high altitude pulmonary oedema
Reading File
Finding Sources
Searching PubMed
"high altitude pulmonary edema" pathophysiology treatment
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have very comprehensive information. Let me compile the full response.
High-Altitude Pulmonary Oedema (HAPE)
HAPE is the most lethal form of altitude illness. It is a non-cardiogenic pulmonary oedema that develops within 2-4 days after rapid ascent to high altitude, and is a leading cause of death in mountaineers.
Definition and Context
HAPE occurs in the spectrum of altitude-related illness, which includes:
- Acute Mountain Sickness (AMS) - mild, benign neurological symptoms
- High-Altitude Cerebral Oedema (HACE) - severe neurological end of the spectrum
- High-Altitude Pulmonary Oedema (HAPE) - primarily a pulmonary disorder, not necessarily preceded by AMS
HAPE rarely develops beyond 4-5 days at the same altitude, likely due to pulmonary vascular remodeling and adaptation. It is rare below 3,600 m (12,000 ft).
- Harrison's Principles of Internal Medicine, 22nd Edition
- Park's Textbook of Preventive and Social Medicine
Risk Factors
| Risk Factor | Notes |
|---|---|
| Rapid rate of ascent | Most important modifiable factor |
| Prior history of HAPE | Strongest individual predictor |
| Male sex | Men more susceptible than women |
| Cold environmental temperatures | Exercise + cold increase pulmonary vascular pressure |
| Respiratory tract infections | Predispose even constitutionally resistant individuals |
| Mitral stenosis, primary pulmonary hypertension | Cardiopulmonary abnormalities causing baseline pulmonary HTN |
| Unilateral absence of pulmonary artery | |
| Patent foramen ovale | 4x more common in HAPE-susceptible individuals (causal link unproven) |
- Harrison's Principles of Internal Medicine, 22nd Edition
Pathophysiology
HAPE is fundamentally driven by hypoxia-induced exaggerated pulmonary vasoconstriction, with several interacting mechanisms:
1. Patchy Hypoxic Pulmonary Vasoconstriction
Severe hypoxia causes pulmonary arteriolar constriction, but this is uneven - some regions constrict more than others. Blood is redirected into fewer unconstricted vessels, causing markedly elevated capillary pressure (>18 mmHg) in those areas. This leads to capillary stress failure and fluid leakage into alveoli. The pulmonary artery wedge pressure remains normal (confirming non-cardiogenic nature).
- Guyton and Hall Textbook of Medical Physiology
2. Impaired Nitric Oxide Availability
Endothelial dysfunction from hypoxia impairs the release of nitric oxide (NO), a key pulmonary vasodilator. HAPE-prone individuals have reduced exhaled NO levels at high altitude. This explains why phosphodiesterase-5 (PDE-5) inhibitors (e.g., tadalafil, sildenafil) - which potentiate NO - are effective in HAPE prevention.
3. Sympathetic Overactivation
Hypoxia triggers increased sympathetic drive, causing pulmonary venoconstriction and extravasation from pulmonary capillaries into alveoli. Alpha-adrenergic blockade (phentolamine) improves HAPE haemodynamics more than other vasodilators. HAPE-susceptible individuals display enhanced sympathetic activity even during short-term hypoxic breathing at low altitude.
4. Elevated Endothelin-1
The endothelium also produces endothelin-1, a potent vasoconstrictor. Concentrations of endothelin-1 are higher than average in HAPE-prone mountaineers, amplifying vasoconstriction.
5. Impaired Alveolar Fluid Clearance
Beta-adrenergic agonists upregulate transepithelial sodium and water clearance from alveoli. HAPE may partly result from impaired alveolar fluid clearance, which is why inhaled salmeterol reduces HAPE incidence by ~50%.
6. Inflammation (Secondary Role)
Patients often have fever, leukocytosis, and raised ESR - but evidence suggests inflammation is an epiphenomenon rather than the primary driver. Viral respiratory infections predispose to HAPE even in normally resistant individuals.
- Harrison's Principles of Internal Medicine, 22nd Edition
Clinical Features
Symptoms (progressive)
- Reduced exercise tolerance (often the earliest sign, disproportionate to altitude)
- Dry, persistent cough (nearly universal in mountain climbers - not specific alone)
- Blood-tinged or frothy sputum (as oedema develops)
- Dyspnoea at rest
- Mental confusion, hallucinations, stupor, seizures, coma (advanced)
- Cheyne-Stokes breathing and oliguria may develop
Signs
-
Tachypnoea and tachycardia at rest - important markers of progression
-
Crackles on auscultation (not diagnostic alone)
-
Cyanosis
-
May have concurrent signs of HACE (ataxia, altered consciousness)
-
Harrison's Principles of Internal Medicine, 22nd Edition
-
Park's Textbook of Preventive and Social Medicine
Investigations
Chest X-ray
Classic findings: patchy or localized opacities, often asymmetric, commonly in the right middle and lower zones. Streaky interstitial oedema may also be seen. Importantly:
- Kerley B lines are NOT seen (unlike cardiogenic pulmonary oedema)
- Bat-wing appearance is NOT seen
- Can mimic pneumonic consolidation - historically misdiagnosed as pneumonia
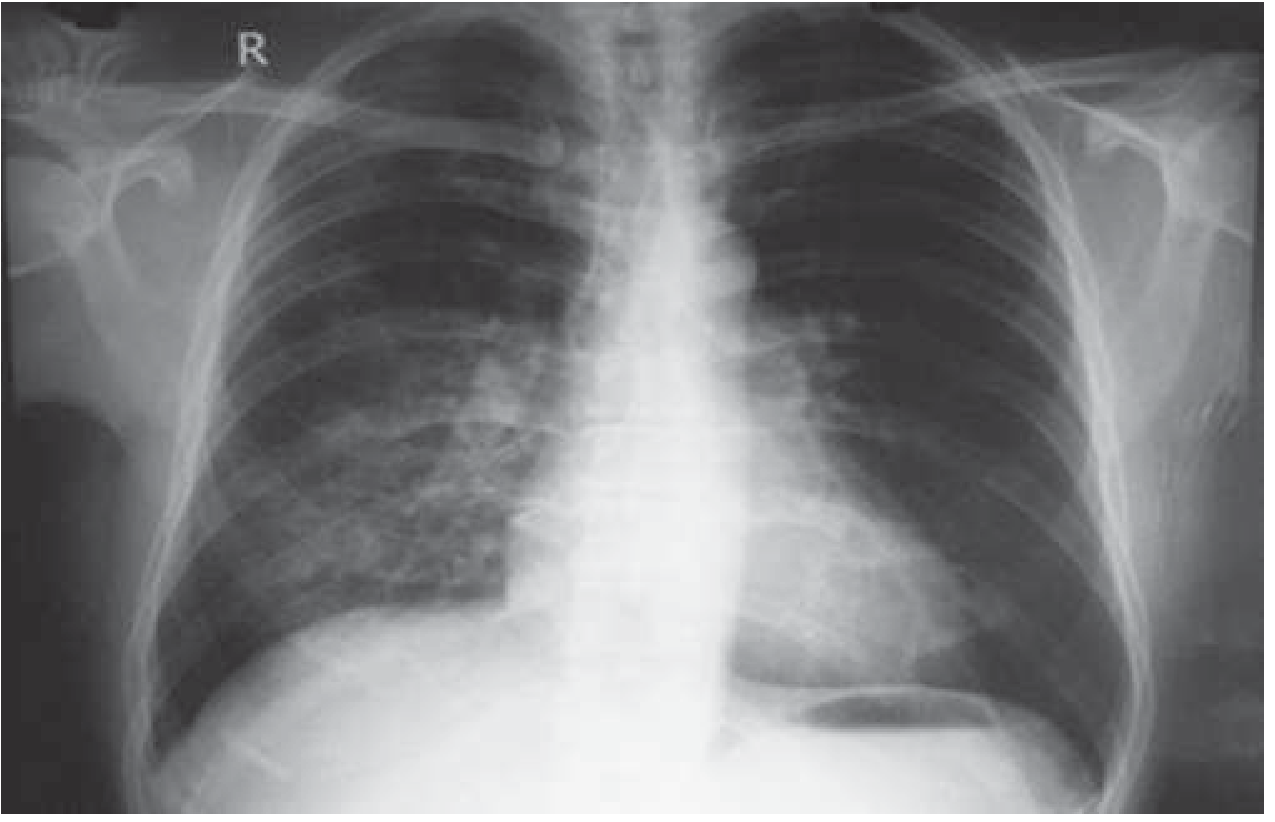
Chest X-ray of HAPE showing right middle and lower zone opacification. - Harrison's, 22nd Edition
ECG
- Right ventricular strain or hypertrophy pattern
ABG / Oximetry
- Hypoxaemia - consistently present
- Respiratory alkalosis - consistently present (unless on acetazolamide, where metabolic acidosis may supervene)
- Pulse oximetry is generally sufficient; formal ABG not mandatory
Echocardiography
- Recommended when HAPE develops at relatively low altitudes (<3,000 m) or when underlying cardiopulmonary abnormalities are suspected
Ultrasound
- Comet-tail scoring (B-lines) is sensitive but not specific for HAPE - many individuals without HAPE also show B-lines at altitude
Differential Diagnosis
- Pneumonia
- Pulmonary embolism
- Pneumothorax
- Anxiety attack / hyperventilation
- Cardiogenic pulmonary oedema
Treatment
1. Immediate Descent (Priority #1)
Descent is the single most effective treatment - symptoms respond rapidly. It is mandatory when HAPE is diagnosed.
2. Supplemental Oxygen
- High-flow oxygen reverses hypoxic vasoconstriction and usually leads to dramatic improvement within hours.
3. Portable Hyperbaric Chamber (Gamow bag)
- Simulates descent by increasing ambient pressure
- Provides "spectacular improvement" and buys time when descent is impossible
- Lightweight and used in remote locations
4. Pharmacological Treatment
| Drug | Role | Dose |
|---|---|---|
| Nifedipine (calcium channel blocker) | Treatment and prevention of HAPE | 30 mg SR every 12h OR 20 mg SR every 8h |
| Tadalafil (PDE-5 inhibitor) | Prevention of HAPE | 10 mg twice daily |
| Salmeterol (beta-2 agonist) | Prevention of HAPE | 125 mcg inhaled twice daily |
| Dexamethasone | Prevention of HAPE (78% reduction in incidence) | 8 mg once, then 4 mg every 6h for treatment |
- Goldman-Cecil Medicine, International Edition
- Harrison's Principles of Internal Medicine, 22nd Edition
Note on PDE-5 inhibitors: Tadalafil prophylaxis reduces HAPE risk by 65%. Dexamethasone reduces it by 78% - possibly via both NO enhancement and sympathetic dampening. However, PDE-5 inhibitors have no role in treating established AMS or HACE.
5. Position
- Sitting upright reduces venous return and pulmonary capillary pressure.
Prevention
- Slow, graded ascent - most important preventive measure (limit gain in sleeping altitude to ~300-500 m/day above 3,000 m, with a rest day every 3 days)
- Avoid over-exertion in the first 48 hours at new altitude
- Pharmacological prophylaxis in HAPE-susceptible individuals: nifedipine, tadalafil, or salmeterol (see table above)
- Acetazolamide (125-250 mg twice daily) is primarily for AMS/HACE prevention, not HAPE - but is an important overall prophylactic drug for altitude illness
Key Distinguishing Points (vs. Cardiogenic Pulmonary Oedema)
| Feature | HAPE | Cardiogenic PE |
|---|---|---|
| Pulmonary artery wedge pressure | Normal | Elevated |
| Kerley B lines | Absent | Present |
| Bat-wing appearance | Absent | Common |
| Cardiomegaly on CXR | Absent | Often present |
| Context | High altitude | Cardiac disease |
| ECG | RV strain | LV strain/ischaemia |
Recent Evidence (2024-2026)
- A 2024 review in Internal Medicine examines clinical and pathophysiological features of HAPE, including data from high-altitude studies in the Japanese population - highlighting reduced exercise tolerance and exaggerated hypoxic pulmonary vasoconstriction as the core mechanism.
- A 2026 review in Signal Transduction and Targeted Therapy (PMID 41571626) covers altitude hypoxia and hypoxaemia pathogenesis and management, including molecular targets.
- A 2025 pharmacological review (PMID 40516140) covers molecular and clinical insights into high-altitude physiology, including pharmacological interventions.
No recent meta-analyses or RCTs contradict standard management; descent + oxygen remain the cornerstone of treatment.
This is a shared conversation. Sign in to Orris to start your own chat.