A patient have irregular periods about 35 days and pain during periods
Reading File
Finding Sources
Finding Sources
Searching PubMed
irregular menstruation dysmenorrhea diagnosis management
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Here is a thorough clinical overview based on your patient's presentation: irregular cycles (~35 days) + painful periods (dysmenorrhea).
Clinical Assessment: Irregular Periods + Dysmenorrhea
Defining the Abnormalities
- Normal menstrual cycle: 21-35 days. A 35-day cycle sits at the upper edge of normal but is considered borderline oligomenorrhea (reduced frequency of periods), especially if cycles vary significantly month to month.
- Oligomenorrhea: cycles consistently >35 days.
- Dysmenorrhea: painful menstruation, most commonly due to excess prostaglandin accumulation in the uterine endometrium.
- Ganong's Review of Medical Physiology, p. 951: "Most of the symptoms of dysmenorrhea are due to accumulation of prostaglandins in the uterus."
Differential Diagnosis
The combination of irregular cycles + pain narrows the differential considerably:
1. Polycystic Ovary Syndrome (PCOS) - Most Common
- Affects 4-10% of premenopausal women.
- Rotterdam Criteria (diagnosis requires 2 of 3):
- Hyperandrogenism (acne, hirsutism, elevated androgens)
- Oligomenorrhea or amenorrhea
- Polycystic ovaries on ultrasound
- Clinical features at diagnosis:
- Oligomenorrhea: ~40% of patients
- Irregular cycle with anovulation
- May also have acne, excess facial/body hair, obesity, infertility
- Hormonal pattern: Normal/low FSH, elevated LH, normal estrogen
- Tietz Textbook of Laboratory Medicine, p. 2451, 2464-2468
2. Endometriosis
- Estimated in ~10% of reproductive-age women.
- Classic triad: dysmenorrhea + dyspareunia (pain during sex) + non-menstrual pelvic pain.
- Found in 20-90% of women with pelvic pain.
- Diagnosed definitively by laparoscopy with histologic confirmation.
- Berek & Novak's Gynecology, p. 617: "Endometriosis is associated with pelvic pain and infertility."
- Can also cause irregular cycles if associated with ovarian endometriomas affecting follicular function.
3. Primary Dysmenorrhea
- Painful periods without identifiable pelvic pathology.
- Common in young women; often improves after first pregnancy.
- Prostaglandin-mediated uterine cramping.
- Cycles may be slightly irregular but usually normalize with age.
4. Adenomyosis
- Endometrial glands within the myometrium.
- Causes heavy, painful periods; uterus is enlarged and "boggy."
- More common in women >30-35 years and multiparous.
5. Uterine Fibroids (Leiomyomas)
- Can cause irregular/heavy bleeding and dysmenorrhea.
- Diagnosed by pelvic ultrasound.
6. Thyroid Dysfunction / Hyperprolactinemia
- Hypothyroidism and elevated prolactin can cause oligomenorrhea and secondary dysmenorrhea.
Workup / Investigations
| Investigation | Purpose |
|---|---|
| Pelvic ultrasound (transvaginal if possible) | Polycystic ovaries, fibroids, adenomyosis, endometriomas |
| Serum LH, FSH, estradiol (Day 2-3 of cycle) | Hormonal profile, assess for PCOS |
| Testosterone (total + free), DHEA-S | Hyperandrogenism in PCOS |
| TSH, prolactin | Exclude thyroid/pituitary causes |
| CA-125 | Elevated in endometriosis (non-specific, but supportive) |
| Progesterone (Day 21) | Confirm ovulation |
| Complete blood count | Assess for anemia from heavy periods |
| Laparoscopy | Gold standard for endometriosis diagnosis |
Treatment Principles
For PCOS (oligomenorrhea-predominant):
- Combined oral contraceptive pills (COCPs) - regulate cycles and reduce androgen effects.
- Metformin - if insulin resistance/metabolic features present.
- Lifestyle modification (weight loss in overweight patients improves cycle regularity).
- Clomiphene/letrozole if fertility desired.
For Dysmenorrhea (primary):
- NSAIDs (ibuprofen, mefenamic acid) - first-line; inhibit prostaglandin synthesis.
- COCPs - second-line; reduce prostaglandin production.
- Recent evidence supports exercise as an effective non-pharmacological option (systematic review, BMC Women's Health, 2024).
- Zinc supplementation shows benefit per a 2024 meta-analysis (Nutrients, PMID 39683510).
For Endometriosis (if suspected/confirmed):
- Medical: COCPs, progestins, GnRH agonists - all equally effective for pain.
- Surgical: Laparoscopic ablation or excision of lesions.
- Berek & Novak's Gynecology, p. 2561: "Suppression of ovarian function reduces pain associated with endometriosis. Different classes of hormonal drugs - combination oral contraceptives, progestins, GnRH agonists - are equally effective in reducing pain."
Red Flags Requiring Urgent Evaluation
- Severe pelvic pain unresponsive to NSAIDs.
- Pain during intercourse (suggests endometriosis or deep pelvic pathology).
- Progressively worsening dysmenorrhea over months.
- Associated infertility.
- Fever with pelvic pain (suggests PID/infection).
Bottom Line
The most likely diagnoses in a reproductive-age woman with ~35-day cycles and dysmenorrhea are PCOS (with anovulatory cycles causing prostaglandin build-up and irregular periods) and/or endometriosis. A pelvic ultrasound + hormonal panel (LH, FSH, testosterone, TSH, prolactin) is the appropriate first-line workup. NSAIDs are appropriate symptomatic treatment for the pain while the workup is ongoing.
Note: This is a clinical overview for educational purposes. Patient management should be individualized based on full history, examination, and test results by a qualified clinician.
What diagnostic labs and imaging do you want to order first?
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Here is the structured first-line diagnostic workup for this patient, based on the most likely diagnoses (PCOS, endometriosis, primary dysmenorrhea):
First-Line Diagnostic Workup
Imaging - Order First
1. Transvaginal Pelvic Ultrasound (TVUS) - Priority #1
This is the single most informative first test.
What to look for:
| Finding | Suggests |
|---|---|
| ≥20 antral follicles per ovary OR ovarian volume ≥10 cm³ | PCOS |
| Endometrioma ("chocolate cyst" - ground-glass appearance) | Endometriosis |
| Enlarged, globular uterus with heterogeneous myometrium | Adenomyosis |
| Submucosal/intramural fibroids | Uterine fibroids |
Technique note: TVUS is preferred over transabdominal ultrasound for better resolution, especially in obese patients. In virginal patients, transabdominal ultrasound is used instead. Perform in the early follicular phase (Days 2-5) ideally. - Grainger & Allison's Diagnostic Radiology, p. 1244-1248
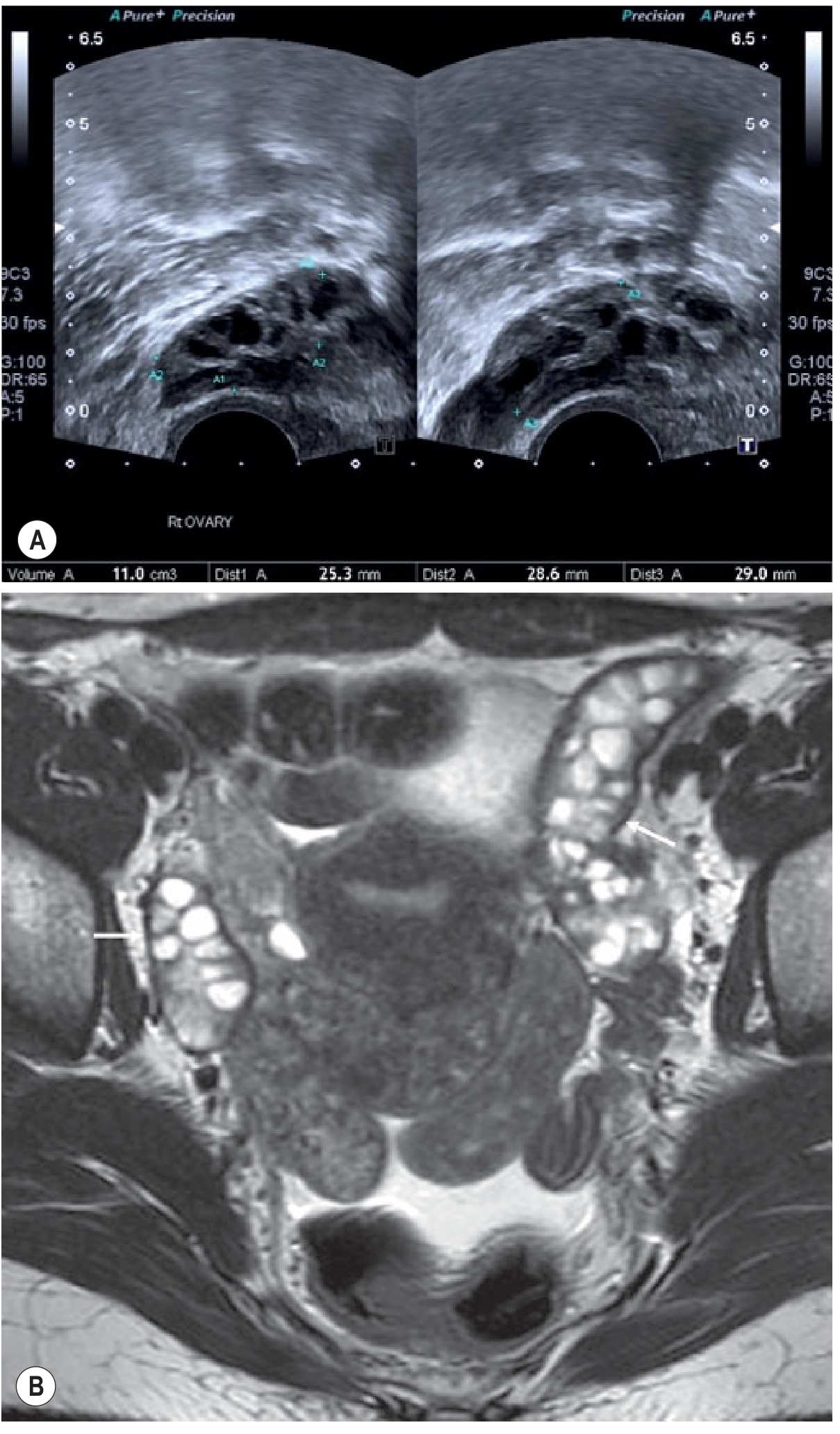
The image below shows what polycystic ovaries look like on TVUS (A) and MRI (B) - note the multiple peripheral follicles arranged around an echogenic stroma:
Blood Tests - Order at Same Visit
Order these on Days 2-5 of the menstrual cycle for hormonal tests (ideally Day 3):
Tier 1 - Essential (Order in ALL patients)
| Test | Why |
|---|---|
| Serum beta-hCG (urine/blood) | Rule out pregnancy FIRST before any other workup |
| FSH + LH (Day 2-3) | PCOS shows normal/low FSH with elevated LH; high FSH suggests premature ovarian insufficiency |
| Estradiol (E2) (Day 2-3) | Baseline ovarian reserve; low = POI, normal = typical in PCOS |
| Total testosterone + free testosterone | Hyperandrogenism - key criterion for PCOS |
| TSH | Hypothyroidism causes oligomenorrhea and worsens dysmenorrhea |
| Prolactin | Hyperprolactinemia causes irregular cycles (inhibits GnRH pulsatility) |
| CBC | Check for anemia from blood loss; rule out infection |
Tier 2 - Add Based on PCOS Suspicion
| Test | Why |
|---|---|
| DHEA-S | Adrenal androgen excess; differentiates adrenal from ovarian source |
| 17-OH Progesterone (Day 3, early morning) | Screens for late-onset congenital adrenal hyperplasia (CAH) - can mimic PCOS |
| Fasting glucose + insulin (HOMA-IR) | Insulin resistance in PCOS; guides metformin use |
| Fasting lipid panel | Metabolic risk assessment in PCOS |
| AMH (Anti-Mullerian Hormone) | Elevated in PCOS; also reflects ovarian reserve. The 2023 updated Rotterdam criteria allow elevated AMH as an alternative to polycystic ovaries on ultrasound. - Harrison's, p. 815 |
Tier 3 - Add if Endometriosis Suspected
| Test | Why |
|---|---|
| CA-125 | Elevated in endometriosis (not specific, but supports diagnosis if elevated with pain) |
| CRP / ESR | Elevated in significant pelvic inflammation/endometriosis |
Day 21 Progesterone (Mid-Luteal Phase)
- If Day 1 = first day of last period, draw Day 21 serum progesterone.
- >3 ng/mL confirms ovulation occurred. A low level confirms anovulation, strongly supporting PCOS.
Decision Tree After Results
Beta-hCG positive? → Manage as pregnancy (ectopic/intrauterine)
↓ negative
TVUS + hormones
↓
≥2 Rotterdam criteria met → Diagnose PCOS, start treatment
↓
Normal hormones + TVUS, but severe dysmenorrhea → Suspect endometriosis
→ Refer for laparoscopy (gold standard for endometriosis)
↓
Fibroid / adenomyosis on TVUS → Manage accordingly
Key Points from Updated Guidelines
Per the 2023 International PCOS Guidelines (cited in Harrison's 22E, p. 815):
- Diagnosis requires 2 of 3 Rotterdam criteria: irregular menses, hyperandrogenism (clinical or biochemical), and polycystic ovarian morphology on ultrasound OR elevated AMH.
- LH/FSH ratio alone is not used as a diagnostic criterion due to pulsatility variability.
- TSH and prolactin must be checked to exclude other causes before labeling PCOS.
- PCOS is a diagnosis of exclusion - other causes must be ruled out first.
This workup covers the two most likely diagnoses simultaneously and is cost-effective as a first step. If both TVUS and initial labs are non-diagnostic but pain persists, diagnostic laparoscopy is the next step for definitive endometriosis diagnosis.
This is a shared conversation. Sign in to Orris to start your own chat.