Explain the recent Updates in Heart failure management According to AHA 2026 guidelines
AHA 2026 heart failure guidelines updates
https://newsroom.heart.org/news/global-experts-update-heart-…
"heart failure" AND guidelines
https://www.youtube.com/watch?v=ibEQhMPKRjo
"heart failure" AND "SGLT2" AND management
2026 second universal definition heart failure new classification LVEF stages staging treatment
"heart failure" AND "universal definition" AND classification
Recent Updates in Heart Failure Management - AHA/ACC/ESC 2026
Important note: This is an expert consensus/definition document, not a full clinical practice guideline. The full AHA/ACC Heart Failure Guideline is expected in late 2027.
1. New Classification of HF by Ejection Fraction
| Category | Definition |
|---|---|
| HF with Reduced EF (HFrEF) | Reduced LVEF (below sex/age/ethnicity-adjusted normal) |
| HF with Preserved EF (HFpEF) | Normal or near-normal LVEF |
| HF with Improved EF (HFimpEF) | Previously reduced LVEF that has increased or normalized |
2. Reaffirmed and Refined Disease Staging (with Stage 0)
| Stage | Description |
|---|---|
| Stage 0 | No risk factors (new addition) |
| Stage A | At risk for HF - risk factors present (hypertension, obesity, T2DM, etc.) but no structural changes, symptoms, or biomarker elevation |
| Stage B | Pre-HF - structural abnormalities, abnormal cardiac function, OR elevated biomarkers, but no symptoms |
| Stage C | Symptomatic HF - structural cardiac abnormality + current or prior symptoms |
| Stage D | Advanced HF - severe symptoms at rest or minimal exertion, recurrent hospitalizations, refractory to guideline-directed medical therapy (GDMT) |
3. Universal Classification of HF Causes
- Infective cardiomyopathy: viral myocarditis, Chagas disease, HIV, Lyme disease
- Inflammatory cardiomyopathy: autoimmune, sarcoidosis, hypersensitivity, desmoplakin
- Ischemic cardiomyopathy: ischemic heart disease, MI, CAD
- Infiltrative cardiomyopathies: cardiac amyloidosis (ATTR and AL), Fabry disease
- Genetic/inherited: familial dilated cardiomyopathy, hypertrophic cardiomyopathy
- Other: toxin-mediated, peripartum, stress-induced (Takotsubo)
4. Therapeutic Shifts: From "Quadruple" to "Heart Function" Paradigm
HFrEF - Quadruple Therapy Becomes Standard
- ACE inhibitor / ARB / ARNI (sacubitril-valsartan preferred over ACE inhibitor)
- Beta-blocker (carvedilol, metoprolol succinate, bisoprolol)
- MRA (spironolactone or eplerenone - non-steroidal finerenone increasingly favored)
- SGLT2 inhibitor (dapagliflozin or empagliflozin)
SGLT2 Inhibitors - Pan-EF Indication
HFpEF - Triple Drug Evidence-Based Therapy
- SGLT2 inhibitors (dapagliflozin, empagliflozin): Class I evidence in HFpEF
- Non-steroidal MRA (finerenone): positive outcomes data in HFpEF
- GLP-1 receptor agonists (semaglutide, tirzepatide): emerging pivotal trial data showing CV outcomes benefit in HFpEF with obesity/T2DM - a major paradigm shift for the cardiometabolic HFpEF phenotype
HFmrEF - Now Evidence-Supported
5. Geographic Variation in HF
6. HF Trajectories: Remission and Recovery
- Improvement (partial recovery of function)
- Remission (symptoms resolved but disease present)
- Recovery (near-complete normalization - previously called HFimpEF)
7. Related 2026 Scientific Statements
- "Strategies for Optimizing Heart Failure Care in the Older Adult" (June 2026) - addressing frailty, polypharmacy, and goals-of-care in elderly HF
- "Risk-Based Primary Prevention of Heart Failure" (March 2025) - a framework for identifying and treating Stage A patients before structural disease develops
Summary Table: What Changed in 2026
| Domain | Before (2022 Guidelines) | 2026 Update |
|---|---|---|
| LVEF classification | HFrEF ≤40%, HFmrEF 41-49%, HFpEF ≥50% | Reduced, Preserved, Improved EF - sex/age/ethnicity adjusted |
| Staging | Stage A-D | Stage 0 added; refined descriptions |
| HFrEF treatment | Quadruple therapy recommended | Quadruple therapy standard; simultaneous initiation emphasized |
| HFpEF treatment | Diuretics only (symptomatic) | SGLT2i + non-steroidal MRA + GLP-1 agonists |
| Etiology classification | Not standardized | Universal etiologic taxonomy proposed |
| Geographic variation | Not addressed | Formally incorporated |
| Disease trajectory | Static framing | Remission / Recovery / Improvement recognized |
Search for clinical images and ECG patterns of HFpEF vs HFrEF
HFpEF vs HFrEF ECG patterns clinical imaging echocardiogram comparison 2024 2025
HFrEF ECG left bundle branch block LVH dilated cardiomyopathy ECG findings site:litfl.com OR site:ecgwaves.com
HFpEF echocardiogram concentric hypertrophy diastolic dysfunction Doppler E/e ratio image
Clinical Images & ECG Patterns: HFpEF vs HFrEF
Overview: Key Distinguishing Features
| Feature | HFrEF | HFpEF |
|---|---|---|
| LVEF | ≤40% | ≥50% (2026: sex/age adjusted) |
| LV size | Dilated (eccentric hypertrophy) | Normal/small (concentric hypertrophy) |
| LV wall | Thin or normal | Thickened |
| Primary dysfunction | Systolic (pump failure) | Diastolic (relaxation/filling failure) |
| ECG hallmark | LBBB, LVH with strain, pseudoinfarction Q waves | LVH strain pattern, AF, low QRS voltage (amyloid) |
| Typical patient | Male, post-MI, younger | Female, elderly, hypertensive, obese |
ECG Patterns
HFrEF (Dilated Cardiomyopathy) ECG
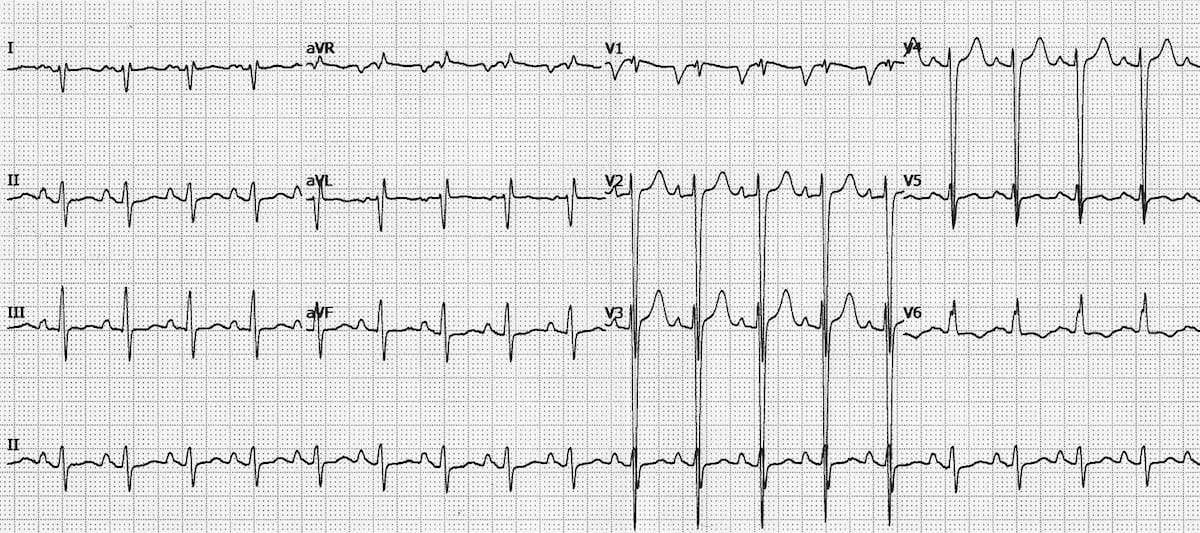
- Left Bundle Branch Block (LBBB) - broad, notched R waves in I, aVL, V5-V6; deep S in V1 - present in ~25-30% of HFrEF patients
- Pseudoinfarction Q waves - abnormal Q waves in V1-V4 mimicking anterior MI (no culprit artery)
- Left atrial enlargement - deep, wide terminal portion of P wave in V1; leftward P-axis deviation
- Biventricular hypertrophy - high QRS voltages in precordial leads (V4-V6) with relatively low limb lead voltages
- Lateral ST-T changes - downsloping ST depression and T-wave inversion in I, aVL, V5-V6 due to strain
Clinical note: No ECG pattern is specific to DCM/HFrEF. However, a completely normal ECG has a very high negative predictive value for significant LV systolic dysfunction (NPV ~98%).
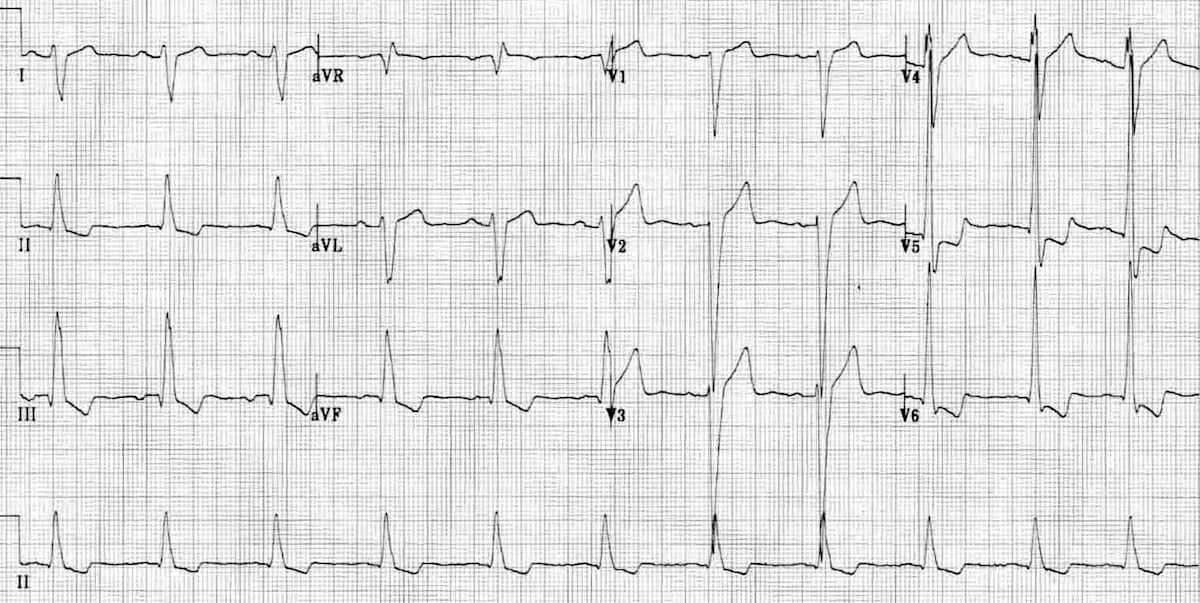
HFpEF ECG Patterns
- Sokolow-Lyon criteria positive: S(V1) + R(V5/V6) > 35 mm
- Cornell criteria: R(aVL) + S(V3) > 28 mm (men), >20 mm (women)
- LVH strain pattern: downsloping ST depression + T-wave inversion in lateral leads (I, aVL, V5, V6) - reflects concentric LV hypertrophy from long-standing hypertension
Echocardiographic Findings (the diagnostic cornerstone)
HFpEF Echocardiography - Doppler Parameters
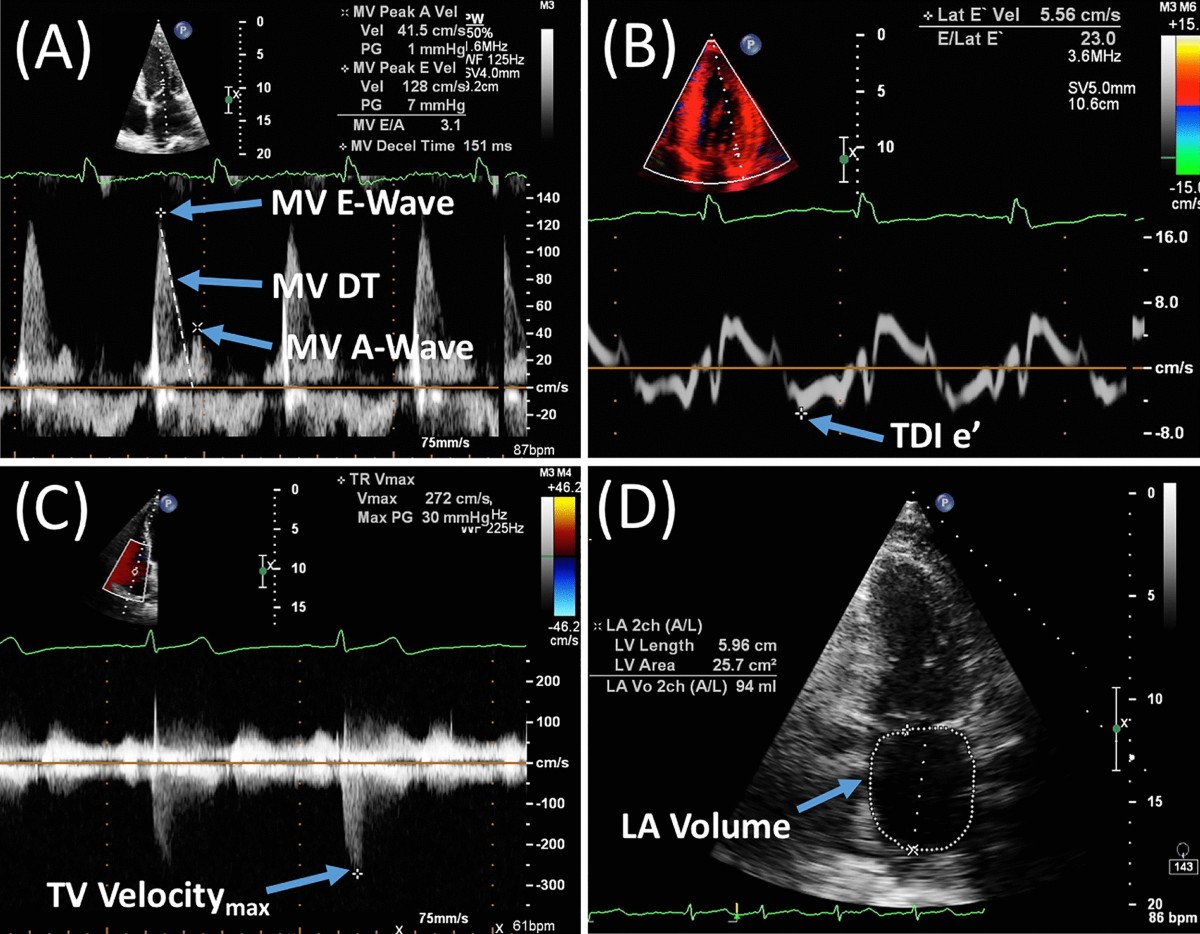
- (A) MV E/A ratio - In HFpEF with impaired relaxation (Grade I): E/A < 1 (A-wave dominant). In severe diastolic dysfunction (Grade III): E/A > 2 (restrictive filling - very elevated filling pressures)
- (B) TDI e' (tissue Doppler e' velocity) - Reduced e' (septal <7 cm/s, lateral <10 cm/s) reflects impaired myocardial relaxation. E/e' ratio >14 indicates elevated LV filling pressures
- (C) TR Vmax - Elevated tricuspid regurgitation velocity (>2.8 m/s) indicates pulmonary hypertension from elevated LA pressure
- (D) LA volume index - Enlarged LA (>34 mL/m²) reflects chronically elevated LV filling pressures
Grades of Diastolic Dysfunction (HFpEF Spectrum)
| Grade | E/A | e' | E/e' | LVEDP |
|---|---|---|---|---|
| Grade I (impaired relaxation) | <1.0 | Low | ≤14 | Normal |
| Grade II (pseudonormal) | 1.0-2.0 | Low | >14 | Elevated |
| Grade III (restrictive) | >2.0 | Low | >14 | Severely elevated |
HFrEF vs HFpEF Echo: Structural Comparison
| Echo Parameter | HFrEF | HFpEF |
|---|---|---|
| LVEF | ≤40% | ≥50% |
| LV cavity | Dilated (LVEDV increased) | Normal/small |
| LV geometry | Eccentric hypertrophy (↑LV mass, normal RWT) | Concentric hypertrophy (↑LV mass, ↑RWT) |
| Wall thickness | Normal/thin | Increased (>12 mm) |
| Systolic function (GLS) | Severely reduced global longitudinal strain | Mildly reduced GLS (subclinical) |
| Mitral annular excursion (MAPSE) | Very reduced | Mildly reduced or normal |
| Diastolic function | Restrictive pattern common (Grade III) | Impaired relaxation (Grade I-II) |
| LA size | Dilated | Dilated (secondary to elevated filling pressures) |
| RV | Often dilated (volume overload) | May be dilated (atrial secondary TR in HFpEF) |
HFrEF Treatment Algorithm (from Goldman-Cecil Medicine)
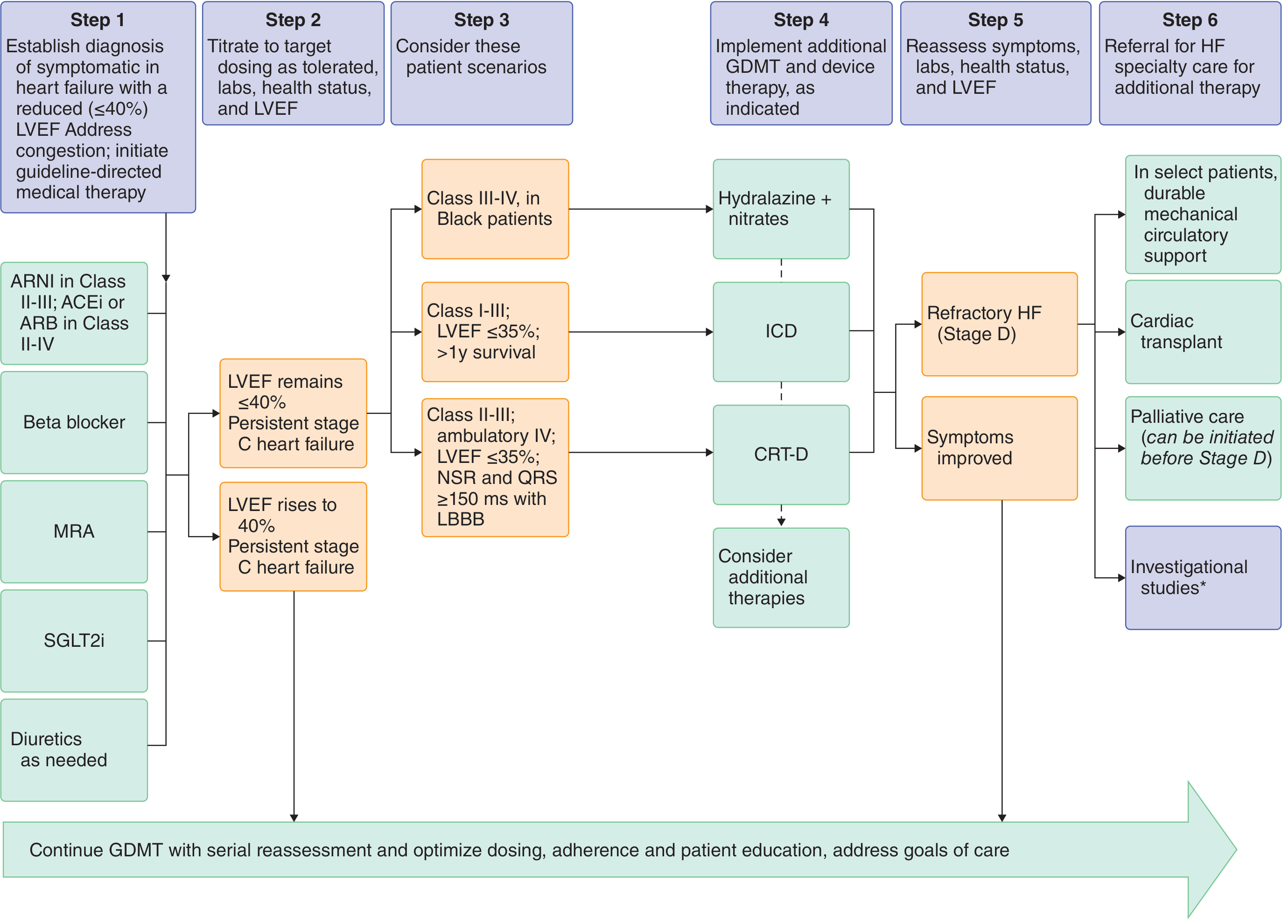
- CRT-D is indicated for HFrEF with LVEF ≤35% + LBBB on ECG (QRS ≥150 ms) + NSR + NYHA Class II-III (ambulatory IV)
- ICD is indicated for LVEF ≤35% + NYHA Class I-III with >1 year expected survival
- LBBB on ECG in a patient with HFrEF is therefore not just a diagnostic finding - it directly triggers a device therapy decision
HFpEF Diagnostic Algorithm (HFA-PEFF)
- ECG: LVH criteria, AF, low voltage
- Labs: BNP ≥35 pg/mL or NT-proBNP ≥125 pg/mL (in sinus rhythm)
- Septal e' <7 cm/s OR lateral e' <10 cm/s
- E/e' ratio >15
- LA volume index >34 mL/m²
- LV mass index >149 g/m² (men) or >122 g/m² (women)
- TR velocity >2.8 m/s (PASP >35 mmHg)
- NT-proBNP >220 pg/mL (sinus) or >660 pg/mL (AF)
Clinical Summary: Pattern Recognition
| Clinical Clue | Think HFrEF | Think HFpEF |
|---|---|---|
| Age/Sex | Younger males | Older females |
| History | Post-MI, DCM, chemotherapy | Hypertension, obesity, DM, AF |
| ECG | LBBB, pseudoinfarction Q waves | LVH strain, AF, low voltage |
| Echo | Dilated LV, EF <40%, eccentric hypertrophy | Normal EF, thick walls, diastolic dysfunction |
| BNP | Very high (proportional to degree of dysfunction) | Elevated but lower (may be "diluted" in obese) |
| Response to diuretics | Dramatic symptomatic improvement | Narrow therapeutic window - easily overdiuresed |
| Chest X-ray | Cardiomegaly + pulmonary vascular congestion | Variable - may show minimal cardiomegaly |