Anal fistula and treatment
Reading File
Finding Sources
Searching PubMed
"anal fistula" AND treatment
Searching Images
anal fistula types classification anatomy
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Here is a comprehensive overview of anal fistula and its treatment.
Anal Fistula
Definition & Epidemiology
An anal fistula is an abnormal tract connecting the internal opening at the dentate line (from an infected anal gland) to the perianal skin. It represents the chronic form of a perianal abscess — when the infected gland fails to heal after drainage, a persistent tract remains. Approximately 30–50% of perianal abscesses lead to fistula formation. The incidence is ~8.6 per 100,000, with men affected 2–3× more than women. — Goldman-Cecil Medicine
Pathogenesis (Cryptoglandular Theory)
Most fistulas arise from infection in the anal glands (cryptoglandular origin), located at the level of the dentate line. The gland becomes infected → forms an abscess → tracks through the sphincter → discharges onto perianal skin, leaving a persistent epithelialized tract.
Parks Classification
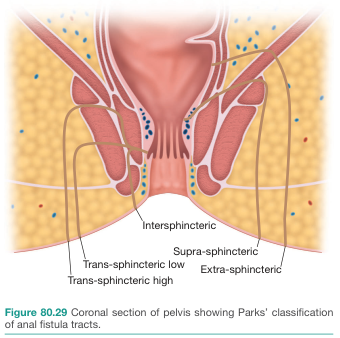
| Type | Description | Frequency |
|---|---|---|
| Intersphincteric | Tract in the intersphincteric space; external opening near anal verge | ~70% (most common) |
| Transsphincteric | Traverses both internal and external sphincters; classified as low (distal EAS) or high (proximal EAS) | ~20–25% |
| Suprasphincteric | Ascends above entire sphincter complex then descends through levator ani to ischioanal fossa | Uncommon |
| Extrasphincteric | Internal opening above dentate line (rectum), perforates levator ani; associated with Crohn disease, trauma, or pelvic abscess | Rare |
A horseshoe fistula has bilateral external openings with a single posterior midline internal opening. — Goldman-Cecil Medicine; Mulholland & Greenfield's Surgery
Clinical Features
- Recurrent perianal abscess at the same site (pathognomonic clue)
- Persistent intermittent purulent discharge from perianal skin
- External opening visible as erythematous nodule with granulation tissue
- Palpable fibrous tract coursing toward the anal canal
- The internal opening at the dentate line may or may not be visible on anoscopy
Differential diagnoses: hidradenitis suppurativa (superficial tracts, no anal canal connection), pilonidal disease (gluteal cleft, foreign body reaction to hair).
Evaluation
- History: duration, prior anorectal surgery, continence, bowel habits (screen for Crohn disease)
- Examination under anesthesia (EUA): probe passed along tract; assess sphincter involvement
- Goodsell's rule: Posterior external openings → internal opening in posterior midline; anterior external openings → nearest anal crypt
- Hydrogen peroxide injection ± endoanal ultrasound to identify smaller tracts
- MRI pelvis (modality of choice for complex fistulas): high signal on fat-suppressed T2W/STIR sequences; shows tracts, abscesses, supralevator extensions; reduces recurrence rates when used preoperatively
- Endoanal ultrasound: good for intraluminal/internal opening assessment
- Fistulography (water-soluble contrast): useful when anatomy is unclear
Treatment
Treatment of anal fistulae is fundamentally surgical. The key principle: eliminate the internal opening while preserving sphincter function (continence).
1. Fistulotomy (Lay-Open)
- Unroofing (laying open) of the fistula tract; heals by secondary intention
- Indicated for intersphincteric and low transsphincteric fistulas with normal continence
- Safe when < 30% of sphincter is involved
- Healing rates up to 90%
- ⚠ Caution: Anterior fistulotomy in women (short anterior sphincter; obstetric injury risk)
2. Seton Placement
- A suture or Silastic vessel loop threaded through the tract and secured
- Draining seton: keeps external opening patent, prevents abscess; allows maturation of the tract before definitive repair
- Cutting seton: tightened at 2–4 week intervals to gradually erode through muscle with fibrosis; success rates up to 94%, but incontinence risk 23–22%
- Often the first step for high or complex fistulas
3. Advancement Flap (Endoanal/Mucosal Advancement Flap)
- A flap of mucosa + internal sphincter is raised; tract is curetted; internal opening is sutured; flap advanced to cover it
- Used for complex fistulas where sphincter division is unsafe
- Success rate: 66–87%
- Failed flaps can be repeated after inflammation resolves
4. LIFT Procedure (Ligation of Intersphincteric Fistula Tract)
- After seton-induced fibrosis, incision in intersphincteric groove → tract identified → both ends ligated and divided
- Sphincter-sparing
- Success rates: 40–95% (wide range)
5. Fibrin Glue & Anal Fistula Plug
- Biological sealant injected into tract (fibrin glue) or bioabsorbable plug inserted
- High recurrence rates — not recommended as primary treatment
6. Newer/Emerging Techniques (Recent Evidence)
- TROPIS (transanal opening of intersphincteric space): recent meta-analysis (2025, PMID 40693967) supports its use for high complex fistulas
- Stem cell therapy (adipose-derived MSCs): 2025 meta-analysis (PMID 40205247) shows promising healing rates, especially in Crohn-associated fistulas
- Autologous platelet-rich plasma (PRP): 2024 meta-analysis (PMID 39127896) supports its efficacy as an adjunct
- Anal fistula clips (OTSC): 2025 meta-analysis (PMID 40929949) evaluating outcomes
Fistula in Crohn Disease
- Affects 13–54% of Crohn disease patients
- Asymptomatic fistulas: no treatment needed
- Complex multi-tract fistulas: unroof branching tracts first → achieve single tract
- Anti-TNF agents (e.g., infliximab): effective for symptomatic control and healing
- Once quiescent → standard surgical options applicable
- Severe cases: long-term seton + medical therapy; temporary diversion; proctectomy for refractory perianal disease
Summary Table: Surgical Options
| Procedure | Best For | Healing Rate | Continence Risk |
|---|---|---|---|
| Fistulotomy | Simple/low fistulas, <30% sphincter | ~90% | Low if <30% muscle |
| Cutting seton | High fistulas | ~94% | Moderate (~23%) |
| Advancement flap | Complex/high | 66–87% | Low |
| LIFT | Transsphincteric | 40–95% | Very low |
| Fibrin glue/plug | — | Poor | None |
| TROPIS | High complex | Emerging evidence | Low |
| Stem cells | Crohn-related | Promising | Minimal |
Sources: Mulholland and Greenfield's Surgery, 7e; Goldman-Cecil Medicine; Grainger & Allison's Diagnostic Radiology; Recent meta-analyses (PubMed 2024–2025).
This is a shared conversation. Sign in to Orris to start your own chat.