell lung cancer) - squamous cell or adenocarcinoma
- Rarely SCLC, carcinoid, or metastatic disease
- Occasionally non-malignant (infections, lymphoma, mesothelioma)
- Defined by location (superior sulcus), not histology
- Chest wall involvement must be at or above the first rib - below the 2nd rib it is NOT a Pancoast tumour
The Investigation Question - X-Ray vs NCS vs CT vs MRI
Investigation 1: Chest X-Ray
- Apical opacity / soft tissue mass at lung apex
- Rib destruction (1st, 2nd ribs - pathognomonic)
- Pleural thickening at apex
- Atelectasis or consolidation if bronchus is involved
- Asymmetry of apical soft tissues
- The lung apex is a blind spot on standard PA CXR - overlying clavicle, ribs and soft tissues obscure it
- A normal CXR does NOT rule out Pancoast tumour
- Some tumours are only identified on CT
If clinical suspicion is high but CXR is negative or equivocal → go straight to CT / MRI.
Investigation 2: NCS (Nerve Conduction Study) - Why It Does NOT Find the Cause
- Electrical conduction along peripheral nerves
- Can confirm that the ulnar nerve (or other nerves) is NOT conducting normally
- Can localise the site of a nerve lesion to a general region (e.g., "proximal" vs "distal")
- NCS evaluates the nerve distal to the point of compression
- In Pancoast, the damage is at the nerve ROOT level (C8/T1) - the most proximal part of the brachial plexus, essentially where the root exits the spinal cord / enters the plexus
- NCS cannot image the root compression; it can only show downstream effects
- More importantly: NCS tells you THAT there is nerve damage but NOT WHY or WHERE the compressing lesion is
- It cannot see a tumour, cannot see bony destruction, cannot see pleural invasion
- Confirms neurogenic pattern (denervation, reduced motor unit potentials)
- Helps differentiate from cervical spondylosis, carpal tunnel, or peripheral neuropathy
- Localises to lower trunk brachial plexus (C8/T1) level
- Useful to EXCLUDE other causes of hand wasting (e.g., MND, ulnar neuropathy at elbow)
NCS is supportive - it tells you the nerve is damaged. It does NOT show you the tumour causing it. You still need imaging.
Investigation 3: CT Chest
- The tumour mass at the apex
- Rib destruction (1st, 2nd ribs)
- Extent of chest wall invasion
- Mediastinal lymph node involvement
- Other pulmonary nodules (metastases/synchronous primaries)
- Pleural involvement
- CT is excellent for parenchymal and bony structures
- CT is inferior for soft tissue planes - especially:
- Brachial plexus invasion (nerves are not well-seen on CT)
- Subclavian vessel involvement
- Extent of plexus involvement (which roots? how far?)
- Subpleural fat plane involvement
- Spinal cord / foraminal extension
CT cannot tell you reliably if the brachial plexus is invaded or how far - and this is critical for surgical planning.
Investigation 4: MRI - The Best Investigation
"MRI of the chest is considered to be superior for evaluating patients with superior sulcus tumors because of better assessment of invasion through the pleura and subpleural fat, better evaluation of plexus involvement, and better definition of subclavian vessel involvement."
| Feature | CT | MRI |
|---|---|---|
| Brachial plexus visualisation | Poor | Excellent |
| Subclavian vessel invasion | Moderate (with contrast) | Excellent |
| Subpleural fat plane | Moderate | Excellent |
| Spinal canal / cord | Poor | Excellent |
| Foraminal extension | Moderate | Excellent |
| Chest wall soft tissue planes | Moderate | Excellent |
| Bony destruction | Excellent | Good |
| Lung parenchyma | Excellent | Moderate |
| Mediastinal nodes | Good | Good |
- T1: Tumour vs fat planes (fat = bright, tumour = dark = invasion if fat plane lost)
- T2: Oedema, fluid, nerve signal
- Coronal and sagittal planes: Critical - shows the relationship of tumour to brachial plexus roots from above
- MR Angiography: Best assessment of subclavian vessel invasion specifically
- Is the lower brachial plexus (C8, T1) invaded? - determines resectability
- Is the subclavian artery/vein involved? - determines if vascular resection is needed
- Is there foraminal or spinal cord extension? - determines if neurosurgical input needed
- Exactly which nerve roots are involved? - predicts post-operative functional deficits
The Diagnostic Pathway - Summarised
Cough + Small muscle wasting (hand) + Shoulder pain
↓
SUSPECT PANCOAST TUMOUR
↓
CHEST X-RAY (PA + Apical lordotic view)
↓
┌─────────────┴──────────────┐
Abnormal Normal but
(apical mass, high suspicion
rib destruction) ↓
↓ Still proceed
CT CHEST to CT/MRI
(confirms mass,
extent, nodes,
bony destruction)
↓
MRI CHEST (BEST)
(brachial plexus invasion,
subclavian vessels,
spinal canal,
subpleural fat planes)
↓
Tissue Diagnosis
┌──────────────────────────────┐
│ Bronchoscopy (~50% yield) │
│ CT-guided TTNA (>90% yield) │
│ EBUS-FNA for mediastinal LN │
└──────────────────────────────┘
↓
Staging + Mediastinoscopy
(exclude N2 disease before
surgery - if N2+, surgery
not beneficial)
Why the Sequence Matters for Exams
| Investigation | Role | Limitation |
|---|---|---|
| CXR | First - always | Misses many apical tumours; can be normal |
| NCS/EMG | Confirms nerve damage pattern | Does NOT show the cause - no tumour, no anatomy |
| CT | Shows tumour, bone, nodes | Cannot adequately assess brachial plexus |
| MRI | Best - shows plexus, vessels, soft tissue invasion | Less available, contraindicated with pacemakers |
| PET-CT | Staging, differentiates benign apical cap from tumour | Not first-line for local assessment |
| Bronchoscopy | Tissue diagnosis (~50% yield for apical) | Limited - peripheral tumour may not be bronchoscopically accessible |
| CT-guided TTNA | Tissue diagnosis (>90% yield) | Pneumothorax risk |
Management Overview
Resectable (T3N0M0 or T3N1M0, no vascular/spinal involvement):
- Induction chemoradiotherapy (cisplatin + etoposide + 45 Gy radiation) x 2 cycles
- Surgical resection - en bloc lobectomy + chest wall resection (ribs 1-3) + lower brachial plexus root ± stellate ganglion
- 5-year survival with complete resection: ~54%
Unresectable (T4: subclavian artery, vertebral body, spinal cord, or N2/N3 nodes):
- Definitive chemoradiotherapy
- Palliative intent
Poor prognostic factors:
- N2 nodal involvement
- Vertebral body or supraclavicular involvement
- Incomplete resection
- Weight loss
Summary Table
| Feature | Detail |
|---|---|
| Location | Apex of lung (superior sulcus), above 1st rib |
| Typical cancer type | NSCLC (squamous cell / adenocarcinoma) |
| Classic triad | Shoulder/arm pain + Hand wasting + Horner's |
| Nerve roots involved | C8, T1 (lower trunk brachial plexus) |
| Pain distribution | Ulnar border - ring and little fingers |
| Hand muscles wasted | Intrinsic hand muscles (interossei, thenar/hypothenar) |
| Best investigation | MRI - brachial plexus + subclavian vessels |
| Why not NCS? | Shows nerve damage but NOT the cause/tumour |
| Why not CT alone? | Cannot assess brachial plexus invasion |
| Treatment | Neoadjuvant chemoRT → surgery |
- Murray & Nadel's Textbook of Respiratory Medicine
- Schwartz's Principles of Surgery, 11th ed.
- Robbins & Kumar Basic Pathology
- Gray's Anatomy for Students
Female breast feeding for child, come to GP for suggestion of contraception, want to conceive in 12 months 1. 2. 3. 4. 5. Continue breastfeeding – 6 weeks (exclusive BF) COCP – can affect the BF POP – early return of fertility Depo – delayed return of fertility IUD – long term contraception
Contraception in a Breastfeeding Woman Who Wants to Conceive in 12 Months
The Clinical Problem - Two Competing Goals
- Contraception NOW - she is breastfeeding and does not want pregnancy immediately
- Fertility WITHIN 12 MONTHS - she wants to conceive again soon
- Is safe while breastfeeding (does not reduce milk supply or harm infant)
- Has a rapid return of fertility on stopping (within the 12-month window)
Understanding the Physiology First
Why is Breastfeeding Itself Contraceptive?
- Suppresses GnRH pulsatility
- Reduces FSH and LH
- Prevents follicular development and ovulation
- Causes lactational amenorrhoea
LAM - The Breastfeeding-as-Contraception Rule
| Criterion | Requirement |
|---|---|
| 1. Amenorrhoea | No return of periods since delivery |
| 2. Fully/exclusively breastfeeding | Day AND night feeds, no supplementary formula or solids |
| 3. Baby < 6 months old | Efficacy drops sharply after 6 months |
Your notes say "6 weeks" - this needs clarification. LAM is effective for up to 6 MONTHS (not 6 weeks) if all three criteria are met. The 6-week figure refers to the postnatal review appointment, not the duration of LAM protection.
- Any supplementary feeds (formula, solids introduced)
- Baby sleeping through the night (long gaps between feeds reduce prolactin)
- Return of menstruation
- Baby > 6 months
Analysing Each Option Against the Two Goals
Option 1: Continue Breastfeeding (LAM)
Return of fertility: ✅ Immediate on stopping
Answer for this patient: ✅ Appropriate for NOW (while exclusively breastfeeding, amenorrhoeic, baby <6 months)
- Only reliable up to 6 months postpartum
- Requires strict exclusive breastfeeding
- Once she introduces solids or supplements, or gets her period back → LAM fails → needs backup method
- Not suitable as her only method if she is already beyond 6 months postpartum or not exclusively breastfeeding
Option 2: COCP (Combined Oral Contraceptive Pill)
Return of fertility: ✅ Rapid (within 1-3 months of stopping)
- Reduced milk volume and quality - oestrogen suppresses prolactin-stimulated milk production
- Oestrogen passes into breast milk - potential hormonal exposure to infant
- Increased VTE risk in the postpartum period - oestrogen is thrombogenic, and postpartum is already a high-VTE state
- COCP in breastfeeding < 6 weeks postpartum = Category 4 (absolutely contraindicated)
- COCP in breastfeeding 6 weeks to 6 months = Category 3 (risks usually outweigh benefits)
- COCP in breastfeeding > 6 months = Category 2 (benefits usually outweigh risks, milk supply more established)
For this patient: COCP should NOT be used while she is still breastfeeding, regardless of timing.
Option 3: POP (Progestogen-Only Pill / Mini-Pill)
Return of fertility: ✅ Rapid return (within days to weeks of stopping)
Answer for this patient: ✅ This is the correct answer
- No oestrogen - does not suppress prolactin, does not reduce milk supply
- Small amounts of progestogen pass into breast milk but are not harmful to infant
- Highly effective (~99% with perfect use)
- WHO MEC Category 1 (no restriction) from 6 weeks postpartum onward in breastfeeding women
- Primary mechanism: Thickens cervical mucus (prevents sperm penetration)
- Secondary: Suppresses ovulation (in ~50% of cycles with traditional POP; ~97% with desogestrel-containing POP like Cerazette)
- Thins endometrium
| Type | Ovulation suppression | Window for taking |
|---|---|---|
| Traditional (norethisterone, levonorgestrel) | ~50% of cycles | Must take within 3-hour window daily |
| Desogestrel POP (Cerazette/Cerelle) | ~97% of cycles | 12-hour window - more forgiving |
- Fertility returns within days to weeks of stopping
- No cumulative effect on future fertility
- Ideal for someone wanting to conceive in 12 months
- Irregular bleeding / spotting (most common reason for discontinuation)
- Possible amenorrhoea
- Headaches, mood changes, breast tenderness
Option 4: Depo-Provera (DMPA - Depot Medroxyprogesterone Acetate)
Return of fertility: ❌ SIGNIFICANTLY DELAYED - WRONG for this patient
Answer for this patient: ❌ Not appropriate
- DMPA is a 3-monthly injection of long-acting progestogen
- After stopping, fertility return is unpredictable and often significantly delayed
- Median time to conception after last injection: 10 months
- Range: 4 months to 2+ years
- Some women do not ovulate for up to 18-24 months after their last injection
- This is irreversible once the injection is given
Teaching point: Depo is excellent for women who want long-term contraception without daily compliance. But if any desire for pregnancy in the near future exists (within 18-24 months), Depo should be avoided.
- Reduced bone mineral density with long-term use (DEXA monitoring if >2 years)
- Irregular bleeding initially, then amenorrhoea
- Cannot be reversed once injected
Option 5: IUD (Intrauterine Device)
Return of fertility: ✅ Immediate on removal
Answer for this patient: ⚠️ Not ideal - designed for long-term use
| Type | Duration | Mechanism | Effect on periods |
|---|---|---|---|
| Copper IUD (non-hormonal) | 5-10 years | Copper is spermicidal; creates hostile uterine environment | May worsen periods |
| LNG-IUS (Mirena, Kyleena) | 3-8 years (device dependent) | Progestogen thickens mucus, thins endometrium, may suppress ovulation | Lighter or absent periods |
- Designed for long-term contraception - inserting and removing within 12 months is poor utilisation
- Insertion procedure - involves speculum exam and intrauterine placement; discomfort, small risk of expulsion/perforation
- Cost-effectiveness - not appropriate for <12-month use
- However: If the patient changes her mind or doesn't conceive, removal at any time is possible with immediate return of fertility
- Wants reliable long-term contraception (years)
- Does not plan further pregnancy for a defined long period
- Cannot take hormonal methods
- Postpartum insertion can be done at 4-6 weeks or immediately postpartum (within 48 hours)
The Answer - What to Recommend
| Method | Safe in BF? | Rapid fertility return? | Recommendation |
|---|---|---|---|
| LAM (continue BF) | ✅ | ✅ | ✅ Use NOW (if criteria met, baby <6 months) |
| COCP | ❌ | ✅ | ❌ Contraindicated in BF |
| POP | ✅ | ✅ | ✅ BEST CHOICE |
| Depo | ✅ | ❌ | ❌ Delayed fertility - inappropriate |
| IUD | ✅ | ✅ (on removal) | ⚠️ Not ideal for <12-month use |
Recommended Management:
- Continue exclusive breastfeeding → LAM provides ~98% protection
- Counsel: "The moment you introduce any formula, solids, or your period returns - you need to start contraception immediately"
- Start Progestogen-Only Pill (POP)
- Desogestrel POP (e.g., Cerazette) preferred for better efficacy and larger window
- Counsel on irregular bleeding
- When ready to conceive: simply stop the POP - fertility returns within days to weeks
Summary Concept Map
Breastfeeding woman + wants pregnancy in 12 months
↓
TWO KEY QUESTIONS:
① Safe in breastfeeding?
② Rapid return of fertility?
↓
COCP → ❌ (reduces milk supply, oestrogen)
DEPO → ❌ (delayed fertility up to 2 years)
IUD → ⚠️ (safe but for long-term use)
LAM → ✅ (if criteria strictly met, <6 months)
POP → ✅ BEST ANSWER
Safe in BF (no oestrogen)
Fertility returns in days-weeks on stopping
Oral, reversible, once-daily
Exam Pearl
The question tests whether you know:
- COCP is contraindicated in breastfeeding (due to oestrogen, not progestogen)
- Depo delays fertility and is wrong for someone wanting pregnancy within 12 months
- IUD is long-term and not the best fit for <12-month contraception
- POP is the correct answer - safe in breastfeeding AND has rapid fertility return
- LAM is valid but only while strict exclusive breastfeeding criteria are met (up to 6 months - not 6 weeks)