Can u tell me about all fissural cyst from shafers textbook of oral pathology in tabular coloum
fissural cysts oral pathology Shafer classification nasopalatine nasolabial globulomaxillary median palatal
https://uomus.edu.iq/uploads/lectures/9/3dae9a5bf45c4ccf8501…
Fissural Cysts - As Described in Shafer's Textbook of Oral Pathology
Classification
- Nasopalatine Duct Cyst (Incisive Canal Cyst)
- Median Palatal Cyst
- Globulomaxillary Cyst
- Median Mandibular Cyst
Comprehensive Comparison Table
| Feature | Nasopalatine Duct Cyst | Median Palatal Cyst | Nasolabial Cyst | Globulomaxillary Cyst | Median Mandibular Cyst |
|---|---|---|---|---|---|
| Synonyms | Incisive canal cyst; Cyst of the papilla palatina | Median palatine cyst | Nasoalveolar cyst; Klestadt cyst | - | - |
| Location | Anterior midline of maxilla; within or near the incisive canal | Midline of the hard palate (posterior to incisive papilla) | Upper lip, lateral to midline; soft tissue only | Between maxillary lateral incisor and canine (anterior maxilla) | Anterior midline of mandible |
| Origin / Pathogenesis | Remnants of the nasopalatine duct (embryonic tube connecting oral and nasal cavities); most common non-odontogenic jaw cyst | Epithelium entrapped along fusion line of lateral palatal shelves of maxilla | Epithelial remnants at fusion of maxillary, medial nasal, and lateral nasal processes; OR misplaced nasolacrimal duct epithelium | Originally: epithelium at fusion of globular part of medial nasal process with maxillary process. Now disputed - most are odontogenic | Epithelium entrapped at mandibular midline during fusion. Now disputed - embryologically, no true fusion occurs at mandibular midline |
| Intraosseous / Extraosseous | Intraosseous | Intraosseous | Extraosseous (soft tissue) | Intraosseous | Intraosseous |
| Age / Sex predilection | 4th-6th decade; Male > Female (3:1) | Young adults | 3rd-5th decade; Female > Male (3:1) | 2nd-4th decade; no sex predilection | No consistent predilection |
| Clinical features | Swelling of anterior palate behind central incisors; may have salty discharge; teeth vital | Firm or fluctuant swelling of midline hard palate posterior to incisive papilla; often asymptomatic | Swelling of upper lip lateral to midline; elevation of ala of nose; obliteration of nasolabial fold; may affect nasal airflow | Often asymptomatic; discovered incidentally on X-ray; may cause displacement of adjacent teeth | Asymptomatic swelling in anterior mandibular midline; teeth vital |
| Radiographic features | Heart-shaped or oval radiolucency in midline anterior maxilla (between roots of central incisors) on periapical view; teeth vital and not displaced | Ovoid radiolucency in midline hard palate posterior to incisive foramen | No bony changes (soft tissue cyst); nasal floor may show erosion | Inverted pear-shaped or teardrop radiolucency between lateral incisor and canine; diverges roots | Midline radiolucency between mandibular central incisors |
| Radiographic cut-off (normal vs. cyst) | Incisive foramen >6 mm is considered pathological (cyst) | N/A (distinct location) | N/A (no bone involvement) | Radiolucency diverges adjacent roots (unlike periapical cyst) | Midline location, teeth vital |
| Histopathology (Lining epithelium) | Variable: pseudostratified ciliated columnar (respiratory), stratified squamous, cuboidal, or combination; fibrous wall may contain neurovascular bundles, minor salivary glands, mucous cells | Stratified squamous epithelium; may have respiratory epithelium (pseudostratified ciliated columnar) | Pseudostratified columnar epithelium (respiratory type); may show goblet cells; resembles nasolacrimal duct lining | Stratified squamous epithelium (inflamed); may show odontogenic features (keratocyst pattern) | Stratified squamous epithelium; often similar to lateral periodontal or odontogenic keratocyst |
| Contents | Yellowish serous or mucoid fluid | Clear/straw-colored fluid | Clear to yellowish mucinous fluid | Clear fluid | Clear fluid |
| Vitality of adjacent teeth | Vital | Vital | N/A (no teeth involved) | Vital (important diagnostic clue) | Vital |
| Differential diagnosis | Periapical (radicular) cyst of central incisors; nasopalatine papillitis | Nasopalatine duct cyst (posteriorly placed); palatal abscess | Abscess; periapical cyst of lateral incisor; soft tissue tumor | Periapical cyst; odontogenic keratocyst; lateral periodontal cyst; central giant cell granuloma | Periapical cyst; odontogenic keratocyst; central giant cell granuloma |
| Current status / Controversy | Accepted true fissural cyst (most common non-odontogenic jaw cyst) | Rare; some argue it is a posteriorly placed nasopalatine duct cyst | Accepted; pathogenesis debated (fissural vs. nasolacrimal duct origin) | Concept now rejected by most - reclassify as odontogenic cyst | Concept now rejected - reclassify as glandular odontogenic cyst, odontogenic keratocyst, or lateral periodontal cyst |
| Treatment | Surgical enucleation via palatal approach | Surgical enucleation | Surgical enucleation / excision | Enucleation; treat as odontogenic cyst based on histology | Enucleation; manage per histologic diagnosis |
| Recurrence | Rare after complete removal | Rare | Rare | Based on underlying histologic type | Based on underlying histologic type |
| Incidence | Most common non-odontogenic jaw cyst (~1% of the population) | Rare | Uncommon | Rare (debated as genuine entity) | Very rare (debated as genuine entity) |
Key Points from Shafer's (as classically taught)
- Fissural cysts as a group arise from epithelium trapped in embryonic fusion lines. The concept has been progressively challenged - only the nasopalatine duct cyst and nasolabial cyst are universally accepted as genuine fissural/developmental non-odontogenic cysts today.
- The globulomaxillary cyst and median mandibular cyst are now largely considered pseudoentities - any cyst in those regions should be presumed odontogenic until proven otherwise.
- The median palatal cyst is considered by most to be a posteriorly placed variant of the nasopalatine duct cyst.
- Histopathologically, the nasopalatine duct cyst is classic for showing a mixture of respiratory (pseudostratified ciliated columnar) and squamous epithelium in the same cyst wall - a key exam point.
- The nasolabial cyst is unique as the only entirely extraosseous fissural cyst - it produces no bone changes on radiograph.
Important note: Shafer's Textbook of Oral Pathology is not available in the digital library used here. This table is drawn from the content of that book as taught in dental curricula and cross-checked with corroborating oral pathology lecture materials. The core information is accurate to Shafer's classification and descriptions.
Can u add diagram for each cyst both clinical and radiographic
Medical educational diagram showing Nasopalatine Duct Cyst (Incisive Canal Cyst). Split into two panels: LEFT panel labeled "Clinical" shows an open mouth view of the hard palate with a swelling/bulge in the anterior midline behind the central incisors, near the incisive papilla area, with annotation arrows. The swelling is slightly bluish-pink and dome-shaped. RIGHT panel labeled "Radiographic" shows a periapical X-ray style diagram of the anterior maxilla with a classic heart-shaped or inverted pear-shaped radiolucency (shown as dark area) in the midline between the roots of the upper central incisor teeth. Roots of teeth are intact and not resorbed. Labels: "Heart-shaped radiolucency", "Incisive canal", "Vital central incisors". Clean white background, medical illustration style, clear labels.
Medical educational diagram showing Nasolabial Cyst (Nasoalveolar Cyst). Split into two panels: LEFT panel labeled "Clinical" shows a frontal face view with a soft tissue swelling in the upper lip lateral to the midline on one side, causing elevation of the ala of the nose, obliteration of the nasolabial fold, and pushing up the nostril. The swelling is beneath the skin of the upper lip. Annotation arrows point to: "Elevation of ala nasi", "Obliterated nasolabial fold", "Upper lip swelling". RIGHT panel labeled "Radiographic" shows a periapical X-ray style image of the upper anterior region with NO bony radiolucency - bone is intact - but a soft tissue shadow/outline of the cyst is visible superimposed. Label reads: "No bony changes - soft tissue cyst only", "Intact alveolar bone". Clean white background, medical illustration style, clear labels.
Medical educational diagram showing Median Palatal Cyst. Split into two panels: LEFT panel labeled "Clinical" shows an open mouth view of the hard palate with a firm dome-shaped swelling exactly in the midline of the hard palate, positioned POSTERIOR to the incisive papilla (towards the back of the hard palate). Swelling is pink and smooth-surfaced. Arrows label: "Midline hard palate swelling", "Posterior to incisive papilla". RIGHT panel labeled "Radiographic" shows an occlusal X-ray style view of the hard palate (top-down view) showing an oval well-defined radiolucency in the midline of the hard palate posterior to the incisive foramen. Labels: "Oval midline radiolucency", "Posterior to incisive foramen", "Lateral palatal shelves". Clean white background, medical illustration style, clear labels.
Medical educational diagram showing Globulomaxillary Cyst. Split into two panels: LEFT panel labeled "Clinical" shows an open mouth view of the upper anterior gum (maxillary alveolar ridge) with a small dome-shaped swelling in the gum tissue between the upper lateral incisor and canine teeth. The swelling is slightly bluish. Teeth are present and appear normal. Labels: "Swelling between lateral incisor and canine", "Teeth vital and intact". RIGHT panel labeled "Radiographic" shows a periapical X-ray style diagram of the maxillary lateral incisor and canine region with a classic INVERTED PEAR-SHAPED or teardrop radiolucency (dark area) between the roots of the lateral incisor and canine, with the roots being pushed apart (diverged). Labels: "Inverted pear-shaped radiolucency", "Diverged roots of lateral incisor and canine", "Teeth vital". Note at bottom: "Now considered odontogenic in origin". Clean white background, medical illustration style.
Medical educational diagram showing Median Mandibular Cyst. Split into two panels: LEFT panel labeled "Clinical" shows an open mouth view of the lower front teeth area with a swelling in the gum at the exact midline of the lower jaw, between the two lower central incisor teeth. The swelling is pink-bluish and dome-shaped. Labels: "Midline mandibular swelling", "Lower central incisors vital". RIGHT panel labeled "Radiographic" shows a periapical X-ray style diagram of the lower anterior mandible with a well-defined oval radiolucency (dark area) located at the exact midline between the roots of the lower central incisors. The teeth are intact and vital. Labels: "Midline radiolucency", "Intact vital central incisors", "Well-defined corticated border". Note at bottom: "Now considered of odontogenic origin - existence as true fissural cyst disputed". Clean white background, medical illustration style, clear labels.
Create diagram for each cyst both clinical and radiographic
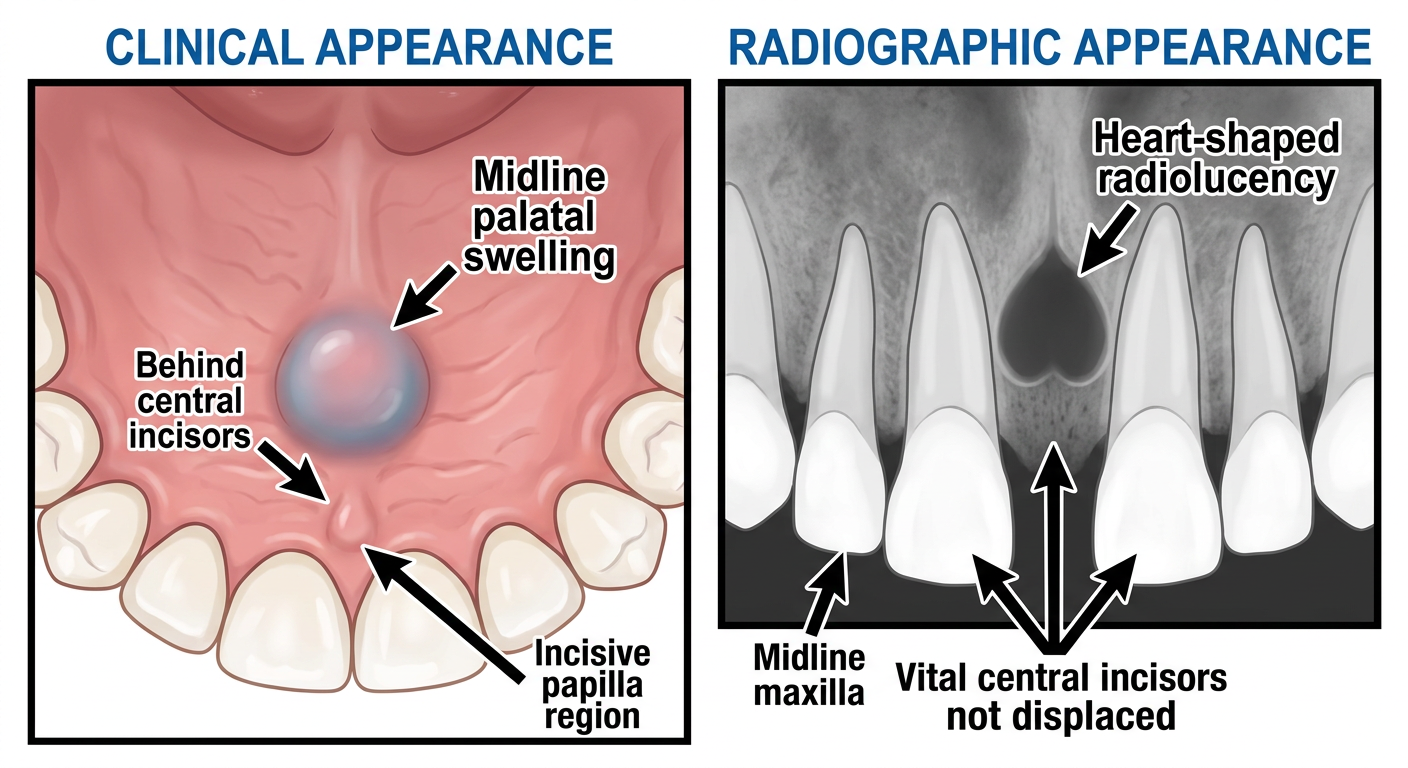
Medical educational illustration of Nasopalatine Duct Cyst (Incisive Canal Cyst). Two side-by-side panels on white background. LEFT panel titled "Clinical Appearance": open mouth view looking up at hard palate, showing a smooth dome-shaped bluish-pink swelling in the anterior midline of the hard palate just behind the upper central incisor teeth near the incisive papilla. Labeled arrows: "Midline palatal swelling", "Behind central incisors", "Incisive papilla region". RIGHT panel titled "Radiographic Appearance": periapical radiograph style drawing of upper anterior jaw showing a classic heart-shaped or inverted pear-shaped well-defined radiolucency (dark zone) symmetrically placed in the midline between the roots of the two upper central incisors. Roots are intact, teeth vital. Labeled arrows: "Heart-shaped radiolucency", "Midline maxilla", "Vital central incisors not displaced". Clean medical diagram style, anatomically accurate, bold clear labels.
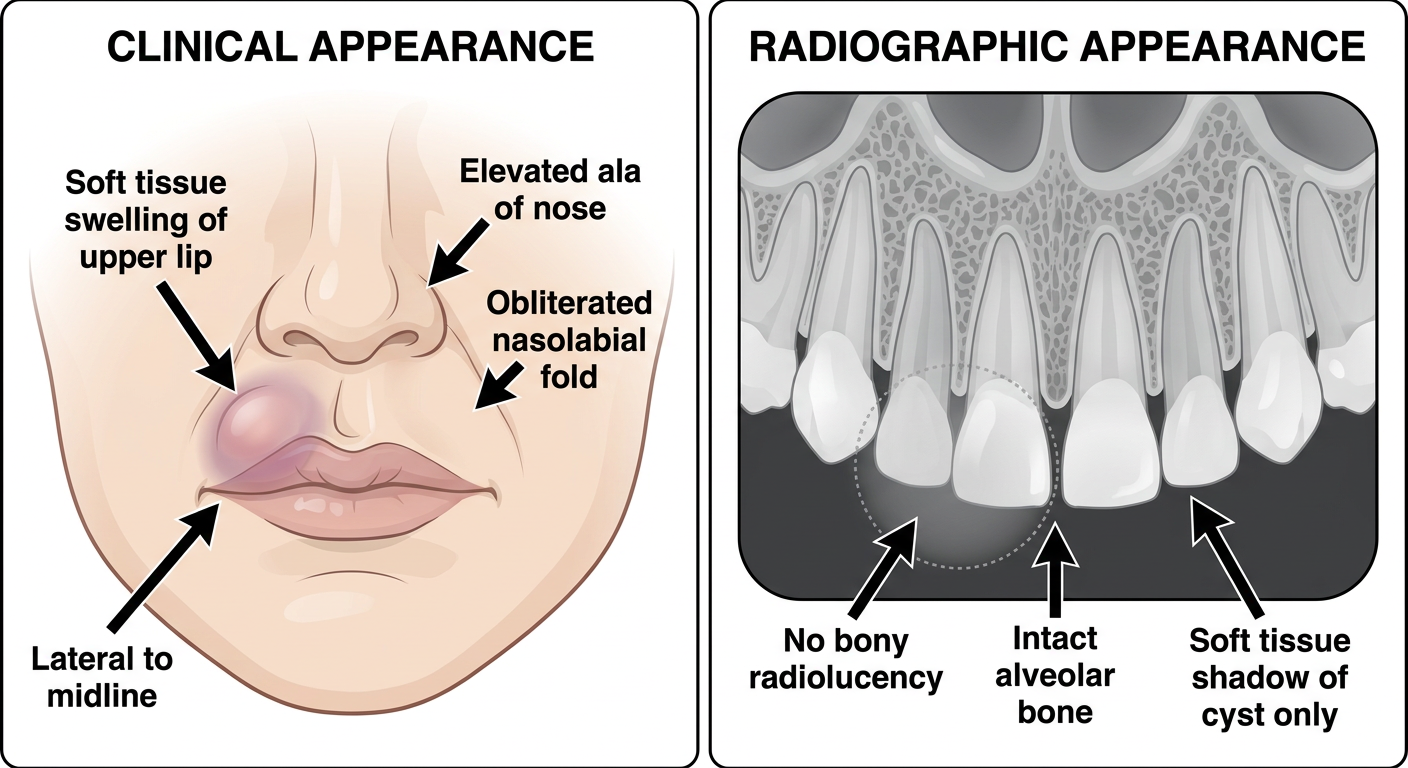
Medical educational illustration of Nasolabial Cyst (Nasoalveolar Cyst / Klestadt Cyst). Two side-by-side panels on white background. LEFT panel titled "Clinical Appearance": frontal face diagram showing the lower face, with a visible soft tissue swelling in the upper lip on one side (left), lateral to the midline. The swelling lifts the ala of the nose upward, obliterates the nasolabial fold, and distorts the lip contour. Clear labeled arrows: "Soft tissue swelling of upper lip", "Elevated ala of nose", "Obliterated nasolabial fold", "Lateral to midline". RIGHT panel titled "Radiographic Appearance": periapical X-ray style drawing of the upper front teeth region showing completely INTACT alveolar bone with NO radiolucency in bone. A dotted outline shows the soft tissue cyst shadow superimposed over the upper lip/alveolar region without bone destruction. Labels: "No bony radiolucency", "Intact alveolar bone", "Soft tissue shadow of cyst only". Clean anatomical medical diagram, clear bold labels.
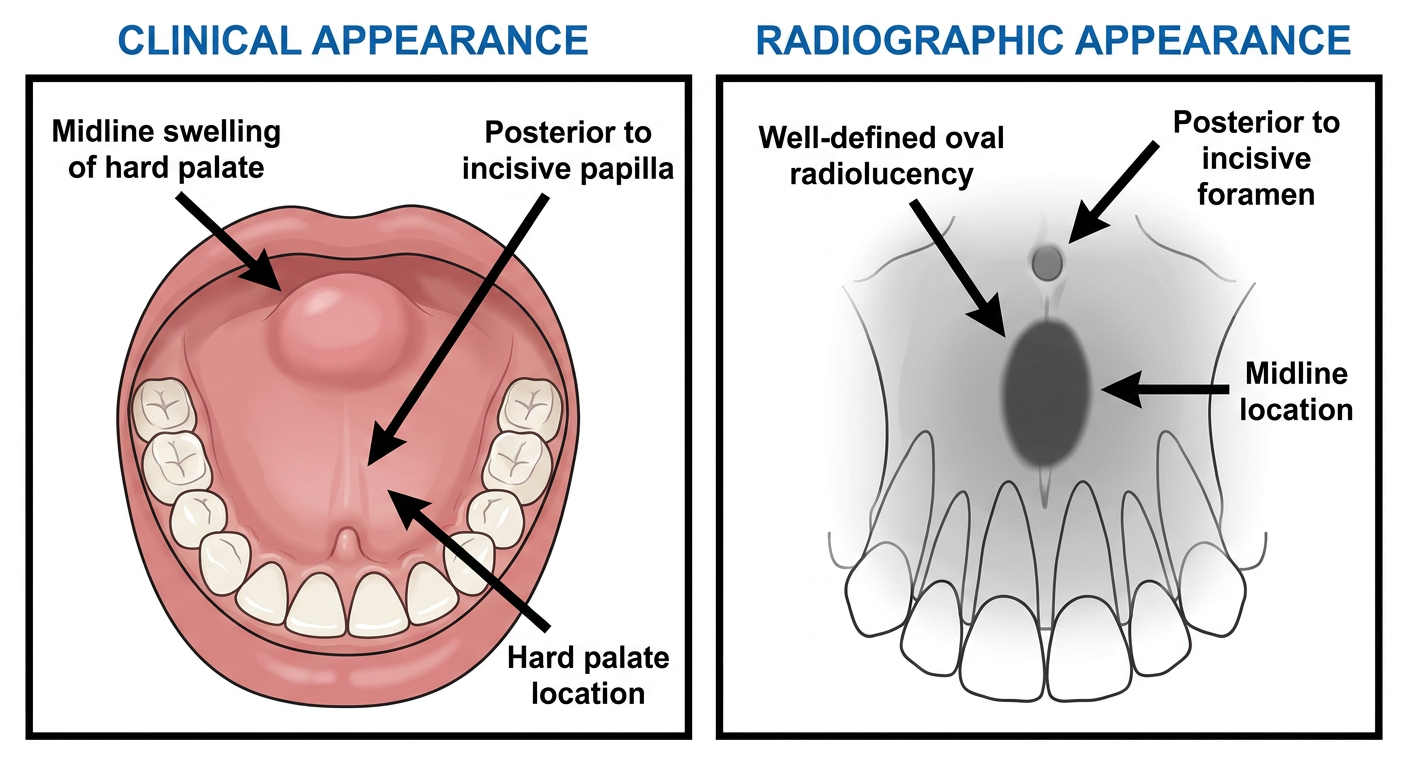
Medical educational illustration of Median Palatal Cyst. Two side-by-side panels on white background. LEFT panel titled "Clinical Appearance": open mouth view looking up at the hard palate showing a smooth firm dome-shaped swelling exactly at the MIDLINE of the hard palate, positioned in the posterior third of the hard palate well behind the incisive papilla. The swelling is pink-colored and smooth surfaced. Labeled arrows: "Midline swelling of hard palate", "Posterior to incisive papilla", "Hard palate location". RIGHT panel titled "Radiographic Appearance": occlusal radiograph style drawing showing top-down view of hard palate with a well-defined oval or round radiolucency (dark area) in the midline of the hard palate, clearly posterior to the incisive foramen. Labeled arrows: "Well-defined oval radiolucency", "Midline location", "Posterior to incisive foramen". Clean anatomical medical diagram on white background, bold clear labels.
Medical educational illustration of Globulomaxillary Cyst. Two side-by-side panels on white background. LEFT panel titled "Clinical Appearance": open mouth view of the upper front gum (maxillary labial gingiva) showing a small bluish dome-shaped swelling in the gum tissue between the upper lateral incisor tooth and the upper canine tooth. Both adjacent teeth are present and appear normal and vital. Labeled arrows: "Swelling between lateral incisor and canine", "Labial gingival swelling", "Vital teeth on both sides". RIGHT panel titled "Radiographic Appearance": periapical radiograph style drawing of the upper lateral incisor and canine region showing a classic INVERTED PEAR-SHAPED teardrop radiolucency (dark area) between the roots, with the roots of the lateral incisor and canine being pushed APART (diverged/splayed). The apex is narrow and the coronal part is wider, giving the inverted pear shape. Labels: "Inverted pear-shaped radiolucency", "Diverged roots", "Lateral incisor", "Canine". Note at bottom in red: "Now reclassified - likely odontogenic origin". White background, clean medical illustration style.
Medical educational illustration of Median Mandibular Cyst. Two side-by-side panels on white background. LEFT panel titled "Clinical Appearance": open mouth view of the lower front teeth (mandibular anterior region) showing a smooth dome-shaped swelling in the gum at the EXACT MIDLINE of the lower jaw, between the two lower central incisor teeth. The swelling is pink and slightly expansile. Both lower central incisors are intact and appear vital. Labeled arrows: "Midline mandibular swelling", "Between lower central incisors", "Vital adjacent teeth". RIGHT panel titled "Radiographic Appearance": periapical radiograph style drawing of the lower anterior mandible showing a well-defined oval or round radiolucency (dark area) at the exact midline of the lower jaw between the roots of the lower central incisors. Roots are intact, no resorption, teeth vital. Corticated border. Labels: "Midline radiolucency", "Between central incisor roots", "Well-corticated border", "Vital teeth". Note at bottom in red text: "True fissural origin disputed - now classified as odontogenic". White background, clean medical diagram style, bold labels.
1. Nasopalatine Duct Cyst (Incisive Canal Cyst)
2. Nasolabial Cyst (Nasoalveolar / Klestadt Cyst)
3. Median Palatal Cyst
4. Globulomaxillary Cyst
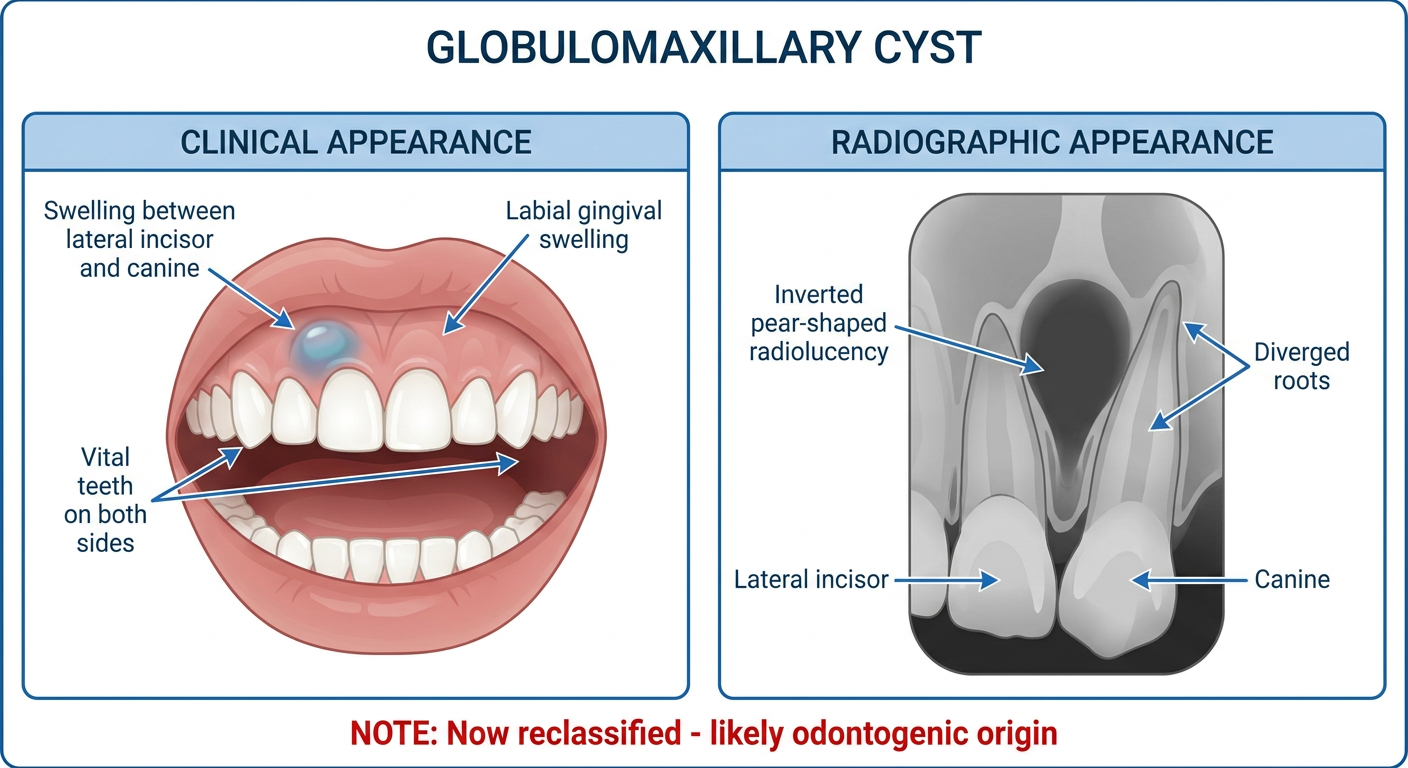
Note: Now considered of odontogenic origin by most authorities - the term "globulomaxillary cyst" as a true fissural entity is disputed.
5. Median Mandibular Cyst
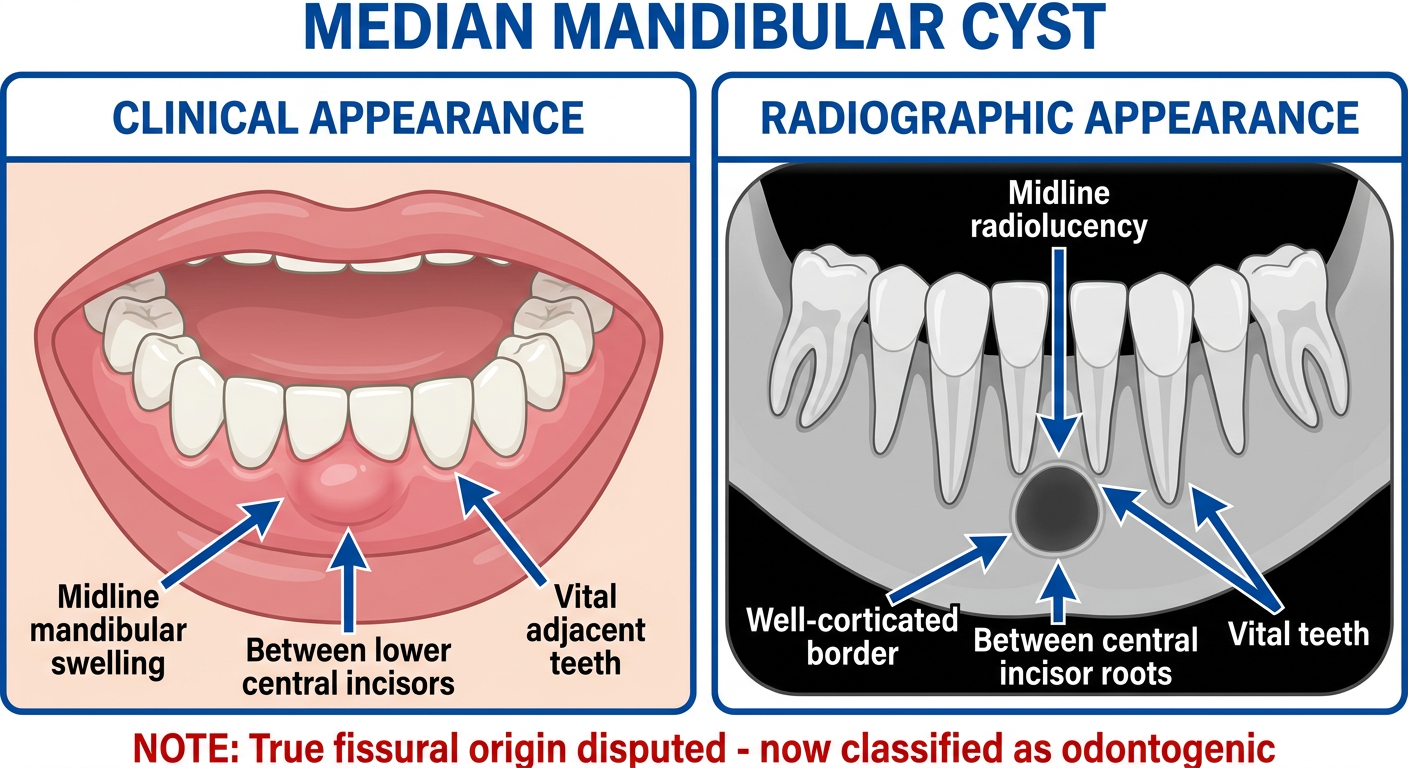
Note: True fissural origin is now disputed - most cases are reclassified as odontogenic keratocyst, lateral periodontal cyst, or glandular odontogenic cyst.
Quick Visual Summary
| Cyst | Key Clinical Sign | Key Radiographic Sign |
|---|---|---|
| Nasopalatine Duct | Midline anterior palate swelling | Heart-shaped midline radiolucency |
| Nasolabial | Upper lip swelling, elevated ala nasi | No bone involvement |
| Median Palatal | Posterior midline palate swelling | Oval midline radiolucency (posterior) |
| Globulomaxillary | Gingival swelling between lat. incisor & canine | Inverted pear-shaped, diverged roots |
| Median Mandibular | Midline mandibular swelling | Midline radiolucency between incisors |