Every detail for MBBS level about glaucoma from basics to clinical
Reading File
Finding Sources
Searching PubMed
glaucoma diagnosis management
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
I now have all the essential content needed. Let me compose the comprehensive MBBS-level glaucoma guide.
Glaucoma - Complete MBBS Guide
Sources: Kanski's Clinical Ophthalmology 10th ed., Robbins & Kumar Basic Pathology, Katzung's Pharmacology 16th ed., Goodman & Gilman's Pharmacological Basis of Therapeutics, Goldman-Cecil Medicine, Harrison's 22E
1. DEFINITION
Glaucoma is not a single disease but a group of conditions sharing a common final pathway: chronic progressive optic neuropathy with characteristic morphological changes at the optic nerve head (ONH) and retinal nerve fibre layer (RNFL), accompanied by progressive retinal ganglion cell (RGC) death and visual field loss. Intraocular pressure (IOP) is the key modifiable risk factor.
- Kanski's: "Glaucoma is the term used to describe a group of conditions that have in common a chronic progressive optic neuropathy that results in characteristic morphological changes at the optic nerve head and in the retinal nerve fibre layer."
- Goal of treatment: to slow progression throughout a patient's lifetime, maintaining visual function and quality of life.
Normal IOP: 10-21 mmHg (mean ~16 mmHg). Sustained IOP >21 mmHg = ocular hypertension.
2. AQUEOUS HUMOR DYNAMICS (Pathophysiology Foundation)
Understanding glaucoma requires understanding aqueous humor (AH) flow:
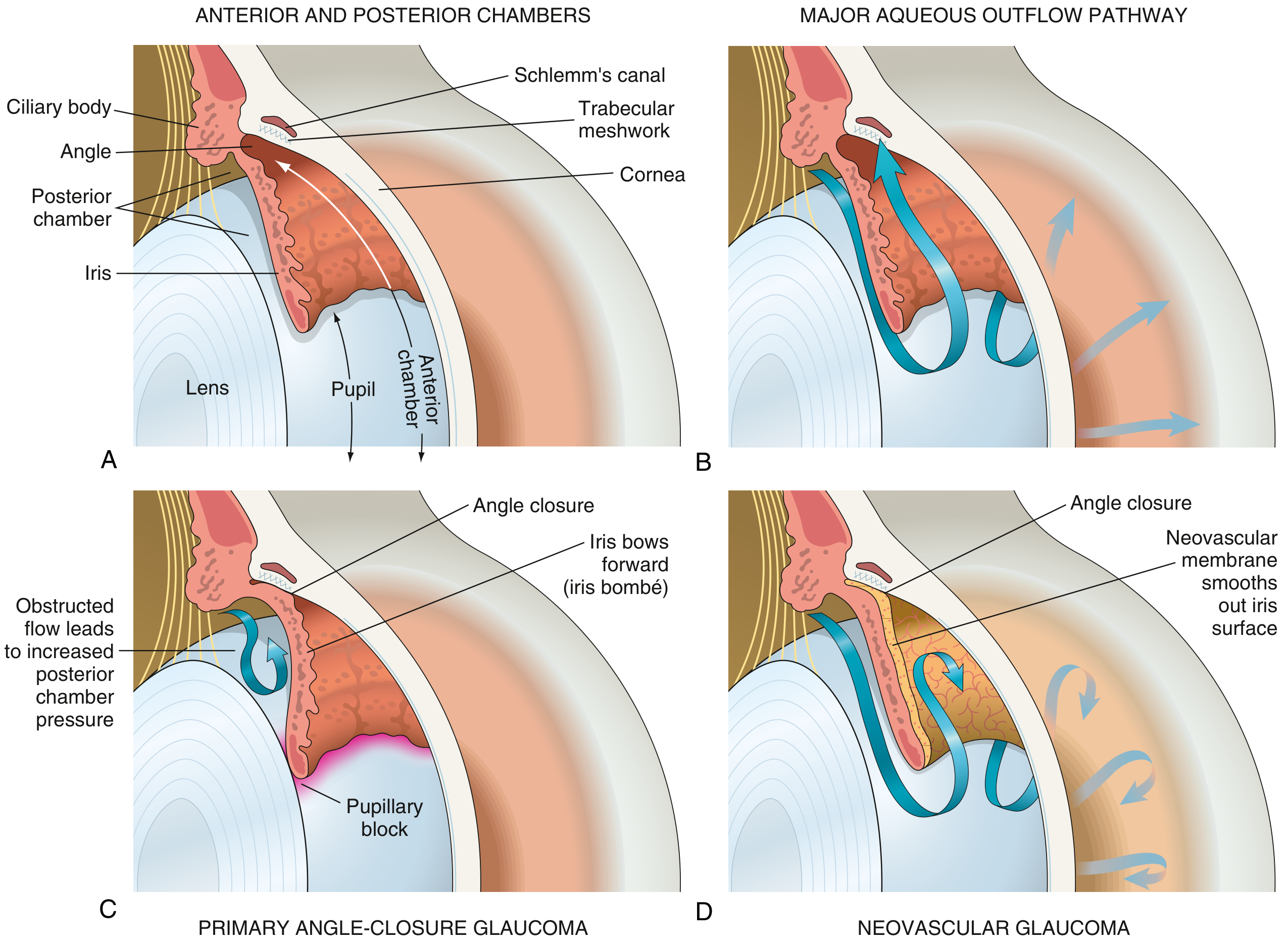
Formation: AH is produced by the ciliary body (epithelium) by active secretion (70-80%) and ultrafiltration (20-30%). Rate ~2-3 µL/min.
Drainage pathways:
- Trabecular (conventional) pathway (~85%): Posterior chamber → pupil → anterior chamber → trabecular meshwork (TM) → Schlemm's canal → episcleral veins. This is the pressure-dependent route.
- Uveoscleral (unconventional) pathway (~15%): Through ciliary muscle bundles to supraciliary/suprachoroidal space. Pressure-independent; enhanced by prostaglandins.
IOP = (Rate of AH production) / (Resistance to outflow) + Episcleral venous pressure
Elevated IOP occurs due to:
- Increased production (rare)
- Decreased trabecular outflow (most common)
- Raised episcleral venous pressure (e.g., Sturge-Weber, AV fistula)
3. CLASSIFICATION
| Basis | Types |
|---|---|
| Mechanism | Open-angle vs. Angle-closure |
| Etiology | Primary vs. Secondary |
| Age at onset | Congenital / Infantile / Juvenile / Adult |
Full Classification:
GLAUCOMA
├── Primary
│ ├── Primary Open-Angle Glaucoma (POAG)
│ │ └── Normal Tension Glaucoma (NTG) - subset
│ ├── Primary Angle-Closure Glaucoma (PACG)
│ └── Primary Congenital Glaucoma
└── Secondary
├── Open-angle: Pigmentary, Pseudoexfoliation, Steroid-induced, Traumatic
└── Angle-closure: Neovascular, Phacolytic, Phacomorphic, Lens-induced
4. PRIMARY OPEN-ANGLE GLAUCOMA (POAG)
The most common form of glaucoma in people of European and African descent.
Epidemiology
- Prevalence in >70 years: ~6% in White, ~16% in Black, ~3% in Asian populations
- Affects both genders equally
- Most prevalent form globally (60-70% of all glaucoma cases)
Risk Factors
| Factor | Details |
|---|---|
| IOP | Higher IOP → greater risk; asymmetry ≥4 mmHg is significant |
| Age | More common in older individuals |
| Race | Black individuals: 4× more common, earlier onset, harder to control |
| Family history | Siblings: ~4× risk; offspring: ~2× risk |
| Myopia | Associated with increased incidence and susceptibility |
| Thin cornea (CCT) | Thin central corneal thickness → risk factor |
| Large optic disc | More vulnerable to damage |
| Vascular disease | HTN, cardiovascular disease, vasospasm (migraine), low OPP |
| Anti-VEGF therapy | Repeated intravitreal injections → sustained IOP elevation |
| β-blockers not a risk | Systemic calcium channel blockers may be associated |
Pathogenesis
Two main theories:
- Mechanical theory: Elevated IOP causes physical distortion of the lamina cribrosa, compressing and damaging RGC axons as they pass through
- Vascular theory: Reduced ocular perfusion pressure → ischaemia of the optic nerve head (explains NTG)
In both: progressive loss of RGCs and their axons → RNFL thinning → optic disc cupping → visual field loss.
Clinical Features
Symptoms: Asymptomatic until late stages. Peripheral vision loss often not noticed until >30-40% of RGCs are lost. No pain (key differentiator from angle-closure).
Signs - Optic Disc Changes (The Core Finding):
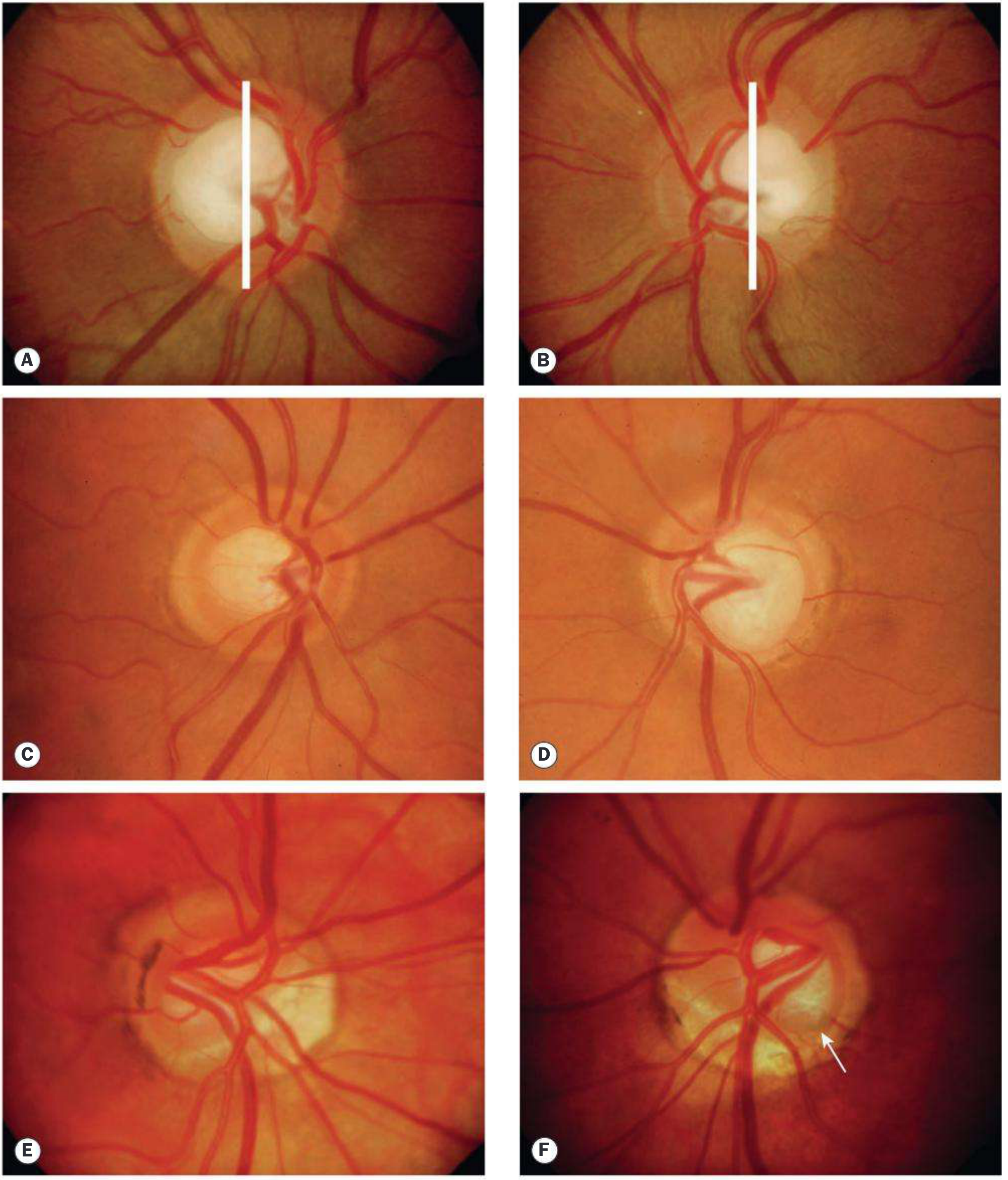
Key optic disc changes to look for:
| Sign | Description |
|---|---|
| Increased C/D ratio | Cup:Disc ratio >0.6 suspicious; >0.7-0.8 highly suspicious; asymmetry >0.2 between eyes |
| Thinning of NRR | Neuroretinal rim (NRR) thinning, especially inferior > superior > nasal > temporal (ISNT rule - normally Inferior is thickest) |
| Focal NRR notching | Particularly at inferior or superior poles |
| RNFL defects | Wedge-shaped RNFL defects visible with red-free fundus photography |
| Disc haemorrhages | Splinter/flame-shaped haemorrhages at disc margin (Drance haemorrhages) - more common in NTG |
| Vessel changes | Nasalization/baring of circumlinear vessels; "bayonetting" sign at disc margin |
| Laminar dots sign | Exposed lamina cribrosa pores visible through a deep cup |
| Parapapillary atrophy (PPA) | Zone β (inner) is more significant - adjacent to glaucomatous disc |
ISNT Rule: In a normal disc, the NRR width follows the order: Inferior > Superior > Nasal > Temporal. Violation of this rule suggests glaucoma.
Visual Field Defects (in order of progression)
- Enlarged blind spot (earliest, but non-specific)
- Paracentral scotomas - small depressions, often superonasally
- Nasal step - difference in sensitivity above and below horizontal midline in nasal field; bounded by horizontal raphe
- Arcuate (Bjerrum) scotoma - arcs from blind spot to nasal horizontal meridian (superior or inferior arcade follows nerve fibre bundle pattern)
- Ring scotoma - when superior and inferior arcuates connect
- Temporal wedge - less common, similar implications
- Advanced loss - only temporal island + central island remaining
- Tubular vision (end stage) - only central 5-10° preserved
- Total blindness
Note: SAP (standard automated perimetry) is used routinely. 24-2 pattern (tests to 24° temporal, 30° nasal) is the standard; 10-2 for advanced disease with split fixation.
Investigations
| Investigation | What it shows |
|---|---|
| Goldmann applanation tonometry | Gold standard for IOP measurement |
| Gonioscopy | Direct visualisation of angle - open angle with visible TM |
| Pachymetry (CCT) | Central corneal thickness - thin CCT underestimates IOP |
| Automated perimetry (HVF) | Visual field defects |
| OCT (Spectral domain) | Quantitative RNFL thickness, GCL analysis, disc parameters |
| HRT (Heidelberg Retina Tomograph) | 3D disc morphometry |
| GDx VCC | RNFL thickness by scanning laser polarimetry |
| Fundus photography | Baseline disc documentation |
IOP correction for CCT: For every 10 µm thinner than 545 µm, add ~1 mmHg; for every 10 µm thicker, subtract ~1 mmHg. (Goldmann tonometer calibrated for 520-540 µm)
Diagnosis
Requires ALL of:
- Open anterior chamber angle on gonioscopy
- Characteristic optic disc/RNFL changes
- Characteristic visual field defects (when present)
- Absence of secondary cause
Treatment of POAG
Target IOP: Generally aim for 30% reduction from untreated baseline, but must be individualized. Lower target for advanced disease (e.g., 12-15 mmHg) or NTG.
Step 1 - Medical (Eye drops first line):
| Drug Class | Example | Mechanism | Reduction in IOP |
|---|---|---|---|
| Prostaglandin analogues | Latanoprost, Bimatoprost, Travoprost, Tafluprost | ↑ Uveoscleral outflow (act at FP receptor) | 25-35% |
| β-blockers | Timolol 0.5% (non-selective), Betaxolol (β1-selective) | ↓ AH production (reduce cAMP in ciliary body) | 20-30% |
| α2-agonists | Brimonidine, Apraclonidine | ↓ AH production + ↑ uveoscleral outflow | 20-25% |
| Carbonic anhydrase inhibitors (CAI) | Dorzolamide, Brinzolamide (topical); Acetazolamide (oral) | ↓ AH production (inhibit CA-II in ciliary body) | 15-25% |
| Miotics (cholinergics) | Pilocarpine | ↑ Trabecular outflow (ciliary muscle contraction opens TM spaces) | 20-25% |
| Rho kinase inhibitors | Netarsudil | ↑ Trabecular outflow | 15-20% |
First-line: Prostaglandin analogues (once daily, most efficacious, good tolerance) or β-blockers (if PGA contraindicated or not tolerated).
Prostaglandin adverse effects: Iris hyperpigmentation (irreversible), periocular skin darkening, eyelash growth (hypertrichosis), CME in aphakic/pseudophakic eyes, rarely periocular fat atrophy.
β-blocker contraindications: Asthma, COPD, heart block, bradycardia. Timolol absorbed systemically - can cause bronchospasm, bradycardia. Betaxolol is β1-selective (less bronchospasm).
Oral acetazolamide adverse effects: Paraesthesias, metabolic acidosis, sulfonamide allergy, renal calculi, Stevens-Johnson syndrome, bone marrow suppression (rare).
Step 2 - Laser:
- Selective Laser Trabeculoplasty (SLT): Can be used as first-line (LiGHT trial: non-inferior to drops). 532 nm frequency-doubled Nd:YAG laser targets pigmented TM cells. 80 laser spots over 360°. Repeatable. 25-30% IOP reduction.
- Argon Laser Trabeculoplasty (ALT): Older modality, not repeatable.
Step 3 - Surgery:
- Trabeculectomy (guarded filtration surgery): Creates a fistula between anterior chamber and subconjunctival space. MMC (mitomycin C) or 5-FU used to prevent scarring. Gold standard surgical procedure.
- Glaucoma Drainage Devices (GDD/Tube shunts): Ahmed, Baerveldt, Molteno devices - for complex cases/failed trabeculectomy.
- Minimally Invasive Glaucoma Surgery (MIGS): iStent, Hydrus, OMNI - less risk but less IOP reduction. Best combined with cataract surgery.
- Cyclodestructive procedures: Diode laser cyclodiode ablation - reduces AH production by destroying ciliary body. Reserved for end-stage/blind painful eyes.
5. NORMAL TENSION GLAUCOMA (NTG)
- IOP consistently ≤21 mmHg but glaucomatous disc and field damage present
- ~30-40% of POAG patients have NTG
- Pathogenesis: Vascular insufficiency (vasospasm, nocturnal hypotension, sleep apnoea, autoimmune) predominates over mechanical
- Disc haemorrhages more frequent; more localised, deeper scotomas closer to fixation
- Associations: Flammer syndrome, obstructive sleep apnoea, autoimmune diseases
- Treatment: Same drugs as POAG (aim lower target IOP); treat systemic vascular risk factors; CCBs (nifedipine) in selected patients
6. PRIMARY ANGLE-CLOSURE GLAUCOMA (PACG)
Overview
- "Angle closure" = occlusion of TM by peripheral iris (iridotrabecular contact, ITC)
- PACG may cause up to half of all glaucoma globally and is particularly prevalent in Asia (East and South)
- Progresses rapidly, more likely to cause visual loss than POAG
Anatomical Predisposition
Small, crowded anterior segment:
- Shallow anterior chamber
- Short axial length (hypermetropia)
- Anterior lens position (increases with age as lens thickens)
- Small corneal diameter
- Thick peripheral iris
Mechanisms (from anterior to posterior)
| Mechanism | Description |
|---|---|
| Pupillary block (most common, ~75%) | Aqueous cannot pass from posterior → anterior chamber through pupil → pressure builds posteriorly → iris bombé → peripheral iris pushed against TM |
| Plateau iris | Anteriorly rotated ciliary processes hold peripheral iris forward - angle closes even after iridotomy |
| Phacomorphic | Swollen/thick lens pushes iris forward |
| Malignant (ciliolenticular block) | Aqueous misdirection into vitreous - posterior; often post-surgical |
Gonioscopy - Shaffer Grading System
| Grade | Angle | Structures visible |
|---|---|---|
| Grade 4 (35-45°) | Wide open | Ciliary body visible |
| Grade 3 (25-35°) | Open | Scleral spur visible |
| Grade 2 (20°) | Narrow | Trabeculum visible, NOT scleral spur |
| Grade 1 (10°) | Very narrow | Only Schwalbe line ± top of TM |
| Slit | Extremely narrow | No structures, but no contact |
| Grade 0 (0°) | Closed | Iridocorneal contact |
Grades 0-1 are at risk of closure. Indentation gonioscopy distinguishes appositional (opens with pressure) from synechial (permanent PAS, does not open) closure.
Van Herick Method (slit-lamp estimation of angle depth):
- Slit beam at limbus, compare anterior chamber depth to peripheral corneal thickness
- Ratio <1/4 → narrow angle → formal gonioscopy needed
PACG Spectrum (Terminology)
| Term | Definition |
|---|---|
| PACS (Suspect) | ITC in ≥2 quadrants on gonioscopy, no PAS, no elevated IOP, no disc/field damage |
| PAC | ITC + elevated IOP and/or PAS, but NO glaucomatous damage |
| PACG | PAC + glaucomatous optic disc/field damage |
| Acute congestive attack | Sudden symptomatic IOP elevation due to acute angle closure |
ACUTE ANGLE-CLOSURE ATTACK (Clinical Emergency)
Precipitating factors:
- Mydriasis: dim lighting, anticholinergics (e.g., atropine, antihistamines, TCAs), sympathomimetics, motion sickness patches
- Topiramate (causes anterior rotation of ciliary body - unusual mechanism)
- Prone position (reading)
- Emotional stress
Symptoms:
- Sudden severe unilateral eye pain
- Blurred vision with coloured halos around lights (corneal oedema causing diffraction)
- Frontal headache, nausea, vomiting (may mimic acute abdomen/migraine)
- Photophobia
Signs:
- Ciliary/circumcorneal congestion (perilimbal injection)
- Corneal oedema (steamy, hazy cornea)
- Shallow anterior chamber (Oblique illumination test / van Herick)
- Mid-dilated, fixed, oval (vertically oval) pupil - key sign
- High IOP (often 40-80 mmHg)
- Corneal endothelial oedema (Haab's striae in congenital)
- Optic disc congestion
Risk to fellow eye: Prophylactic laser iridotomy mandatory to the fellow eye.
Management of Acute Attack
Immediate (Emergency - lower IOP fast):
-
Topical medications (instill with 3-5 min interval):
- Apraclonidine 0.5-1% (α2-agonist)
- Timolol 0.5% (β-blocker)
- Prednisolone 1% or dexamethasone 0.1% (reduce inflammation)
-
Pilocarpine 2%: 1 drop to affected eye, repeat after 30 min; 1% to fellow eye. Note: Do NOT repeat if IOP >40 mmHg (ischaemia renders iris sphincter unresponsive)
-
Analgesia + antiemetic
-
Systemic hyperosmotic agents (if topical insufficient):
- Mannitol 20%: 1-2 g/kg IV over 1 hour
- Oral glycerol 50%: 1 g/kg
- Oral isosorbide: 1-1.5 g/kg
- These raise serum osmolality → draw fluid from vitreous → reduce IOP
-
Oral/IV acetazolamide 250-500 mg (CAI - reduces AH production)
Resistant cases:
- Corneal indentation (force aqueous posteriorly to open angle)
- 50% topical glycerol to clear corneal oedema before laser
- Paracentesis (rapid IOP reduction, small risk)
- Early laser iridotomy/iridoplasty once cornea clears
Definitive treatment:
- Laser peripheral iridotomy (LPI): Creates a full-thickness hole in peripheral iris → equalizes pressure between posterior and anterior chambers → relieves pupillary block → angle opens. Bilateral (fellow eye prophylactically). Gold standard.
- Lens extraction (phacoemulsification): Particularly if significant phacomorphic component; increasingly favoured (EAGLE trial showed superior outcomes over LPI alone)
- Trabeculectomy: If persistent IOP elevation despite patent iridotomy
Post-attack:
- Continue pilocarpine 2% QDS; topical steroid for inflammation
- Repeat gonioscopy to confirm angle is open
- Low threshold for cataract surgery
7. PRIMARY CONGENITAL GLAUCOMA (PCG)
- Autosomal recessive (CYP1B1 gene mutation most common)
- Due to trabeculodysgenesis (maldevelopment of angle structures)
- Presents from birth to age 3 (most within first year)
Classic Triad:
- Epiphora (watering, photophobia)
- Blepharospasm (squinting in light)
- Corneal cloudiness (oedema)
Signs:
- Buphthalmos (ox eye): enlarged globe, due to scleral stretching in infants (sclera is distensible)
- Haab's striae: breaks in Descemet's membrane, horizontal or concentric, from distension
- Elevated IOP
- Deep, large cup
Treatment:
- Medical treatment is inadequate alone as a long-term measure
- Goniotomy (internal incision of angle, requires clear cornea) or Trabeculotomy (external approach): first-line surgical options
- Trabeculectomy + MMC: if above fail
- GDD: best for long-term IOP control if surgery fails
8. SECONDARY GLAUCOMAS
8a. Pseudoexfoliation (PXF) Glaucoma
- Deposition of grey-white fibrillar material on anterior segment structures (lens surface, TM, zonules)
- Leads to TM blockage and reduced outflow
- Associated with zonular weakness → cataract surgery complications (phacodonesis)
- Most common identifiable cause of secondary OAG worldwide
- More aggressive than POAG; responds less well to medications
8b. Pigment Dispersion Syndrome / Pigmentary Glaucoma
- Reversed pupillary block: concave iris bows backwards, rubbing against zonular packets → pigment dispersed into AH → deposited on TM → obstructs outflow
- Classic triad: Krukenberg spindle (vertical fusiform pigment on corneal endothelium), Sampaolesi line (TM pigment band), Spoke-wheel iris TID (transillumination defects)
- Young, myopic males
- Exercise/dilation can precipitate acute IOP spikes
- Treatment: pilocarpine (re-deepens AC, moves iris forward), laser iridotomy for reverse pupillary block
8c. Neovascular Glaucoma (NVG)
- New vessels grow on iris (rubeosis iridis) and angle
- Fibrovascular membrane contracts → PAS → closed angle
- Causes: central retinal vein occlusion (most common), diabetic retinopathy, CRAO, carotid occlusive disease ("hypoxic ocular syndrome")
- Treatment: anti-VEGF injections, panretinal photocoagulation (PRP), + surgical IOP control
8d. Steroid-Induced Glaucoma
- Topical > systemic > inhaled > nasal steroids
- Mechanism: Steroids increase TM resistance by accumulation of extracellular material (fibronectin, proteoglycans) and inhibition of phagocytosis in TM
- Steroid responder: Defined as IOP rise of ≥6-10 mmHg with steroids
- POAG patients and their relatives are particularly susceptible
- Management: Discontinue steroid; use IOP-lowering drops; may need surgery
8e. Phacolytic Glaucoma
- Hypermature cataract releases lens proteins through intact capsule
- Macrophages engulf proteins → engorged cells block TM
- Open-angle mechanism; severe inflammation
- Treatment: Urgent cataract extraction
8f. Phacomorphic Glaucoma
- Swollen/intumescent cataract pushes iris-lens diaphragm forward → angle closure
- Angle-closure mechanism
- Treatment: medical IOP reduction followed by urgent cataract extraction; iridotomy may help temporarily
8g. Traumatic Glaucoma
- Angle recession (from blunt trauma): rupture of ciliary body face → RGC damage, TM fibrosis over years
- Hyphaema → blood blocks TM
- Ghost cell glaucoma: degenerated RBCs from old vitreous haemorrhage block TM
- Lens dislocation → pupillary block
- Long-term monitoring needed after blunt ocular trauma
9. PHARMACOLOGY OF GLAUCOMA DRUGS (Detailed)
| Drug | Class | MOA | Dose | Key Side Effects | Contraindications |
|---|---|---|---|---|---|
| Latanoprost | PGA (FP agonist) | ↑ Uveoscleral outflow | 1 drop OD (night) | Iris pigmentation (irreversible), lash growth, CME, periocular fat atrophy | Aphakia, uveitic glaucoma (relative) |
| Bimatoprost | Prostamide | ↑ Both outflow pathways | 1 drop OD | Same as above; most potent | Same |
| Travoprost | PGA | ↑ Uveoscleral outflow | 1 drop OD | Same as above | Same |
| Timolol | Non-selective β-blocker | ↓ AH production (↓ cAMP) | 0.5% BD | Bradycardia, bronchospasm, depression, sexual dysfunction, masking of hypoglycaemia | Asthma, COPD, heart block, bradycardia, heart failure |
| Betaxolol | β1-selective blocker | ↓ AH production | 0.5% BD | Less bronchospasm than timolol | Heart block, severe heart failure |
| Brimonidine | Selective α2-agonist | ↓ AH production + ↑ uveoscleral outflow + possible neuroprotection | 0.2% TDS | Allergy, dry mouth, fatigue, CNS depression in infants | Infants (<2 yrs - fatal apnoea), MAOIs |
| Apraclonidine | α2-agonist | ↓ AH production | 0.5-1% TDS | Allergy (up to 40%), tachyphylaxis | Short-term use only |
| Dorzolamide | Topical CAI | ↓ AH production (inhibits CA-II) | 2% TDS | Stinging, superficial punctate keratitis, metallic taste | Sulfonamide allergy (relative) |
| Brinzolamide | Topical CAI | Same | 1% TDS | Less stinging than dorzolamide | Same |
| Acetazolamide | Systemic CAI | ↓ AH production | 250 mg QID or SR 500 mg BD | Paraesthesias (most common), metabolic acidosis, kidney stones, sulfa allergy, aplastic anaemia (rare) | Sulfonamide allergy, kidney/liver failure, sickle cell |
| Pilocarpine | Muscarinic agonist | ↑ Trabecular outflow (ciliary muscle contraction) | 2-4% QID | Miosis, brow ache, accommodative spasm, retinal detachment risk (myopes) | Acute asthma, recent MI |
| Netarsudil | Rho-kinase inhibitor | ↑ Trabecular outflow + ↓ AH production + ↓ episcleral venous pressure | 0.02% OD | Conjunctival hyperaemia, cornea verticillata | - |
Fixed combinations (improves compliance):
- Latanoprost + Timolol (Xalacom)
- Dorzolamide + Timolol (Cosopt)
- Brimonidine + Timolol (Combigan)
- Bimatoprost + Timolol (Ganfort)
10. GLAUCOMA SURGERY
Trabeculectomy
- Creates a guarded fistula under a scleral flap allowing AH to drain into subconjunctival space (bleb)
- Antifibrotics: 5-fluorouracil (5-FU) or Mitomycin C (MMC) applied to bleb area to inhibit fibroblast proliferation and prevent bleb scarring
- Complications: Hypotony, bleb leak, blebitis/endophthalmitis, choroidal effusion/haemorrhage, cataract progression, failure
Glaucoma Drainage Devices (GDD)
- Ahmed (FP7/S2), Baerveldt, Molteno
- Tube in anterior chamber → plate sutured to episclera posteriorly
- Used for: failed trabeculectomy, neovascular glaucoma, post-vitreoretinal surgery
MIGS (Minimally Invasive Glaucoma Surgery)
- iStent/iStent inject: Titanium stent through TM into Schlemm's canal
- Hydrus Microstent: Scaffold within Schlemm's canal
- OMNI: Viscodilation + trabeculotomy
- XEN Gel Stent: Gelatin stent from AC to subconjunctival space
- Lower risk profile than trabeculectomy; best combined with phaco; moderate IOP reduction
Cyclodestructive Procedures
- Diode laser cyclophotocoagulation (CPC): Transscleral delivery; damages ciliary processes → ↓ AH production
- Reserved for refractory/end-stage/blind painful eyes
- Risks: Phthisis bulbi, hypotony, pain
11. OCULAR HYPERTENSION (OHT)
- IOP consistently >21 mmHg with normal optic disc, normal visual fields, and open angles
- NOT the same as glaucoma; only ~9.5% convert to POAG over 5 years (OHTS study)
- Treatment reduces conversion to 4.4% (OHTS)
- Treat if: IOP ≥30 mmHg (>40% 5-year risk), or high-risk profile (thin CCT, large C/D ratio, older age, Black ethnicity)
- Monitoring acceptable for lower-risk individuals
12. OPTIC NERVE HEAD IMAGING (OCT)
Spectral domain OCT provides:
- RNFL thickness map (TSNIT: Temporal-Superior-Nasal-Inferior-Temporal pattern)
- Loss typically starts inferiorly and superiorly (corresponding to superior/inferior arcuate field defects)
- Ganglion Cell Layer (GCL) analysis: Macula GCL thinning mirrors RNFL loss
- Serial OCT critical for progression analysis
- OCT detects structural damage earlier than visual field loss (structural precedes functional)
13. GLAUCOMA IN PHACOMATOSES
-
Sturge-Weber syndrome: Glaucoma in ~30% ipsilateral to facial haemangioma; 60% develop before age 2 (buphthalmos). Mechanism: trabeculodysgenesis (early) + raised episcleral venous pressure from AV communication (late). Goniotomy/trabeculotomy for early-onset; GDD for others. High risk of choroidal effusion/haemorrhage during filtration surgery.
-
Neurofibromatosis type 1: Rare; when present, usually unilateral and congenital. Association with plexiform neurofibroma of upper eyelid. Mechanisms: angle anomaly, ectropion uveae.
14. QUICK REVISION TABLE: POAG vs PACG
| Feature | POAG | PACG (Acute) |
|---|---|---|
| Onset | Insidious | Sudden |
| Symptoms | Asymptomatic (late field loss) | Severe pain, halos, vomiting |
| IOP | Elevated (variable) | Very high (40-80 mmHg) |
| Cornea | Clear | Oedematous (steamy) |
| Anterior chamber | Normal/deep | Shallow |
| Pupil | Normal | Mid-dilated, fixed, oval |
| Angle (gonioscopy) | Open | Closed |
| Fundus | Disc changes when advanced | Disc congested/normal early |
| Race predilection | Black > White | Asian |
| Gender | M = F | F > M |
| Refraction | Myopia association | Hypermetropia association |
| Definitive treatment | IOP-lowering drops/SLT/surgery | Laser iridotomy; phaco |
15. EXAM HIGH-YIELD POINTS
- Normal IOP: 10-21 mmHg; Goldmann applanation is the gold standard tonometer
- POAG is chronic and painless; asymptomatic until late - "sneak thief of sight"
- Visual field defect starts peripherally in POAG (ring scotoma, then tunnel vision); in NTG, defects are closer to fixation
- Prostaglandin analogues are first-line medical therapy for POAG
- Acute angle closure is an emergency: mid-dilated fixed oval pupil + rocky hard eye + corneal oedema
- Pilocarpine is contraindicated when IOP >40 mmHg in acute attack (ischaemic iris fails to respond)
- Laser peripheral iridotomy is the definitive treatment for pupillary block angle closure
- Congenital glaucoma triad: epiphora + photophobia/blepharospasm + corneal cloudiness; buphthalmos is pathognomonic
- ISNT rule: Normal NRR is Inferior > Superior > Nasal > Temporal; violation = glaucoma
- Neovascular glaucoma: Think ischaemic conditions - CRVO, PDR, carotid occlusion
- Steroid-induced glaucoma: Any route of steroid administration; especially risky in POAG patients
- Acetazolamide: Most common side effect is paraesthesias (tingling of hands/feet)
- Timolol: Contraindicated in asthma (bronchospasm), heart block
- SLT is repeatable (unlike ALT); can be used as primary therapy (LiGHT trial)
- Trabeculectomy + MMC: Gold standard surgery; bleb complications are major concern
- NTG diagnosis requires: IOP always ≤21 mmHg + glaucomatous damage + exclude other causes (pituitary tumour compressing optic chiasm, etc.)
- C/D ratio >0.7 or asymmetry >0.2 warrants full glaucoma workup
- Brimonidine is absolutely contraindicated in infants (<2 years) - causes CNS depression and apnoea
- OCT shows structural damage before visual field loss - structural-functional correlation
- EAGLE trial: Lens extraction superior to laser iridotomy as initial treatment for PAC/PACG
All information compiled from: Kanski's Clinical Ophthalmology 10th Edition, Robbins & Kumar Basic Pathology, Katzung's Basic and Clinical Pharmacology 16th Edition, Goodman & Gilman's Pharmacological Basis of Therapeutics, Goldman-Cecil Medicine, Harrison's Principles of Internal Medicine 22E
Make a pharmacology table (PPT) on all glaucoma medications with dosing and contraindications
Reading File
Reading File
Reading File
Reading File
Running Command
Running Command
Writing File
Running Command
Running Command
Your presentation is ready!
Glaucoma Pharmacology
Presentation · PPTX
9 slides, wide format (13.3" × 7.5"), navy/teal color theme:
| Slide | Content |
|---|---|
| 1 | Cover - title, badge highlights, contents list |
| 2 | Overview table - all 6 drug classes, mechanisms, IOP reduction %, first-line status |
| 3 | Prostaglandin Analogues - Latanoprost, Bimatoprost, Travoprost, Tafluprost |
| 4 | Beta-Blockers - Timolol, Betaxolol, Levobunolol, Carteolol, Metipranolol |
| 5 | Alpha-2 Agonists - Brimonidine vs. Apraclonidine with exam warning box |
| 6 | Carbonic Anhydrase Inhibitors - Dorzolamide, Brinzolamide, Acetazolamide, Methazolamide |
| 7 | Miotics + Rho-Kinase Inhibitors - Pilocarpine, Netarsudil, Ripasudil |
| 8 | Hyperosmotic Agents - Mannitol, Glycerol, Isosorbide, Urea (acute emergency use) |
| 9 | Summary - Treatment algorithm, fixed combinations (Cosopt, Xalacom, etc.), contraindication panel, 10 exam high-yield facts |
Every table includes: drug name, concentration, dosing frequency, mechanism of action, adverse effects, and contraindications. Amber/red highlights flag critical contraindications throughout.
Create a case based study document with 5 rabies clinical scenarios bro
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.