Describe the complications of rigid oesophagoscopy in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Searching PubMed
"rigid esophagoscopy" AND complications
Searching the Web
rigid oesophagoscopy complications RGUHS ENT exam Scott Brown Cummings Dhingra
Reading File
Reading File
Reading File
Reading Article
PMID: 38410347
Finding Sources
Finding Sources
Reading Web Page
https://www.entlecture.com/rigid-oesophagoscopy
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Searching the Web
rigid oesophagoscopy complications Zakir Hussain Hazarika Stell Maran ENT textbook perforation mediastinitis
Loading Image
Loading Image
COMPLICATIONS OF RIGID OESOPHAGOSCOPY
RGUHS 20-Mark Long Essay Answer
INTRODUCTION
Rigid oesophagoscopy is the direct endoscopic examination of the oesophagus using a hollow metal tube passed through the mouth under general anaesthesia. While it remains the gold standard for foreign body removal, complex stricture dilation, and biopsy of oesophageal lesions, it carries a distinct complication profile owing to the instrument's rigidity and the need for forceful alignment of the oral-pharyngeal-oesophageal axes (Boyce-Jackson position).
The overall complication rate of rigid aerodigestive endoscopy is reported between 1% and 8% (Cummings Otolaryngology). Instrumental perforation now accounts for more than half of all oesophageal perforations (Fishman's Pulmonary Diseases). The incidence of oesophageal perforation specifically with esophagoscopic examination ranges from 0.15% to 0.70% (Murray & Nadel's Textbook of Respiratory Medicine).
CLASSIFICATION OF COMPLICATIONS
COMPLICATIONS OF RIGID OESOPHAGOSCOPY
│
├── ANAESTHESIA-RELATED
│ ├── Cardiopulmonary depression
│ ├── Laryngospasm / bronchospasm
│ └── Aspiration pneumonia
│
├── INTRAOPERATIVE
│ ├── MINOR
│ │ ├── Mucosal laceration (most common: 38.9%)
│ │ ├── Endoluminal bleeding / haematoma (9.3%)
│ │ ├── Mucosal oedema (3.7%)
│ │ └── Dental avulsion / lip/tongue injury (1.9%)
│ │
│ └── MAJOR
│ ├── Oesophageal perforation (8%) ← MOST SERIOUS
│ ├── Haemorrhage
│ └── Failure to remove foreign body
│
└── POSTOPERATIVE
├── Oesophageal perforation sequelae:
│ ├── Cervical emphysema (1.2%)
│ ├── Pneumomediastinum (1.9%)
│ ├── Pneumothorax / hydropneumothorax (1.9%)
│ ├── Mediastinitis (1.2%)
│ └── Septic shock / Death (2.5%)
├── Abscess formation (3.1%)
├── Laryngeal oedema
└── Oesophageal stricture (late)
Complication rates from: Alexandre et al., Cureus 2024 [PMID: 38410347], n=162 patients
ANATOMICAL BASIS OF COMPLICATIONS
The three natural narrowings of the oesophagus are the most vulnerable sites for perforation:
Diagram: Oesophageal Landmarks and Danger Zones (from K.J. Lee's Essential Otolaryngology)
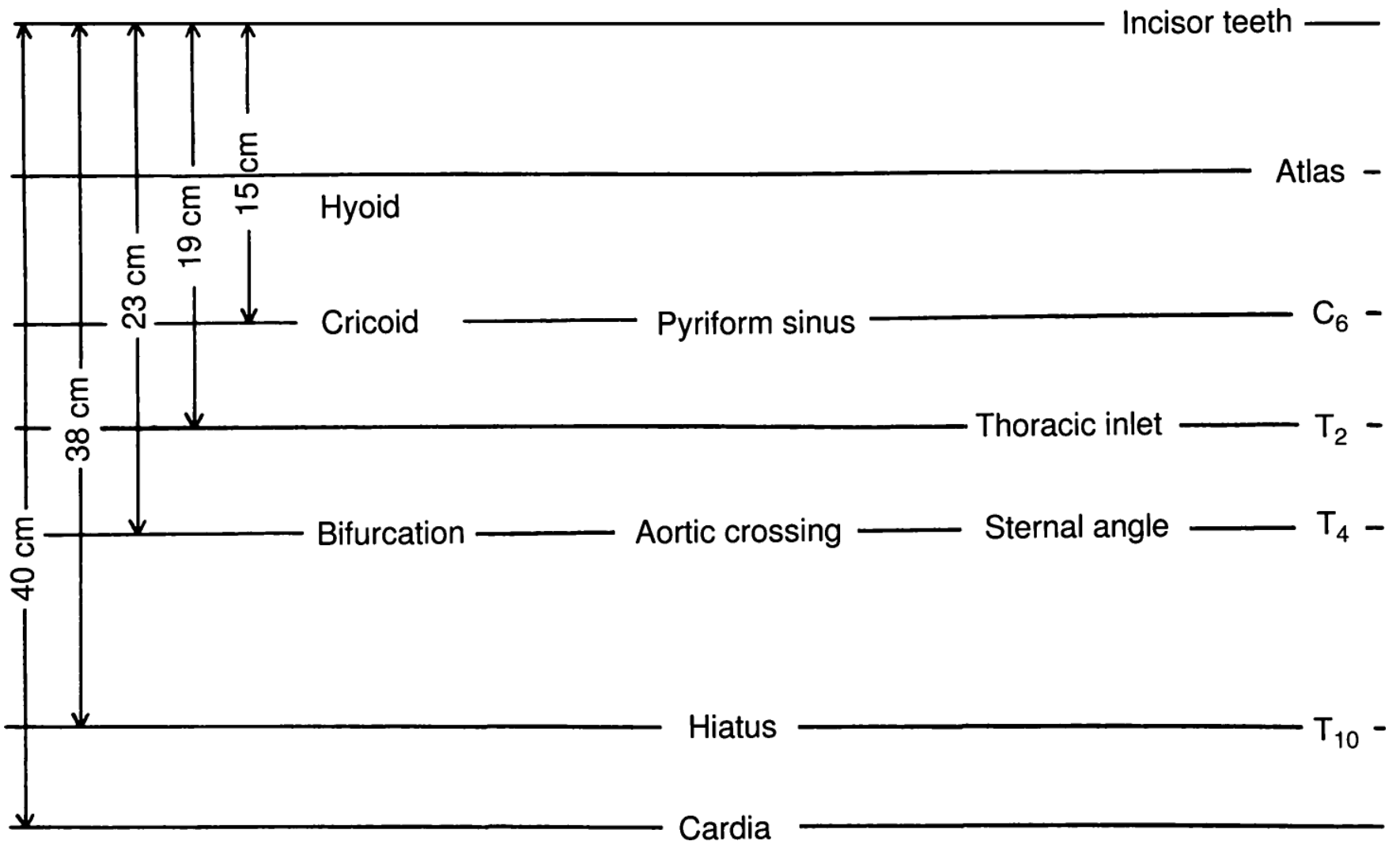
| Landmark | Distance from Incisor Teeth |
|---|---|
| Hyoid | 15 cm |
| Cricoid / Cricopharynx (UOS) | 19-23 cm |
| Thoracic inlet | 38 cm |
| Aortic arch / Tracheal bifurcation | 40 cm |
| Oesophageal hiatus | T10 |
Most common perforation site: the cricopharynx (Killian's dehiscence)
Killian's dehiscence (Killian's triangle / Laimer's triangle) is a triangular zone of muscular weakness in the posterior hypopharyngeal wall between the oblique fibres of the inferior constrictor and the horizontal fibres of the cricopharyngeus muscle. It represents the weakest point and the commonest site of iatrogenic perforation.
A. OESOPHAGEAL PERFORATION (Most Important Complication)
Causes / Predisposing Factors
RISK FACTORS FOR PERFORATION
│
├── Instrument-related
│ ├── Blind advancement of scope
│ ├── Excessive force at cricopharynx
│ └── Too large a scope for lumen
│
├── Patient-related
│ ├── Cervical osteophytes
│ ├── Prominent cricopharyngeal bar
│ ├── Foreign body (especially sharp, impacted)
│ ├── Pre-existing stricture
│ ├── Zenker's pharyngeal pouch
│ └── Malignancy thinning the wall
│
├── Procedural
│ ├── Attempted dilation of tight stricture
│ ├── Location: middle/distal oesophagus
│ │ (OR 4.67× higher than proximal - Alexandre et al. 2024)
│ └── Previous failed endoscopic attempt
│
└── Operator-related
├── Inexperienced surgeon
└── Inadequate anaesthesia / patient movement
Sites of Perforation (in order of frequency)
- Posterior pharyngeal wall / Killian's dehiscence - most common (cervical perforation)
- Cricopharyngeal region (C5-C6 level)
- Middle thoracic oesophagus - at the level of the aortic arch
- Lower thoracic oesophagus - at the diaphragmatic hiatus
As noted in Fishman's Pulmonary Diseases: "Instrumental perforation of the esophagus most frequently is localized to the cervical esophagus, whereas Boerhaave syndrome usually results in perforation of the distal thoracic and abdominal esophagus."
Clinical Features of Oesophageal Perforation
Mackler's Triad (classical presentation):
- Vomiting
- Chest pain
- Subcutaneous emphysema
Additional signs:
- Persistent chest/epigastric pain hours after procedure
- Fever, tachycardia, tachypnoea (signs of mediastinitis)
- Dyspnea and cyanosis
- Cervical subcutaneous emphysema at the suprasternal notch
- Dysphagia, odynophagia
- Shock (in advanced cases)
Murray & Nadel's (p.2293) note: "When the esophagus is perforated during esophagoscopy, the endoscopist generally does not realize it; however, the patients usually develop persistent chest or epigastric pain within a few hours after the procedure."
B. MEDIASTINITIS (Most Dangerous Sequela)
Oesophageal perforation leads to contamination of the mediastinum by oropharyngeal flora, producing acute mediastinitis.
CT Scan showing post-emetic esophageal rupture with mediastinal air:

CT scan showing extensive air surrounding the lower oesophagus with bilateral loculated effusions and left lower lobe atelectasis. - Fishman's Pulmonary Diseases
Pathophysiology of Mediastinitis
OESOPHAGEAL PERFORATION
│
↓
Oropharyngeal flora + food particles enter mediastinum
│
↓
Bacterial contamination (polymicrobial: Streptococcus,
Staphylococcus, anaerobes, gram-negatives)
│
↓
Acute mediastinitis
│ │
↓ ↓
Pleural effusion Mediastinal abscess
(usually LEFT sided) │
│ ↓
↓ Septicaemia / SIRS
Empyema thoracis
│
↓
Multi-organ failure / Death
- Pleural effusion occurs in ~60% of oesophageal perforations (usually left-sided)
- Pneumothorax in ~25%
- Mortality: 30-60% if untreated; <10% if repaired within 24 hours; rises steeply after 24 hours
C. ANAESTHESIA-RELATED COMPLICATIONS
| Complication | Mechanism | Management |
|---|---|---|
| Laryngospasm | Reflex stimulation during intubation/scope insertion | Propofol, succinylcholine, 100% O2 |
| Bronchospasm | Vagal stimulation | Bronchodilators, deepen anaesthesia |
| Aspiration pneumonitis | Pre-existing full stomach / regurgitation | Pre-op fasting, RSI, cricoid pressure |
| Cardiorespiratory depression | Anaesthetic agents | Monitoring, airway support |
| Arrhythmias | Vagal stimulation at cricopharynx | Atropine, ECG monitoring |
D. DIRECT MECHANICAL COMPLICATIONS
1. Mucosal Laceration (38.9% - most common minor complication)
- Superficial tears of the mucosa
- Usually self-limiting
- Managed conservatively: nil oral, antibiotics if extensive
2. Haemorrhage / Bleeding Haematoma (9.3%)
- From mucosal tears, biopsy sites, or vascular injury
- Rarely life-threatening
- More dangerous if eroding into great vessels (aorta - rare but fatal)
3. Dental and Oropharyngeal Trauma
- Dental avulsion (1.9%) - especially with poor dentition
- Lip, tongue, palatal laceration from scope insertion
- Prevention: dental guard, careful technique
4. Laryngeal Oedema
- Especially in children (narrow airway)
- May require racemic epinephrine nebulisation, IV dexamethasone (0.5-1 mg/kg)
- Rarely: tracheostomy
5. Pyriform Sinus Perforation
- Scope entering the pyriform fossa instead of oesophageal inlet
- Produces cervical emphysema
- Usually managed conservatively
E. FLOWCHART: MANAGEMENT OF SUSPECTED PERFORATION POST-OESOPHAGOSCOPY
Patient with post-procedure chest pain, fever,
subcutaneous emphysema, or crepitus
│
↓
STOP ORAL FEEDS
IV antibiotics (broad-spectrum + anaerobic cover)
│
↓
Chest X-ray + Lateral neck X-ray
(Look for: mediastinal widening,
pneumomediastinum, cervical air,
pleural effusion, pneumothorax)
│
┌──────┴──────┐
CXR+ve CXR-ve but suspicion HIGH
│ │
↓ ↓
CT Chest/Neck Gastrografin swallow
with contrast (water-soluble first)
│ │
│ If negative → Barium swallow
│ │
└──────────────┬──────┘
↓
PERFORATION CONFIRMED?
┌───────────┴───────────┐
YES NO
│ │
↓ Observe, NBM,
SIZE OF PERFORATION IV Ab
TIMING? LOCATION?
│
┌────┴─────────────────┐
│ │
< 24 hrs, contained > 24 hrs /
cervical perforation thoracic / large
│ │
↓ ↓
Conservative / SURGERY:
Endoscopic stent - Primary repair + drainage
(if suitable) - Cervical: transcervical
- Thoracic: left thoracotomy
- Wide mediastinal drainage
- Broad-spectrum antibiotics
- Nutritional support (TPN/NGT)
± Oesophagectomy (destroyed oes.)
F. LATE / CHRONIC COMPLICATIONS
| Complication | Cause | Management |
|---|---|---|
| Oesophageal stricture | Mucosal burns, repeated trauma, healing by fibrosis | Serial dilatation, stenting |
| Tracheo-oesophageal fistula | Unrecognised full-thickness perforation | Surgical repair, muscle flap interposition |
| Pharyngeal / cervical abscess | Contained perforation with infection | Drainage + antibiotics |
| Recurrent aspiration | Post-procedural dysmotility | Swallowing therapy |
G. DIAGNOSIS OF PERFORATION - INVESTIGATIONS
| Investigation | Finding | Significance |
|---|---|---|
| CXR (erect) | Mediastinal widening, pneumomediastinum, pleural effusion, pneumothorax | First-line screening |
| Lateral neck X-ray | Retropharyngeal air, prevertebral soft tissue widening | Cervical perforation |
| Gastrografin swallow | Extravasation of contrast | First-line contrast study (10% false negative) |
| Barium swallow | If Gastrografin negative but suspicion remains | More sensitive, but barium toxic if extravasated |
| CT chest/neck | Air in mediastinum, fluid collections, perforation site | Most sensitive - "gold standard" |
| Pleural fluid analysis | Elevated amylase, pH <7.0, squamous cells, polymicrobial | Strongly suggestive |
| Flexible oesophagoscopy | Mucosal tear visualised | Adjunct - may miss cricopharyngeal tears |
Key point from Cummings: "Several authors have reported a missed perforation near the cricopharyngeus as well as the hypopharynx, where flexible endoscopy is least satisfactory owing to mucosa redundancy."
Key point from Murray & Nadel: "The best screening test for esophageal rupture appears to be the level of amylase in the pleural fluid."
H. FLOWCHART: PREVENTION OF COMPLICATIONS
PRE-OPERATIVE
├── Proper patient selection
├── Correct anaesthetic (GA, muscle relaxation)
├── Review imaging (barium swallow, CT neck/chest)
├── Know the anatomy - narrowings & distances
├── Informed consent (perforation risk explained)
└── Dental guard preparation
INTRA-OPERATIVE
├── Correct Boyce-Jackson position (neck flexed,
│ mouth opened, axes aligned)
├── Never advance scope blindly
├── Adequate lubrication
├── Correct scope size (adult: 9×50 mm;
│ child: 5-6×35 mm)
├── Proximal FB → easier; distal FB → higher risk
├── Do NOT pass scope beyond area of injury
│ (especially in caustic ingestion / button battery)
└── Gentle manipulation, avoid excess force
POST-OPERATIVE
├── Post-op CXR if difficult procedure
├── Monitor: fever, tachycardia, tachypnoea,
│ chest pain, crepitus
├── IV dexamethasone if mucosal oedema
├── Antibiotics only if significant injury
└── Clinic review to ensure symptom resolution
I. SPECIAL SITUATIONS
Foreign Body-Related Complications
- Button battery is a special emergency - generates hydroxide ions by electrical current, causing liquefactive necrosis within 2 hours; scope must NOT be advanced beyond an area of battery injury (Cummings)
- Fish bones / sharp foreign bodies carry higher perforation risk
- Impacted meat - enzyme-based dissolution (e.g., papain) is absolutely CONTRAINDICATED - causes oesophageal necrosis and mediastinitis
Zenker's Diverticulum Risk
A large pharyngeal pouch represents a particular danger zone. The scope can inadvertently enter the pouch (which has a thin, easily perforated wall) instead of the oesophageal lumen. This is a well-described cause of perforation.
J. RECENT ADVANCES (RGUHS CONTEXT)
-
Flexible vs. Rigid debate - The UK trend (Scott-Brown's) is to discourage rigid oesophagoscopy of the lower third owing to higher perforation risk; flexible oesophagoscopy and transnasal oesophagoscopy (TNO) have largely replaced rigid techniques for lower oesophageal pathology.
-
Endoscopic stenting for perforation - Covered self-expanding metal/plastic stents (SEMS/SEPS) are now a widely accepted treatment for contained oesophageal perforation, avoiding open surgery in selected cases. Higher failure rate for cervical perforations and those >6 cm (Fishman's).
-
Minimally invasive drainage - Image-guided percutaneous drainage of mediastinal collections reduces the need for thoracotomy in stable patients.
-
Button battery ingestion protocols - "Stat red" urgent removal protocols; sucralfate/honey administration en route to prevent burns.
-
Transnasal oesophagoscopy (TNO) - Avoids GA-related risks; lower complication profile; cost-effective alternative for assessment of dysphagia (Scott-Brown's, Chapter 79).
-
Cryoprobe use - New technique for removing foreign bodies embedded in granulation tissue (Cummings, 2024 edition).
-
AI-assisted image analysis - Emerging use of artificial intelligence to detect mucosal injuries and guide real-time decision-making during endoscopy.
SUMMARY TABLE (Quick Revision)
| Complication | Frequency | Key Feature | Management |
|---|---|---|---|
| Mucosal laceration | 38.9% (most common) | Minor, superficial | Conservative, NBM |
| Bleeding/haematoma | 9.3% | Usually self-limiting | Observation; rarely surgery |
| Oesophageal perforation | 8% | Most serious | Surgery/stent within 24 hrs |
| Abscess | 3.1% | Contained perforation | Drainage + antibiotics |
| Death | 2.5% | Mediastinitis, sepsis | Prevention key |
| Pneumothorax | 1.9% | Chest drain | Intercostal drainage |
| Pneumomediastinum | 1.9% | Mediastinal air | Monitoring, antibiotics |
| Cervical emphysema | 1.2% | Crepitus at neck | NBM, antibiotics |
| Mediastinitis | 1.2% | Life-threatening | Urgent surgery |
| Dental avulsion | 1.9% | Tooth damage | Dental review |
REFERENCES
- Cummings Otolaryngology Head and Neck Surgery (7th ed.) - Chapter 211: Aerodigestive Foreign Bodies; Complications pp. 3966-3974
- Scott-Brown's Otorhinolaryngology, Head & Neck Surgery (8th ed.) - Chapter on Direct Pharyngo-oesophagoscopy and Transnasal Oesophagoscopy, pp. 2047-2088
- K.J. Lee's Essential Otolaryngology (11th ed.) - Esophagoscopy landmarks, p. 184
- Fishman's Pulmonary Diseases and Disorders - Mediastinitis from Esophageal Perforation, pp. 3949-3959
- Murray & Nadel's Textbook of Respiratory Medicine - Esophageal Perforation, pp. 2280-2297
- Dhingra's Diseases of Ear, Nose and Throat - Oesophagoscopy and complications (standard Indian ENT textbook reference)
- Hazarika's ENT Head and Neck Surgery - Complications of rigid oesophagoscopy (standard RGUHS reference)
- Stell & Maran's Head and Neck Surgery - Endoscopy of the upper aerodigestive tract (standard reference)
- Alexandre PL et al. "Rigid Esophagoscopy for Foreign Body Extraction: Results and Complications in the Endoscopic Era." Cureus 2024; [PMID: 38410347] - prospective data on complication rates in 162 patients
RGUHS Exam Tip: The RGUHS 20-mark answer expects: definition + classification + detailed description of each complication (especially perforation and mediastinitis) + diagrams + flowcharts for management + recent advances. The most heavily tested complication is oesophageal perforation with mediastinitis, and the most tested landmark is Killian's dehiscence as the commonest perforation site. Always mention the time-critical nature: mortality is <10% if repaired within 24 hours but rises sharply after that.
This is a shared conversation. Sign in to Orris to start your own chat.