Write university like handwritten notes on urinary bladder for anatomy with clinical applied
ls /home/daytona/workspace/ 2>/dev/null || mkdir -p /home/daytona/workspace/
mkdir -p /home/daytona/workspace/bladder-notes && ls /home/daytona/workspace/bla…
~/bladder-notes/create_notes.js
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = 'LAYOUT_WIDE'; // 13.3" x 7.5"
pres.title = 'Urinary Bladder - Anatomy Notes';
pres.author = 'University Anatomy Notes';
// ─── Color Palette (Handwritten notebook feel) ───────────────────────────────
const BG = "FFFDF4"; // warm cream paper
const INK = "1A1A2E"; // deep navy ink
const HEADING = "1B4F72"; // blue heading (like colored marker)
const RED = "C0392B"; // red ink for important points
const GREEN = "1E8449"; // green for clinical notes
const PURPLE = "6C3483"; // purple for mnemonics
const ORANGE = "D35400"; // orange for embryology
const LIGHT_BG = "EBF5FB"; // light blue boxes
const GREEN_BG = "EAFAF1"; // light green boxes
const RED_BG = "FDEDEC"; // light red for clinical
const RULED = "D6EAF8"; // ruled line color
// ─── Helper: ruled-line background ─────────────────────────────────────────
function addRuledBg(slide) {
slide.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 13.3, h: 7.5, fill: { color: BG }, line: { color: BG } });
// Horizontal rules
for (let y = 0.9; y < 7.5; y += 0.34) {
slide.addShape(pres.ShapeType.line, { x: 0.3, y, w: 12.7, h: 0, line: { color: RULED, width: 0.5, dashType: 'solid' } });
}
// Left red margin line
slide.addShape(pres.ShapeType.line, { x: 1.1, y: 0.3, w: 0, h: 7.0, line: { color: "F1948A", width: 1.2 } });
}
function slideHeader(slide, title, subtitle) {
slide.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 13.3, h: 0.62, fill: { color: HEADING }, line: { color: HEADING } });
slide.addText(title, { x: 0.15, y: 0.08, w: 9, h: 0.48, fontSize: 20, fontFace: 'Patrick Hand SC', bold: true, color: 'FFFFFF', margin: 0 });
if (subtitle) {
slide.addText(subtitle, { x: 9.2, y: 0.1, w: 3.9, h: 0.42, fontSize: 11, fontFace: 'Patrick Hand SC', color: 'D6EEF8', align: 'right', margin: 0 });
}
}
function box(slide, x, y, w, h, fillColor, borderColor, text, textOptions) {
slide.addShape(pres.ShapeType.roundRect, { x, y, w, h, fill: { color: fillColor }, line: { color: borderColor, width: 1 }, rectRadius: 0.07 });
if (text) {
slide.addText(text, { x: x + 0.08, y: y + 0.04, w: w - 0.16, h: h - 0.08, ...textOptions });
}
}
// ─── SLIDE 1: Title ──────────────────────────────────────────────────────────
{
const sl = pres.addSlide();
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 13.3, h: 7.5, fill: { color: "0D2137" }, line: { color: "0D2137" } });
// decorative ruled lines
for (let i = 0; i < 14; i++) {
sl.addShape(pres.ShapeType.line, { x: 0, y: 0.5 + i * 0.52, w: 13.3, h: 0, line: { color: "1B3A55", width: 0.6 } });
}
sl.addShape(pres.ShapeType.rect, { x: 0.5, y: 0.9, w: 12.3, h: 5.7, fill: { color: "FFFDF4", transparency: 5 }, line: { color: "A9CCE3", width: 1.5 } });
sl.addShape(pres.ShapeType.line, { x: 1.6, y: 0.9, w: 0, h: 5.7, line: { color: "F1948A", width: 1.5 } });
sl.addText("URINARY BLADDER", { x: 2, y: 1.4, w: 10, h: 1.0, fontSize: 48, bold: true, color: INK, fontFace: 'Patrick Hand SC', align: 'center' });
sl.addText("Anatomy with Clinical Applications", { x: 2, y: 2.55, w: 10, h: 0.55, fontSize: 22, color: HEADING, fontFace: 'Patrick Hand SC', align: 'center', italic: true });
sl.addShape(pres.ShapeType.line, { x: 2.5, y: 3.2, w: 8.3, h: 0, line: { color: RED, width: 1.5 } });
sl.addText([
{ text: "Topics: ", options: { bold: true, color: RED } },
{ text: "Position & Parts • Relations • Interior • Histology • Blood Supply\nInnervation • Lymphatics • Micturition • Embryology • Clinical Notes", options: { color: INK } }
], { x: 2, y: 3.4, w: 9.5, h: 1.3, fontSize: 14, fontFace: 'Patrick Hand SC', align: 'center' });
sl.addText("✏ University Anatomy Notes | Date: _______________ | Subject: Human Anatomy", {
x: 0.6, y: 6.75, w: 12, h: 0.45, fontSize: 11, color: "7F8C8D", fontFace: 'Patrick Hand SC', align: 'center'
});
}
// ─── SLIDE 2: Introduction & Position ────────────────────────────────────────
{
const sl = pres.addSlide();
addRuledBg(sl);
slideHeader(sl, "1. INTRODUCTION & POSITION", "Urinary Bladder | Anatomy");
// Left column
sl.addText("Definition & Basic Facts", { x: 1.2, y: 0.75, w: 5.5, h: 0.35, fontSize: 14, bold: true, color: HEADING, fontFace: 'Patrick Hand SC', underline: true });
sl.addText([
{ text: "• ", options: { color: RED, bold: true } }, { text: "Hollow, muscular, distensible reservoir for urine\n", options: { color: INK } },
{ text: "• ", options: { color: RED, bold: true } }, { text: "Located in the lesser pelvis, posterior to pubic symphysis\n", options: { color: INK } },
{ text: "• ", options: { color: RED, bold: true } }, { text: "Capacity: ~", options: { color: INK } }, { text: "500 mL", options: { color: RED, bold: true } }, { text: " (urge to void at ~300 mL)\n", options: { color: INK } },
{ text: "• ", options: { color: RED, bold: true } }, { text: "Shape varies: EMPTY = pyramidal; FULL = ovoid\n", options: { color: INK } },
{ text: "• ", options: { color: RED, bold: true } }, { text: "When full, apex rises above pubic symphysis into abdomen\n", options: { color: INK } },
], { x: 1.2, y: 1.12, w: 5.6, h: 1.8, fontSize: 12, fontFace: 'Patrick Hand SC', lineSpacingMultiple: 1.3 });
sl.addText("Parts of Urinary Bladder", { x: 1.2, y: 3.0, w: 5.5, h: 0.35, fontSize: 14, bold: true, color: HEADING, fontFace: 'Patrick Hand SC', underline: true });
const parts = [
{ label: "APEX", desc: "Anterosuperior; attached to median umbilical ligament (obliterated urachus) → umbilicus", col: ORANGE },
{ label: "BODY", desc: "Main bulk of organ; bounded by superior + 2 inferolateral surfaces", col: HEADING },
{ label: "FUNDUS (Base)", desc: "Posterior; receives 2 ureters; related to seminal vesicles (M) / uterus/vagina (F)", col: PURPLE },
{ label: "NECK", desc: "Inferiormost; continuous with urethra; most fixed part; rests on prostate (M) / UG diaphragm (F)", col: RED },
];
parts.forEach((p, i) => {
box(sl, 1.2, 3.45 + i * 0.82, 5.6, 0.74, i % 2 === 0 ? LIGHT_BG : "FEF9E7", p.col, null, {});
sl.addText(p.label, { x: 1.3, y: 3.5 + i * 0.82, w: 1.5, h: 0.64, fontSize: 11, bold: true, color: p.col, fontFace: 'Patrick Hand SC', valign: 'middle' });
sl.addText(p.desc, { x: 2.85, y: 3.5 + i * 0.82, w: 4.0, h: 0.64, fontSize: 10.5, color: INK, fontFace: 'Patrick Hand SC', valign: 'middle', wrap: true });
});
// Right column: Gender differences box
sl.addText("Position by Gender & Age", { x: 7.3, y: 0.75, w: 5.6, h: 0.35, fontSize: 14, bold: true, color: HEADING, fontFace: 'Patrick Hand SC', underline: true });
box(sl, 7.3, 1.12, 5.6, 1.4, LIGHT_BG, HEADING, null, {});
sl.addText("MALE RELATIONS (posterior)", { x: 7.4, y: 1.18, w: 5.4, h: 0.28, fontSize: 11, bold: true, color: HEADING, fontFace: 'Patrick Hand SC' });
sl.addText([
{ text: "• Seminal vesicles, vas deferens (posterolateral)\n", options: { color: INK } },
{ text: "• Rectum (posterior, separated by rectovesical pouch)\n", options: { color: INK } },
{ text: "• Prostate gland (inferior to bladder neck)\n", options: { color: INK } },
], { x: 7.5, y: 1.5, w: 5.2, h: 1.0, fontSize: 11, fontFace: 'Patrick Hand SC', lineSpacingMultiple: 1.2 });
box(sl, 7.3, 2.6, 5.6, 1.3, GREEN_BG, GREEN, null, {});
sl.addText("FEMALE RELATIONS (posterior)", { x: 7.4, y: 2.66, w: 5.4, h: 0.28, fontSize: 11, bold: true, color: GREEN, fontFace: 'Patrick Hand SC' });
sl.addText([
{ text: "• Uterus (body) separated by vesicouterine pouch\n", options: { color: INK } },
{ text: "• Anterior vaginal wall (base of bladder sits on it)\n", options: { color: INK } },
{ text: "• Bladder neck: rests on perineal membrane / UG diaphragm\n", options: { color: INK } },
], { x: 7.5, y: 2.96, w: 5.2, h: 0.9, fontSize: 11, fontFace: 'Patrick Hand SC', lineSpacingMultiple: 1.2 });
box(sl, 7.3, 3.98, 5.6, 0.75, RED_BG, RED, null, {});
sl.addText("CHILDREN", { x: 7.4, y: 4.02, w: 5.4, h: 0.25, fontSize: 11, bold: true, color: RED, fontFace: 'Patrick Hand SC' });
sl.addText("Bladder is an abdominal organ even when empty (descends to pelvis after puberty ~6 yrs)", { x: 7.5, y: 4.3, w: 5.2, h: 0.4, fontSize: 10.5, color: INK, fontFace: 'Patrick Hand SC', wrap: true });
sl.addText("PERITONEAL RELATIONS:", { x: 7.3, y: 4.82, w: 5.6, h: 0.3, fontSize: 13, bold: true, color: HEADING, fontFace: 'Patrick Hand SC' });
sl.addText([
{ text: "✦ Superior surface → COVERED by peritoneum\n", options: { color: HEADING } },
{ text: "✦ Anterior & lateral walls → NO peritoneum (retropubic space of Retzius)\n", options: { color: INK } },
{ text: "✦ As bladder fills → peritoneum peels off anterior wall → safe suprapubic access\n", options: { color: GREEN, bold: true } },
], { x: 7.3, y: 5.15, w: 5.6, h: 1.1, fontSize: 11, fontFace: 'Patrick Hand SC', lineSpacingMultiple: 1.3 });
sl.addText("★ MOST FIXED PART = BLADDER NECK (prostate/UG diaphragm)", {
x: 1.2, y: 7.1, w: 11.5, h: 0.3, fontSize: 11, bold: true, color: RED, fontFace: 'Patrick Hand SC', align: 'center'
});
}
// ─── SLIDE 3: Interior & Histology ───────────────────────────────────────────
{
const sl = pres.addSlide();
addRuledBg(sl);
slideHeader(sl, "2. INTERIOR OF BLADDER & HISTOLOGY", "Urinary Bladder | Anatomy");
// Left: Interior
sl.addText("Interior of Bladder", { x: 1.2, y: 0.75, w: 5.5, h: 0.35, fontSize: 14, bold: true, color: HEADING, fontFace: 'Patrick Hand SC', underline: true });
sl.addText([
{ text: "Mucosa (empty): ", options: { bold: true, color: HEADING } }, { text: "thrown into irregular RUGAE / FOLDS → disappear when distended\n", options: { color: INK } },
{ text: "Mucosa (trigone): ", options: { bold: true, color: ORANGE } }, { text: "SMOOTH, no folds → firmly adherent to detrusor\n", options: { color: INK } },
], { x: 1.2, y: 1.15, w: 5.6, h: 0.85, fontSize: 12, fontFace: 'Patrick Hand SC', lineSpacingMultiple: 1.35 });
// Trigone box
box(sl, 1.2, 2.08, 5.6, 2.5, "FEF9E7", ORANGE, null, {});
sl.addText("TRIGONE OF BLADDER", { x: 1.35, y: 2.14, w: 5.3, h: 0.35, fontSize: 13, bold: true, color: ORANGE, fontFace: 'Patrick Hand SC' });
sl.addText([
{ text: "Triangular smooth area on the FLOOR / POSTERIOR WALL\n\n", options: { color: INK, bold: true } },
{ text: "Boundaries:\n", options: { bold: true, color: ORANGE } },
{ text: " • Superolateral angles (×2) = ", options: { color: INK } }, { text: "Ureteric orifices\n", options: { bold: true, color: HEADING } },
{ text: " • Inferior angle = ", options: { color: INK } }, { text: "Internal urethral orifice\n\n", options: { bold: true, color: HEADING } },
{ text: "Interureteric ridge (Mercier's bar) = ", options: { bold: true, color: PURPLE } }, { text: "transverse fold connecting ureteric orifices\n\n", options: { color: INK } },
{ text: "Uvula vesicae = ", options: { bold: true, color: RED } }, { text: "small elevation at internal urethral orifice in MALES (due to median lobe of prostate)\n\n", options: { color: INK } },
{ text: "Embryology: Trigone derived from MESONEPHRIC DUCT (mesoderm)\n", options: { color: ORANGE, italic: true } },
{ text: " → NO muscularis mucosae or submucosal layer!\n", options: { color: ORANGE, italic: true } },
{ text: "Rest of bladder derived from CLOACA (endoderm)\n", options: { color: ORANGE, italic: true } },
], { x: 1.35, y: 2.52, w: 5.3, h: 2.0, fontSize: 10.5, fontFace: 'Patrick Hand SC', lineSpacingMultiple: 1.2 });
sl.addText("Ureteric orifices open OBLIQUELY (antireflux mechanism!)", { x: 1.2, y: 4.65, w: 5.6, h: 0.3, fontSize: 11, bold: true, color: GREEN, fontFace: 'Patrick Hand SC' });
// Right: Histology layers
sl.addText("Histology / Layers of Bladder Wall", { x: 7.1, y: 0.75, w: 5.8, h: 0.35, fontSize: 14, bold: true, color: HEADING, fontFace: 'Patrick Hand SC', underline: true });
const layers = [
{ num: "1", name: "UROTHELIUM (Transitional Epithelium)", detail: "Lines entire interior; stratified; 4-6 cell layers when empty, 2-3 when distended. Barrier function against urine. Umbrella cells at surface.", col: HEADING, bg: LIGHT_BG },
{ num: "2", name: "LAMINA PROPRIA", detail: "Loose vascular connective tissue; contains muscularis mucosae (thin, variable). ABSENT in trigone.", col: PURPLE, bg: "F9F0FF" },
{ num: "3", name: "DETRUSOR MUSCLE", detail: "Three ill-defined smooth muscle layers: inner longitudinal, middle circular, outer longitudinal. At internal urethral orifice → forms INTERNAL SPHINCTER (involuntary).\n• Sympathetic (β₃): RELAXES detrusor\n• Parasympathetic (M3): CONTRACTS detrusor", col: GREEN, bg: GREEN_BG },
{ num: "4", name: "ADVENTITIA / SEROSA", detail: "Fibrofattite adventitia on most surfaces. PERITONEUM (serosa) only on superior surface & part of posterior surface above trigone.", col: ORANGE, bg: "FEF9E7" },
];
layers.forEach((l, i) => {
box(sl, 7.1, 1.15 + i * 1.52, 5.8, 1.42, l.bg, l.col, null, {});
sl.addText(l.num, { x: 7.18, y: 1.2 + i * 1.52, w: 0.38, h: 1.3, fontSize: 18, bold: true, color: l.col, fontFace: 'Patrick Hand SC', valign: 'middle', align: 'center' });
sl.addText(l.name, { x: 7.6, y: 1.22 + i * 1.52, w: 5.2, h: 0.32, fontSize: 11.5, bold: true, color: l.col, fontFace: 'Patrick Hand SC' });
sl.addText(l.detail, { x: 7.6, y: 1.56 + i * 1.52, w: 5.2, h: 1.0, fontSize: 10, color: INK, fontFace: 'Patrick Hand SC', wrap: true, lineSpacingMultiple: 1.15 });
});
// Footer note
sl.addText("★ Trigone = smooth & adherent (no rugae) → First site of tumor implantation / schistosomiasis calcification", {
x: 1.2, y: 7.05, w: 11.5, h: 0.35, fontSize: 10.5, bold: true, color: RED, fontFace: 'Patrick Hand SC', align: 'center'
});
}
// ─── SLIDE 4: Blood Supply & Lymphatics ──────────────────────────────────────
{
const sl = pres.addSlide();
addRuledBg(sl);
slideHeader(sl, "3. BLOOD SUPPLY & LYMPHATIC DRAINAGE", "Urinary Bladder | Anatomy");
// Arterial supply
sl.addText("Arterial Supply", { x: 1.2, y: 0.75, w: 5.5, h: 0.35, fontSize: 14, bold: true, color: RED, fontFace: 'Patrick Hand SC', underline: true });
const arteries = [
{ vessel: "Superior Vesical Artery (×2)", src: "Branch of umbilical artery → from internal iliac artery", supply: "Superior, anterior & lateral surfaces of bladder + upper ureter", col: RED },
{ vessel: "Inferior Vesical Artery (×2)", src: "Direct branch of anterior trunk of internal iliac artery (male)\nVaginal artery equivalent (female)", supply: "Base (fundus), neck of bladder, seminal vesicles, prostate (M) / upper vagina (F)", col: PURPLE },
{ vessel: "Middle Rectal Artery", src: "Branch of internal iliac", supply: "Minor contribution to bladder base", col: ORANGE },
{ vessel: "Obturator & Inferior Gluteal", src: "Internal iliac branches", supply: "Small accessory twigs to bladder", col: "7D6608" },
];
arteries.forEach((a, i) => {
box(sl, 1.2, 1.15 + i * 1.1, 5.7, 1.02, i % 2 === 0 ? RED_BG : "FDF2F8", a.col, null, {});
sl.addText(a.vessel, { x: 1.3, y: 1.18 + i * 1.1, w: 5.5, h: 0.3, fontSize: 11.5, bold: true, color: a.col, fontFace: 'Patrick Hand SC' });
sl.addText("Source: " + a.src, { x: 1.3, y: 1.5 + i * 1.1, w: 5.5, h: 0.3, fontSize: 10, color: HEADING, fontFace: 'Patrick Hand SC', wrap: true });
sl.addText("Supply: " + a.supply, { x: 1.3, y: 1.72 + i * 1.1, w: 5.5, h: 0.36, fontSize: 10, color: INK, fontFace: 'Patrick Hand SC', wrap: true });
});
sl.addText("All arterial supply from INTERNAL ILIAC ARTERY (anterior trunk)", {
x: 1.2, y: 5.6, w: 5.7, h: 0.3, fontSize: 11, bold: true, color: RED, fontFace: 'Patrick Hand SC', align: 'center'
});
sl.addText("Rich collateral network → ligation of single artery is NOT detrimental", {
x: 1.2, y: 5.9, w: 5.7, h: 0.3, fontSize: 10.5, color: GREEN, fontFace: 'Patrick Hand SC', align: 'center', italic: true
});
// Right: Venous & Lymphatics
sl.addText("Venous Drainage", { x: 7.2, y: 0.75, w: 5.8, h: 0.35, fontSize: 14, bold: true, color: HEADING, fontFace: 'Patrick Hand SC', underline: true });
box(sl, 7.2, 1.12, 5.8, 1.4, LIGHT_BG, HEADING, null, {});
sl.addText([
{ text: "Vesical venous plexus ", options: { bold: true, color: HEADING } }, { text: "→ surrounds fundus & base\n", options: { color: INK } },
{ text: "→ Drains into ", options: { color: INK } }, { text: "Internal Iliac Veins\n", options: { bold: true, color: RED } },
{ text: "Communicates with: Prostatic venous plexus (M) | Vaginal venous plexus (F)\n", options: { color: INK } },
{ text: "Also communicates with vertebral (Batson's) plexus → metastasis pathway!", options: { bold: true, color: RED } },
], { x: 7.3, y: 1.2, w: 5.6, h: 1.28, fontSize: 10.5, fontFace: 'Patrick Hand SC', lineSpacingMultiple: 1.3 });
sl.addText("Lymphatic Drainage", { x: 7.2, y: 2.62, w: 5.8, h: 0.35, fontSize: 14, bold: true, color: GREEN, fontFace: 'Patrick Hand SC', underline: true });
const lymph = [
{ from: "Superior & lateral wall", to: "External iliac nodes", col: GREEN },
{ from: "Fundus & Trigone (base)", to: "Internal iliac nodes", col: HEADING },
{ from: "Anterior wall", to: "Internal iliac nodes (via obturator/iliac)", col: PURPLE },
{ from: "All nodes → ultimately", to: "Para-aortic nodes (lateral aortic)", col: ORANGE },
];
box(sl, 7.2, 3.05, 5.8, 2.15, GREEN_BG, GREEN, null, {});
sl.addText("Region → Lymph Node", { x: 7.3, y: 3.1, w: 5.6, h: 0.28, fontSize: 11, bold: true, color: GREEN, fontFace: 'Patrick Hand SC' });
sl.addShape(pres.ShapeType.line, { x: 7.3, y: 3.4, w: 5.6, h: 0, line: { color: GREEN, width: 0.5 } });
lymph.forEach((l, i) => {
sl.addText(`${l.from} → `, { x: 7.35, y: 3.46 + i * 0.43, w: 3.1, h: 0.38, fontSize: 10.5, color: INK, fontFace: 'Patrick Hand SC', valign: 'middle' });
sl.addText(l.to, { x: 10.45, y: 3.46 + i * 0.43, w: 2.4, h: 0.38, fontSize: 10.5, bold: true, color: l.col, fontFace: 'Patrick Hand SC', valign: 'middle' });
});
// Clinical note: vesical fistula
box(sl, 7.2, 5.3, 5.8, 1.15, RED_BG, RED, null, {});
sl.addText("⚕ CLINICAL: Lymphatic spread of bladder carcinoma", { x: 7.3, y: 5.36, w: 5.6, h: 0.3, fontSize: 11, bold: true, color: RED, fontFace: 'Patrick Hand SC' });
sl.addText([
{ text: "Bladder TCC spreads to → External iliac → Common iliac → Para-aortic\n", options: { color: INK } },
{ text: "Trigone tumors → directly to internal iliac & obturator nodes\n", options: { color: INK } },
{ text: "Check obturator nodes in radical cystectomy!", options: { bold: true, color: RED } },
], { x: 7.3, y: 5.68, w: 5.6, h: 0.73, fontSize: 10, fontFace: 'Patrick Hand SC', lineSpacingMultiple: 1.2 });
sl.addText("MNEMONIC - Arterial supply: 'SLIM' = Superior Vesical, (inferior) Linings vesical, Internal iliac Main trunk", {
x: 1.2, y: 6.95, w: 11.5, h: 0.35, fontSize: 10.5, color: PURPLE, fontFace: 'Patrick Hand SC', italic: true, align: 'center'
});
}
// ─── SLIDE 5: Nerve Supply ────────────────────────────────────────────────────
{
const sl = pres.addSlide();
addRuledBg(sl);
slideHeader(sl, "4. NERVE SUPPLY & SPHINCTERS", "Urinary Bladder | Anatomy");
// Left column: nerve table
sl.addText("Innervation of Urinary Bladder", { x: 1.2, y: 0.75, w: 5.7, h: 0.35, fontSize: 14, bold: true, color: HEADING, fontFace: 'Patrick Hand SC', underline: true });
const nerves = [
{
type: "PARASYMPATHETIC",
level: "S2, S3, S4 (Pelvic splanchnic nerves)",
path: "Via inferior hypogastric / pelvic plexus → postganglionic in bladder wall",
effects: [
"Contracts DETRUSOR (via M3 muscarinic receptors)",
"Relaxes INTERNAL SPHINCTER (via NO release)",
"→ MICTURITION (S2-S4 keeps the urine off the floor!)"
],
bg: LIGHT_BG, col: HEADING
},
{
type: "SYMPATHETIC",
level: "T11–L2 (Hypogastric nerve / inf. mesenteric plexus)",
path: "Via superior & inferior hypogastric plexus → vesical plexus",
effects: [
"β₃ receptors: RELAXES detrusor (bladder filling)",
"α₁ receptors: CONTRACTS internal urethral sphincter",
"→ STORAGE (bladder fills, urine retained)"
],
bg: "FEF9E7", col: ORANGE
},
{
type: "SOMATIC (Pudendal Nerve)",
level: "S2, S3, S4",
path: "Via pudendal nerve → perineal nerve → external sphincter",
effects: [
"Maintains TONIC CONTRACTION of external (rhabdosphincter)",
"Voluntary control over micturition",
"Nicotinic ACh receptors → skeletal muscle contraction"
],
bg: GREEN_BG, col: GREEN
},
{
type: "AFFERENT (Sensory)",
level: "Travel with both para & sympathetic",
path: "Stretch receptors in detrusor → sense fullness. Pain fibers via sympathetics (T11-L2)",
effects: [
"Urgency & pain travel in SYMPATHETIC fibers",
"Stretch/fullness sensation in PARASYMPATHETIC (S2-4)",
"Pain referred to hypogastrium, perineum, inner thigh"
],
bg: "FDF2F8", col: PURPLE
},
];
nerves.forEach((n, i) => {
box(sl, 1.2, 1.12 + i * 1.55, 5.7, 1.47, n.bg, n.col, null, {});
sl.addText(n.type, { x: 1.3, y: 1.17 + i * 1.55, w: 5.5, h: 0.3, fontSize: 11.5, bold: true, color: n.col, fontFace: 'Patrick Hand SC' });
sl.addText("Level: " + n.level, { x: 1.3, y: 1.48 + i * 1.55, w: 5.5, h: 0.25, fontSize: 9.5, color: HEADING, fontFace: 'Patrick Hand SC', italic: true });
sl.addText(n.effects.map(e => "→ " + e).join("\n"), { x: 1.3, y: 1.74 + i * 1.55, w: 5.5, h: 0.82, fontSize: 9.5, color: INK, fontFace: 'Patrick Hand SC', lineSpacingMultiple: 1.15, wrap: true });
});
// Right: Sphincters + micturition
sl.addText("Sphincters of Bladder", { x: 7.2, y: 0.75, w: 5.8, h: 0.35, fontSize: 14, bold: true, color: HEADING, fontFace: 'Patrick Hand SC', underline: true });
const sphincters = [
{
name: "INTERNAL URETHRAL SPHINCTER",
type: "SMOOTH muscle (involuntary)",
location: "At bladder neck / junction with urethra",
nerve: "Sympathetic (α₁) → contracts; Parasympathetic (NO) → relaxes",
bg: LIGHT_BG, col: HEADING
},
{
name: "EXTERNAL URETHRAL SPHINCTER",
type: "SKELETAL (striated) muscle (voluntary)",
location: "Surrounds membranous urethra; within deep perineal pouch",
nerve: "Somatic - Pudendal nerve (S2-4) → tonic contraction maintained",
bg: GREEN_BG, col: GREEN
},
];
sphincters.forEach((s, i) => {
box(sl, 7.2, 1.12 + i * 1.7, 5.8, 1.6, s.bg, s.col, null, {});
sl.addText(s.name, { x: 7.3, y: 1.17 + i * 1.7, w: 5.6, h: 0.32, fontSize: 12, bold: true, color: s.col, fontFace: 'Patrick Hand SC' });
sl.addText([
{ text: "Type: ", options: { bold: true, color: s.col } }, { text: s.type + "\n", options: { color: INK } },
{ text: "Location: ", options: { bold: true, color: s.col } }, { text: s.location + "\n", options: { color: INK } },
{ text: "Nerve: ", options: { bold: true, color: s.col } }, { text: s.nerve, options: { color: INK } },
], { x: 7.3, y: 1.52 + i * 1.7, w: 5.6, h: 1.1, fontSize: 10, fontFace: 'Patrick Hand SC', lineSpacingMultiple: 1.25 });
});
box(sl, 7.2, 4.6, 5.8, 2.2, "FEF9E7", ORANGE, null, {});
sl.addText("MICTURITION REFLEX (Summary)", { x: 7.3, y: 4.66, w: 5.6, h: 0.3, fontSize: 12, bold: true, color: ORANGE, fontFace: 'Patrick Hand SC' });
sl.addText([
{ text: "FILLING phase (SYMPATHETIC dominates):\n", options: { bold: true, color: ORANGE } },
{ text: " β₃ → detrusor relaxes; α₁ → internal sphincter CONTRACTS\n Pudendal → external sphincter CONTRACTS\n\n", options: { color: INK } },
{ text: "VOIDING phase (PARASYMPATHETIC dominates):\n", options: { bold: true, color: HEADING } },
{ text: " Stretch receptors → afferents → S2-4 → efferents → ACh\n", options: { color: INK } },
{ text: " Detrusor CONTRACTS + both sphincters RELAX\n\n", options: { color: INK } },
{ text: "VOLUNTARY CONTROL: Cortex inhibits → pudendal maintains contraction\n", options: { color: GREEN, bold: true } },
{ text: "Higher center (pons micturition center / Barrington's nucleus) coordinates\n", options: { color: INK } },
], { x: 7.3, y: 4.99, w: 5.6, h: 1.75, fontSize: 9.5, fontFace: 'Patrick Hand SC', lineSpacingMultiple: 1.15 });
sl.addText("★ DETRUSOR = Pelvic nerve (S2-4) | SPHINCTER = Pudendal (S2-4) | STORAGE = Hypogastric (L1-2)", {
x: 1.2, y: 7.0, w: 11.5, h: 0.35, fontSize: 10.5, bold: true, color: PURPLE, fontFace: 'Patrick Hand SC', align: 'center'
});
}
// ─── SLIDE 6: Embryology ─────────────────────────────────────────────────────
{
const sl = pres.addSlide();
addRuledBg(sl);
slideHeader(sl, "5. EMBRYOLOGY OF URINARY BLADDER", "Urinary Bladder | Anatomy");
sl.addText("Development Overview", { x: 1.2, y: 0.75, w: 6, h: 0.35, fontSize: 14, bold: true, color: ORANGE, fontFace: 'Patrick Hand SC', underline: true });
// Timeline boxes
const stages = [
{ week: "Week 4", event: "Cloaca forms (expanded hindgut terminal part)", detail: "Receives allantois anteriorly, hindgut posteriorly, and mesonephric ducts laterally" },
{ week: "Week 4-7", event: "Urorectal septum divides cloaca", detail: "→ Urogenital sinus (anterior) + Rectum (posterior)" },
{ week: "Week 5-7", event: "3 parts of urogenital sinus form", detail: "VESICAL part → bladder body\nPELVIC part → urethra neck\nPHALLIC part → grows toward genital tubercle" },
{ week: "Week 7-12", event: "Allantois obliterates → URACHUS", detail: "Urachus = fibrous cord from apex of bladder to umbilicus → Adult = MEDIAN UMBILICAL LIGAMENT" },
{ week: "Week 8-12", event: "Mesonephric ducts absorbed into bladder wall", detail: "Contribute connective tissue to TRIGONE\nUreters gain separate openings into bladder\nTrigone mucosa → MESODERMAL origin" },
];
stages.forEach((s, i) => {
box(sl, 1.2, 1.15 + i * 1.2, 6.0, 1.1, i % 2 === 0 ? "FFF8EC" : LIGHT_BG, ORANGE, null, {});
sl.addShape(pres.ShapeType.rect, { x: 1.2, y: 1.15 + i * 1.2, w: 1.05, h: 1.1, fill: { color: ORANGE }, line: { color: ORANGE } });
sl.addText(s.week, { x: 1.22, y: 1.2 + i * 1.2, w: 1.0, h: 1.0, fontSize: 10, bold: true, color: "FFFFFF", fontFace: 'Patrick Hand SC', align: 'center', valign: 'middle' });
sl.addText(s.event, { x: 2.3, y: 1.18 + i * 1.2, w: 4.8, h: 0.3, fontSize: 11, bold: true, color: ORANGE, fontFace: 'Patrick Hand SC' });
sl.addText(s.detail, { x: 2.3, y: 1.5 + i * 1.2, w: 4.8, h: 0.7, fontSize: 10, color: INK, fontFace: 'Patrick Hand SC', wrap: true, lineSpacingMultiple: 1.15 });
});
// Right column
sl.addText("Urachal Remnants & Anomalies", { x: 7.5, y: 0.75, w: 5.5, h: 0.35, fontSize: 14, bold: true, color: RED, fontFace: 'Patrick Hand SC', underline: true });
const urachus = [
{ name: "Patent Urachus", desc: "Urachus remains open → Urine drains from umbilicus", color: RED },
{ name: "Urachal Cyst", desc: "Obliterated at both ends but patent in middle → cyst forms; can become infected", color: PURPLE },
{ name: "Urachal Sinus", desc: "Open at umbilical end only → drains at umbilicus", color: ORANGE },
{ name: "Vesicourachal Diverticulum", desc: "Open at bladder end only → diverticulum at apex of bladder", color: HEADING },
{ name: "Urachal Adenocarcinoma", desc: "Rare (~1% of bladder tumors); located at dome/apex; often mucin-secreting adenocarcinoma", color: RED },
];
urachus.forEach((u, i) => {
box(sl, 7.5, 1.12 + i * 1.2, 5.5, 1.1, i % 2 === 0 ? RED_BG : "FEF9E7", u.color, null, {});
sl.addText(u.name, { x: 7.62, y: 1.16 + i * 1.2, w: 5.3, h: 0.3, fontSize: 11, bold: true, color: u.color, fontFace: 'Patrick Hand SC' });
sl.addText(u.desc, { x: 7.62, y: 1.48 + i * 1.2, w: 5.3, h: 0.7, fontSize: 10, color: INK, fontFace: 'Patrick Hand SC', wrap: true, lineSpacingMultiple: 1.15 });
});
sl.addText("Epithelium origin: Bladder body (endoderm of cloaca) | Trigone (mesoderm of mesonephric duct)", {
x: 1.2, y: 7.05, w: 11.5, h: 0.35, fontSize: 10.5, bold: true, color: ORANGE, fontFace: 'Patrick Hand SC', align: 'center'
});
}
// ─── SLIDE 7: Clinical Applied Anatomy ───────────────────────────────────────
{
const sl = pres.addSlide();
addRuledBg(sl);
slideHeader(sl, "6. CLINICAL APPLIED ANATOMY", "Urinary Bladder | HIGH YIELD");
const clinicals = [
{
title: "1. Suprapubic Cystostomy",
content: "Distended bladder rises above pubic symphysis → peritoneum peels off anterior wall. Needle/trocar inserted just above pubic symphysis avoids peritoneum → extraperitoneal access to bladder. Used in: urethral trauma, BPH, post-op retention.",
col: HEADING, bg: LIGHT_BG
},
{
title: "2. Vesicoureteric Reflux (VUR)",
content: "Ureters enter bladder OBLIQUELY through detrusor (2-3 cm intramural course). Detrusor tone compresses ureter → antireflux valve. If obliquity lost (short intramural segment) → urine refluxes to kidney → recurrent UTI, hydronephrosis, scarring.",
col: GREEN, bg: GREEN_BG
},
{
title: "3. Neurogenic Bladder",
content: "Upper Motor Neuron lesion (above S2-4): Spastic/reflex bladder → detrusor overactivity, small capacity, incontinence.\nLower Motor Neuron lesion (S2-4 / conus medullaris): Flaccid/autonomous bladder → urinary retention, overflow incontinence, large residual volume.",
col: PURPLE, bg: "F9F0FF"
},
{
title: "4. Bladder Injuries",
content: "Intraperitoneal rupture (dome): Blunt abdominal trauma with full bladder → urine into peritoneum → peritonitis. Extraperitoneal rupture: Pelvic fracture lacerates anterolateral wall → urine in retropubic/pelvic fat. Iatrogenic: Midline incision extended to pubis may injure full bladder.",
col: RED, bg: RED_BG
},
{
title: "5. Bladder Carcinoma",
content: "Most common: Transitional Cell Ca (TCC/Urothelial Ca). Presents with painless hematuria. Trigone is common site. Spreads → external iliac, internal iliac nodes. Schistosomiasis → squamous cell Ca (S. haematobium; calcification on X-ray). Risk: smoking, aniline dyes, cyclophosphamide (hemorrhagic cystitis → Ca).",
col: "922B21", bg: "#FDEDEC"
},
{
title: "6. Cystitis & Trigone",
content: "Cystitis (UTI) → inflammation → trigone involvement → frequency, dysuria, urgency. Trigone is most sensitive area. Female > Male (short urethra 3-4 cm vs male 20 cm). Interstitial cystitis: chronic, sterile inflammation → Hunner's ulcers on trigone/posterior wall.",
col: ORANGE, bg: "FFF8EC"
},
];
clinicals.forEach((c, i) => {
const col = i < 3 ? 0 : 1;
const row = i % 3;
const x = col === 0 ? 1.2 : 7.2;
const y = 0.78 + row * 2.12;
box(sl, x, y, 5.7, 2.04, c.bg, c.col, null, {});
sl.addText(c.title, { x: x + 0.1, y: y + 0.06, w: 5.5, h: 0.32, fontSize: 11.5, bold: true, color: c.col, fontFace: 'Patrick Hand SC' });
sl.addShape(pres.ShapeType.line, { x: x + 0.1, y: y + 0.4, w: 5.5, h: 0, line: { color: c.col, width: 0.5 } });
sl.addText(c.content, { x: x + 0.1, y: y + 0.44, w: 5.5, h: 1.55, fontSize: 9.5, color: INK, fontFace: 'Patrick Hand SC', wrap: true, lineSpacingMultiple: 1.18 });
});
sl.addText("⚕ See also: BPH (prostate compresses bladder neck), Pelvic floor disorders (female), Detrusor overactivity", {
x: 1.2, y: 7.08, w: 11.5, h: 0.3, fontSize: 10, color: "7F8C8D", fontFace: 'Patrick Hand SC', align: 'center'
});
}
// ─── SLIDE 8: More Clinical - Fistulae, TURBT, Cystoscopy ─────────────────
{
const sl = pres.addSlide();
addRuledBg(sl);
slideHeader(sl, "7. MORE CLINICAL CORRELATES", "Urinary Bladder | Applied Anatomy");
// Left: vesical fistulae
sl.addText("Vesical Fistulae", { x: 1.2, y: 0.75, w: 5.7, h: 0.35, fontSize: 14, bold: true, color: RED, fontFace: 'Patrick Hand SC', underline: true });
const fistulae = [
{ name: "Vesicovaginal Fistula", cause: "Obstetric trauma, gynecological surgery, cervical Ca, radiotherapy", feature: "Continuous urinary incontinence per vagina; commonest pelvic fistula in developing countries" },
{ name: "Vesicointestinal (Colovesical)", cause: "Diverticular disease, Crohn's, colorectal Ca, pelvic surgery", feature: "Pneumaturia (gas in urine) + fecaluria → PATHOGNOMONIC. Recurrent UTI with mixed organisms" },
{ name: "Vesicouterine", cause: "LSCS complications (lower segment), uterine rupture", feature: "Cyclical hematuria (Youssef's syndrome) + amenorrhea + urinary incontinence" },
{ name: "Urethrovaginal", cause: "Obstetric trauma / anterior colporrhaphy", feature: "Incontinence position-dependent; leakage into vagina" },
];
fistulae.forEach((f, i) => {
box(sl, 1.2, 1.15 + i * 1.5, 5.7, 1.4, i % 2 === 0 ? RED_BG : "FDF2F8", RED, null, {});
sl.addText(f.name, { x: 1.3, y: 1.19 + i * 1.5, w: 5.5, h: 0.3, fontSize: 11, bold: true, color: RED, fontFace: 'Patrick Hand SC' });
sl.addText("Cause: " + f.cause, { x: 1.3, y: 1.51 + i * 1.5, w: 5.5, h: 0.28, fontSize: 9.5, color: HEADING, fontFace: 'Patrick Hand SC', wrap: true });
sl.addText("Feature: " + f.feature, { x: 1.3, y: 1.8 + i * 1.5, w: 5.5, h: 0.3, fontSize: 9.5, color: INK, fontFace: 'Patrick Hand SC', wrap: true });
});
// Right column
sl.addText("Cystoscopy & Surgical Notes", { x: 7.2, y: 0.75, w: 5.8, h: 0.35, fontSize: 14, bold: true, color: HEADING, fontFace: 'Patrick Hand SC', underline: true });
box(sl, 7.2, 1.12, 5.8, 1.6, LIGHT_BG, HEADING, null, {});
sl.addText("Cystoscopy Landmarks", { x: 7.3, y: 1.18, w: 5.6, h: 0.3, fontSize: 11.5, bold: true, color: HEADING, fontFace: 'Patrick Hand SC' });
sl.addText([
{ text: "• Trigone: Smooth, pale → most common tumor site; easy to see\n", options: { color: INK } },
{ text: "• Ureteric orifices: Slit-like openings; efflux of urine visible\n", options: { color: INK } },
{ text: "• Interureteric ridge (bar): Visible as transverse fold\n", options: { color: INK } },
{ text: "• Uvula vesicae (male): Elevation above internal meatus\n", options: { color: INK } },
{ text: "• Bladder dome: Rugae present (redundant mucosa)\n", options: { color: INK } },
], { x: 7.3, y: 1.5, w: 5.6, h: 1.16, fontSize: 10, fontFace: 'Patrick Hand SC', lineSpacingMultiple: 1.2 });
box(sl, 7.2, 2.8, 5.8, 1.55, GREEN_BG, GREEN, null, {});
sl.addText("TURBT & Radical Cystectomy", { x: 7.3, y: 2.86, w: 5.6, h: 0.3, fontSize: 11.5, bold: true, color: GREEN, fontFace: 'Patrick Hand SC' });
sl.addText([
{ text: "TURBT (Trans-Urethral Resection of Bladder Tumor):\n", options: { bold: true, color: GREEN } },
{ text: " • Peritoneal perforation risk → dome is extraperitoneal (ant) but superior dome = peritoneum\n • Risk of obturator nerve stimulation → adductor spasm (obturator reflex) during lateral wall resection\n\n", options: { color: INK } },
{ text: "Radical Cystectomy: ", options: { bold: true, color: GREEN } }, { text: "Incision in retropubic space (of Retzius); identify median umbilical ligament (obliterated urachus) as guide to dome", options: { color: INK } },
], { x: 7.3, y: 3.18, w: 5.6, h: 1.12, fontSize: 9.5, fontFace: 'Patrick Hand SC', lineSpacingMultiple: 1.18 });
box(sl, 7.2, 4.43, 5.8, 1.55, "FEF9E7", ORANGE, null, {});
sl.addText("Space of Retzius (Retropubic Space)", { x: 7.3, y: 4.49, w: 5.6, h: 0.3, fontSize: 11.5, bold: true, color: ORANGE, fontFace: 'Patrick Hand SC' });
sl.addText([
{ text: "Extraperitoneal potential space between pubis/rectus & bladder\n", options: { color: INK } },
{ text: "Contents: loose areolar tissue, fat, vesical venous plexus\n", options: { color: INK } },
{ text: "Clinical: Catheterization, suprapubic cystostomy, radical prostatectomy, bladder surgery all use this space\n", options: { color: INK } },
{ text: "Retropubic hematoma after pelvic fracture fills this space!", options: { bold: true, color: RED } },
], { x: 7.3, y: 4.82, w: 5.6, h: 1.1, fontSize: 9.5, fontFace: 'Patrick Hand SC', lineSpacingMultiple: 1.18 });
box(sl, 7.2, 6.05, 5.8, 1.2, RED_BG, RED, null, {});
sl.addText("Overflow / Stress Incontinence", { x: 7.3, y: 6.11, w: 5.6, h: 0.28, fontSize: 11, bold: true, color: RED, fontFace: 'Patrick Hand SC' });
sl.addText([
{ text: "Stress incontinence (F): Weakened pelvic floor → urethrovesical junction descends → loss of posterior urethrovesical angle → leakage on coughing/sneezing → treat with pelvic floor exercises / TVT\n", options: { color: INK } },
{ text: "Overflow incontinence: BPH → chronic retention → paradoxical incontinence\n", options: { color: INK } },
], { x: 7.3, y: 6.42, w: 5.6, h: 0.78, fontSize: 9.5, fontFace: 'Patrick Hand SC', lineSpacingMultiple: 1.15 });
sl.addText("Remember: Obturator nerve (L2-4) lies on lateral bladder wall → at risk in radical cystectomy & pelvic node dissection", {
x: 1.2, y: 7.08, w: 11.5, h: 0.3, fontSize: 10, bold: true, color: PURPLE, fontFace: 'Patrick Hand SC', align: 'center'
});
}
// ─── SLIDE 9: Quick Revision / Summary Table ─────────────────────────────────
{
const sl = pres.addSlide();
addRuledBg(sl);
slideHeader(sl, "8. QUICK REVISION TABLE", "Urinary Bladder | One-Page Summary");
// Summary table
const tHeaders = ["Feature", "Detail", "Key Point"];
const rows = [
["Position", "Lesser pelvis, behind pubic symphysis", "When FULL → rises above symphysis (abdominal!)"],
["Parts", "Apex, Body, Fundus (Base), Neck", "Neck = most fixed part"],
["Capacity", "~500 mL; urge at ~300 mL", "Children: bladder is abdominal organ"],
["Lining", "Transitional epithelium (Urothelium)", "4-6 layers (empty); 2 layers (full)"],
["Trigone", "Smooth triangular area at base; no rugae", "Derived from mesonephric duct (mesoderm)"],
["Detrusor", "3 smooth muscle layers; inner+outer=longitudinal, mid=circular", "Contracts: Parasympathetic (M3); Relaxes: Sympathetic (β₃)"],
["Int. Sphincter", "Smooth muscle at bladder neck", "Sympathetic (α₁) contracts; Parasympathetic relaxes"],
["Ext. Sphincter", "Skeletal muscle; membranous urethra", "Pudendal nerve (S2-4); VOLUNTARY"],
["Arterial supply", "Superior & inferior vesical arteries", "From internal iliac artery"],
["Venous", "Vesical venous plexus → internal iliac veins", "Communicates with Batson's plexus"],
["Lymphatics (sup)", "External iliac nodes", "Superior & lateral walls"],
["Lymphatics (base)", "Internal iliac nodes", "Fundus, trigone, anterior wall"],
["Sympathetic", "T11–L2 via hypogastric nerve", "FILLING: detrusor relaxes, sphincter contracts"],
["Parasympathetic", "S2–S4 pelvic splanchnic nerves", "VOIDING: detrusor contracts, sphincter relaxes"],
["Peritoneum", "Superior surface only (+ post. above trigone)", "Anterior wall = NO peritoneum → safe for suprapubic puncture"],
["Embryology", "Vesical part of urogenital sinus (endoderm)", "Urachus → median umbilical ligament"],
["Most common Ca", "TCC / Urothelial carcinoma", "Painless hematuria; spreads to external & internal iliac nodes"],
["VUR", "Ureters enter obliquely (antireflux)", "Short intramural segment → VUR → UTI, hydronephrosis"],
];
// Draw table
const tX = 1.1, tY = 0.72, cellH = 0.35;
const colW = [2.5, 5.0, 4.5];
const hdrColors = [HEADING, HEADING, HEADING];
// Header row
let cx = tX;
tHeaders.forEach((h, c) => {
sl.addShape(pres.ShapeType.rect, { x: cx, y: tY, w: colW[c], h: 0.38, fill: { color: HEADING }, line: { color: "FFFFFF", width: 0.5 } });
sl.addText(h, { x: cx + 0.05, y: tY + 0.05, w: colW[c] - 0.1, h: 0.28, fontSize: 11, bold: true, color: "FFFFFF", fontFace: 'Patrick Hand SC', valign: 'middle' });
cx += colW[c];
});
rows.forEach((row, r) => {
const rowBg = r % 2 === 0 ? "F0F4F8" : "FFFDF4";
cx = tX;
row.forEach((cell, c) => {
sl.addShape(pres.ShapeType.rect, { x: cx, y: tY + 0.38 + r * cellH, w: colW[c], h: cellH, fill: { color: rowBg }, line: { color: "C8D6E1", width: 0.3 } });
const fontSize = cell.length > 60 ? 8 : 9;
sl.addText(cell, { x: cx + 0.05, y: tY + 0.38 + r * cellH + 0.02, w: colW[c] - 0.1, h: cellH - 0.04, fontSize, color: c === 2 ? RED : INK, fontFace: 'Patrick Hand SC', valign: 'middle', wrap: true });
cx += colW[c];
});
});
}
// ─── SLIDE 10: Mnemonics & Memory Aids ────────────────────────────────────────
{
const sl = pres.addSlide();
addRuledBg(sl);
slideHeader(sl, "9. MNEMONICS & MEMORY AIDS", "Urinary Bladder | Exam Tips");
const mnemonics = [
{
title: "Parts of Bladder: 'A Big Fat Neck'",
details: "A = Apex (attached to median umbilical lig.)\nB = Body (main part)\nF = Fundus/Base (receives ureters)\nN = Neck (continues as urethra; most FIXED)",
col: HEADING, bg: LIGHT_BG
},
{
title: "S2,3,4 Keep Urine Off The Floor",
details: "Pelvic splanchnic nerves (parasympathetic S2-S4) → CONTRACT detrusor → MICTURITION\nAlso pudendal nerve (S2-4) → SOMATIC control of external sphincter",
col: GREEN, bg: GREEN_BG
},
{
title: "Arterial Supply: 'SIVA'",
details: "S = Superior vesical artery (from umbilical a.)\nI = Inferior vesical artery (internal iliac a.)\nV = Vesical plexus drains to internal iliac veins\nA = All from INTERNAL ILIAC artery system",
col: RED, bg: RED_BG
},
{
title: "Trigone: 2U+1U = Triangle",
details: "2 Ureteric orifices (superolateral angles)\n+1 Urethral orifice (internal; inferior angle)\n= TRIGONE (base of bladder)\nConnected by Interureteric ridge (Mercier's bar)",
col: ORANGE, bg: "FFF8EC"
},
{
title: "Lymphatics: 'External wall → External nodes'",
details: "Upper & lateral walls → EXTERNAL iliac nodes\nBase & Trigone → INTERNAL iliac nodes\nAll → ultimately → PARA-AORTIC nodes",
col: PURPLE, bg: "F9F0FF"
},
{
title: "Filling vs Voiding (PSVP rule)",
details: "Para S2-4 → Voiding (contracts detrusor)\nSympathetic T11-L2 → Storage/Filling (relaxes detrusor, closes sphincter)\nVoluntary = Pudendal nerve (S2-4) → VOLUNTARY hold",
col: "1A5276", bg: "EAF2FF"
},
{
title: "Urachal Anomalies: 'PCSD'",
details: "P = Patent urachus (urine at umbilicus)\nC = Cyst (infected swelling at midline)\nS = Sinus (opens at umbilicus only)\nD = Diverticulum (opens at bladder apex only)",
col: ORANGE, bg: "FFF8EC"
},
{
title: "Bladder Cancer Memory Aid: 'TCC SMOKES'",
details: "T = TCC/Urothelial Ca (most common)\nC = Cyclophosphamide → hemorrhagic cystitis → risk\nS = Schistosomiasis → Squamous cell Ca\nM = Male (3:1 over female)\nO = painless hematuria (Obvious sign)\nK = Know: trigone most common site\nE = External iliac nodes (lymph spread)\nS = Smoking = #1 risk factor",
col: "922B21", bg: "#FDEDEC"
},
];
mnemonics.forEach((m, i) => {
const col = i < 4 ? 0 : (i < 8 ? 1 : 2);
const row = i % 4;
const x = [1.2, 5.55, 9.85][col];
const y = 0.75 + row * 1.66;
box(sl, x, y, 4.1, 1.58, m.bg, m.col, null, {});
sl.addText(m.title, { x: x + 0.1, y: y + 0.06, w: 3.9, h: 0.32, fontSize: 10.5, bold: true, color: m.col, fontFace: 'Patrick Hand SC', wrap: true });
sl.addShape(pres.ShapeType.line, { x: x + 0.1, y: y + 0.4, w: 3.9, h: 0, line: { color: m.col, width: 0.5, dashType: 'dash' } });
sl.addText(m.details, { x: x + 0.1, y: y + 0.44, w: 3.9, h: 1.1, fontSize: 9.5, color: INK, fontFace: 'Patrick Hand SC', wrap: true, lineSpacingMultiple: 1.18 });
});
sl.addText("Good Luck! 🎓 Revise with clinical MCQs on urinary bladder • Topic: Applied Anatomy", {
x: 0.5, y: 7.1, w: 12.3, h: 0.3, fontSize: 10.5, color: "7F8C8D", fontFace: 'Patrick Hand SC', align: 'center'
});
}
// ─── Write file ──────────────────────────────────────────────────────────────
pres.writeFile({ fileName: "/home/daytona/workspace/bladder-notes/Urinary_Bladder_Anatomy_Notes.pptx" })
.then(() => console.log("✅ PPTX created successfully!"))
.catch(err => console.error("❌ Error:", err));
cd /home/daytona/workspace/bladder-notes && node create_notes.js 2>&1
ls -lh /home/daytona/workspace/bladder-notes/
Urinary Bladder Anatomy Notes
Presentation · PPTX
What's Inside (10 Slides)
| Slide | Topic | Highlights |
|---|---|---|
| 1 | Title Page | Topic overview, date field |
| 2 | Introduction & Position | Parts (APEX / BODY / FUNDUS / NECK), male vs female relations, peritoneal coverage |
| 3 | Interior & Histology | Trigone (Mercier's bar, uvula vesicae), 4 wall layers, urothelium, detrusor, receptor pharmacology |
| 4 | Blood Supply & Lymphatics | Superior/inferior vesical arteries from internal iliac, vesical venous plexus → Batson's plexus, lymph node stations |
| 5 | Nerve Supply & Sphincters | Parasympathetic S2-4 / Sympathetic T11-L2 / Pudendal nerve, filling vs voiding table, micturition reflex |
| 6 | Embryology | Week-by-week timeline, urorectal septum, urachus → median umbilical ligament, 5 types of urachal remnants |
| 7 | Clinical Applied Anatomy | Suprapubic cystostomy, VUR, neurogenic bladder (UMN vs LMN), bladder injuries, carcinoma, cystitis |
| 8 | More Clinical | Vesical fistulae (4 types), cystoscopy landmarks, TURBT hazards, space of Retzius, stress incontinence |
| 9 | Quick Revision Table | 18-row summary: every feature in one table |
| 10 | Mnemonics | "A Big Fat Neck", "S2-3-4 keeps urine off the floor", SIVA, Trigone 2U+1U, PCSD, TCC SMOKES |
Key Diagrams Referenced
Do it fast
Urinary Bladder Anatomy Notes
Presentation · PPTX
It is not downloadable
ls -lh /home/daytona/workspace/bladder-notes/ && echo "File exists"
cp /home/daytona/workspace/bladder-notes/Urinary_Bladder_Anatomy_Notes.pptx /hom…
Urinary Bladder Anatomy Notes
Presentation · PPTX
Yes pdf
cd /home/daytona/workspace/bladder-notes && libreoffice --headless --convert-to …
libreoffice --headless --convert-to pdf /home/daytona/workspace/bladder-notes/Ur…
chmod 777 /home/daytona/workspace/bladder-notes/ && libreoffice --headless --con…
mkdir -p /tmp/bladder_out && libreoffice --headless --convert-to pdf /home/dayto…
cp /tmp/bladder_out/Urinary_Bladder_Anatomy_Notes.pdf /home/daytona/workspace/Ur…
Urinary Bladder Anatomy Notes
PDF Document · PDF
Don't create pdf just write it here
📓 URINARY BLADDER — Anatomy Notes
with Clinical Applied Anatomy
1. INTRODUCTION & POSITION
| Feature | Detail |
|---|---|
| Capacity | ~500 mL; urge to void at ~300 mL |
| Shape (empty) | Pyramidal / tetrahedral |
| Shape (full) | Ovoid; apex rises above pubic symphysis into abdomen |
| Most fixed part | Neck (held by prostate in male / UG diaphragm in female) |
2. PARTS OF THE BLADDER
A B F N → "A Big Fat Neck"
- Anterosuperior tip
- Attached to median umbilical ligament (obliterated urachus) → runs to umbilicus
- Landmark during bladder surgery
- Main bulk; has superior surface + 2 inferolateral surfaces
- Superior surface covered by peritoneum
- Anterolateral surfaces = no peritoneum (retropubic fat)
- Posterior wall, faces posteroinferiorly
- Receives 2 ureters at its superolateral angles
- Male: related to seminal vesicles + rectum
- Female: related to uterus/cervix + vagina
- Most inferior and fixed part
- Continuous with urethra below
- Male: rests on prostate gland
- Female: rests on perineal membrane / UG diaphragm
3. RELATIONS
Male
| Surface | Relation |
|---|---|
| Anterior | Retropubic space of Retzius, pubic symphysis |
| Superior | Peritoneum → loops of small intestine, sigmoid colon |
| Posterior | Seminal vesicles, vas deferens, rectovesical pouch, rectum |
| Inferior (neck) | Prostate gland |
Female
| Surface | Relation |
|---|---|
| Posterior (superior) | Uterus (body); separated by vesicouterine pouch |
| Posterior (base) | Anterior vaginal wall (firmly adherent) |
| Inferior (neck) | Perineal membrane / UG diaphragm |
⚠️ Peritoneum covers only the SUPERIOR surface + part of posterior above trigone. Anterior & lateral walls = extraperitoneal → safe for suprapubic puncture!
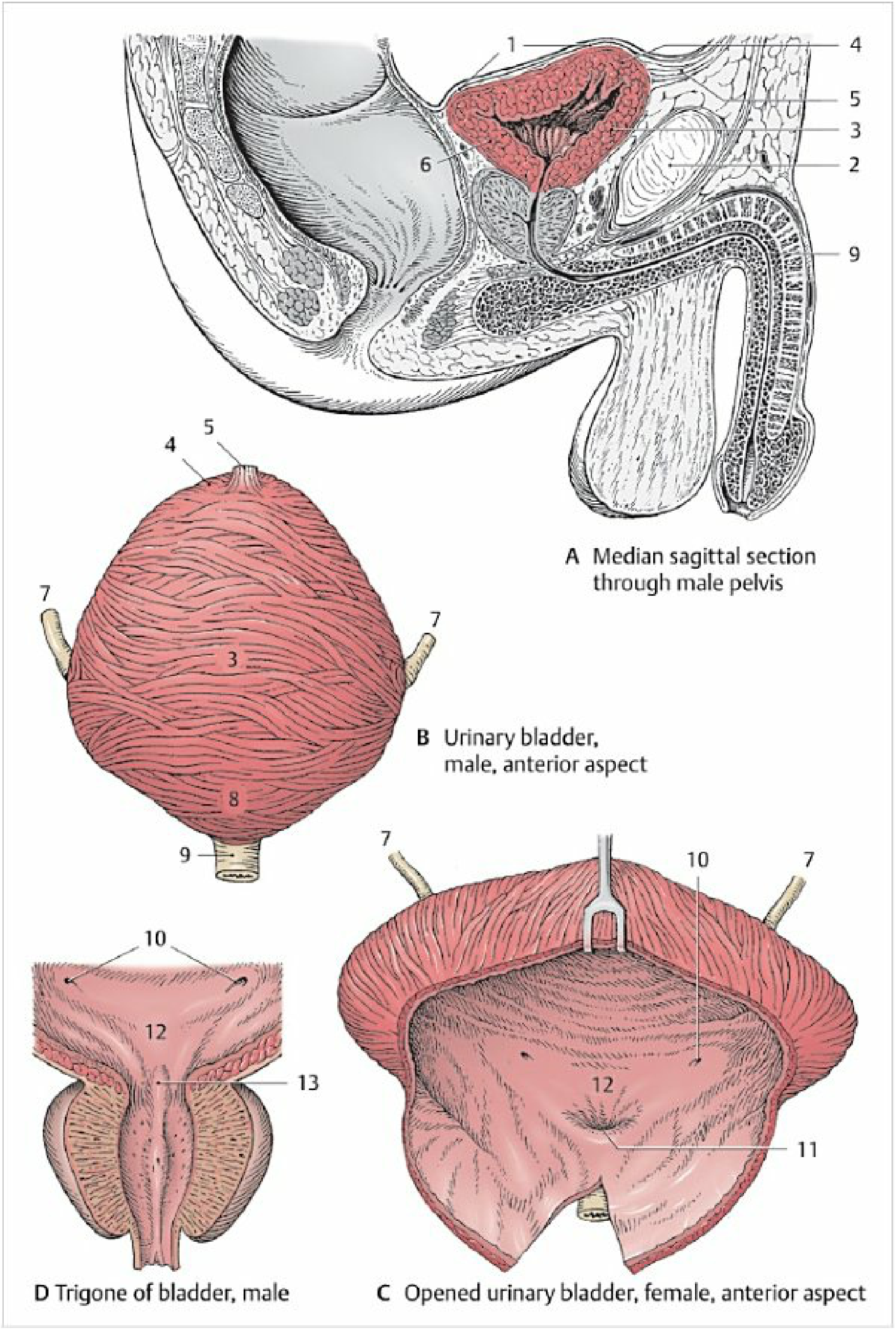
4. INTERIOR OF THE BLADDER
Mucosal Surface
- Most of bladder: Mucosa thrown into RUGAE / FOLDS when empty → disappear when distended
- Trigone: Smooth, no folds, firmly adherent to detrusor → permanent smooth area
THE TRIGONE (Most Important Area!)
Ureteric orifice (L) Ureteric orifice (R)
●──────────────────●
\ Interureteric \
\ ridge (bar) \
\ \
●
Internal urethral orifice
| Feature | Detail |
|---|---|
| Shape | Triangular |
| Superolateral angles (×2) | Ureteric orifices |
| Inferior angle | Internal urethral orifice |
| Transverse fold | Interureteric ridge (Mercier's bar) connecting ureteric orifices |
| In males | Uvula vesicae = small elevation above internal urethral orifice (due to median lobe of prostate) |
| Mucosa | Smooth, pale, always flat |
| Embryology | Derived from mesonephric duct (mesoderm) |
★ No muscularis mucosae or submucosa in trigone (unlike rest of bladder)
5. HISTOLOGY / LAYERS OF BLADDER WALL
Layer 1 — UROTHELIUM (Transitional Epithelium)
- Stratified; 4-6 cell layers when empty, 2-3 layers when distended
- Surface "umbrella cells" — tight junctions → barrier against urine
- Lines entire interior including trigone
Layer 2 — LAMINA PROPRIA
- Loose vascular connective tissue
- Contains thin muscularis mucosae (variable)
- ABSENT in trigone (trigone goes straight to muscle)
Layer 3 — DETRUSOR MUSCLE (Most Important!)
- Three ill-defined smooth muscle layers:
- Inner longitudinal
- Middle circular ← thickest
- Outer longitudinal
- At bladder neck → circular fibers condense → Internal Urethral Sphincter (involuntary)
- Receptor pharmacology:
- β₃ adrenergic → RELAXES detrusor (sympathetic, filling)
- M3 muscarinic → CONTRACTS detrusor (parasympathetic, voiding)
Layer 4 — ADVENTITIA / SEROSA
- Adventitia (fibrofatty) on most surfaces
- Serosa (peritoneum) only on superior surface + posterior above trigone
6. BLOOD SUPPLY
Arterial (all from Internal Iliac Artery)
| Artery | Source | Supply |
|---|---|---|
| Superior vesical artery | Umbilical artery (patent part) → internal iliac | Superior, anterior, lateral walls; upper ureter |
| Inferior vesical artery | Anterior trunk of internal iliac (M) / Vaginal artery (F) | Base, neck, seminal vesicles, prostate (M) |
| Middle rectal artery | Internal iliac | Minor contribution to base |
✏️ Rich collateral network → ligation of a single artery is NOT detrimental
Venous Drainage
- Vesical venous plexus surrounds fundus/base
- Drains → Internal Iliac Veins
- Communicates with prostatic plexus (M) / vaginal plexus (F)
- Also communicates with Batson's vertebral venous plexus → pathway for haematogenous metastasis!
7. LYMPHATIC DRAINAGE
| Region | Drains to |
|---|---|
| Superior & lateral walls | External iliac nodes |
| Base (fundus) & Trigone | Internal iliac nodes |
| Anterior wall | Internal iliac nodes (via obturator channel) |
| All above → ultimately | Para-aortic (lateral aortic) nodes |
★ Check obturator nodes during radical cystectomy — often skipped but involved early!
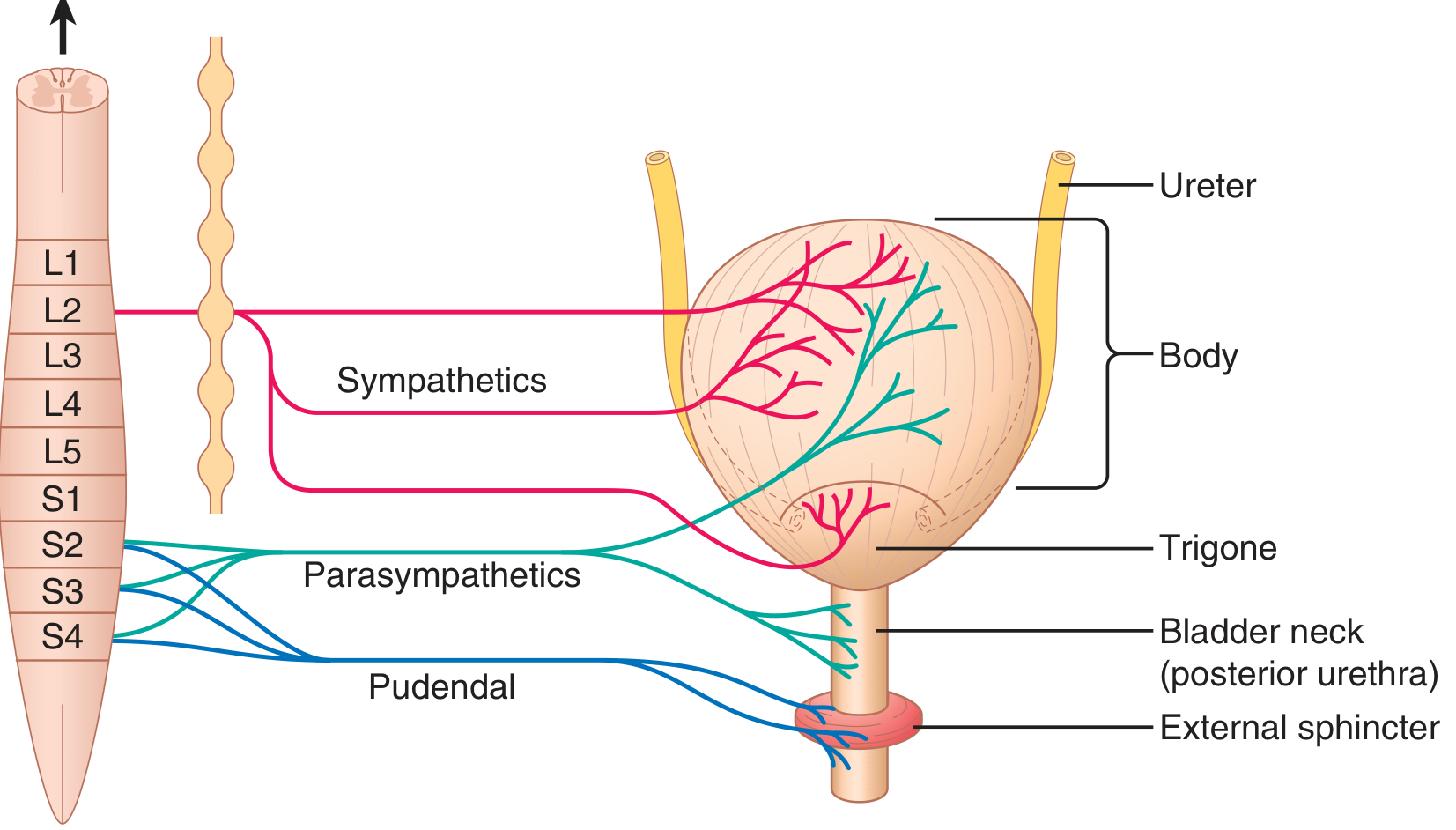
8. NERVE SUPPLY
MNEMONIC: "S2, 3, 4 keeps urine off the floor"
Parasympathetic (VOIDING)
- S2, S3, S4 → pelvic splanchnic nerves → inferior hypogastric plexus
- ACh → M3 receptors → detrusor CONTRACTS
- NO release → internal sphincter RELAXES
- = Micturition
Sympathetic (STORAGE / FILLING)
- T11–L2 → hypogastric nerve → inferior hypogastric plexus
- β₃ receptors → detrusor RELAXES
- α₁ receptors → internal sphincter CONTRACTS
- = Retention / filling
Somatic (VOLUNTARY)
- Pudendal nerve (S2, S3, S4)
- Innervates external urethral sphincter (striated/skeletal muscle)
- Tonic contraction = continent at rest
- Voluntary relaxation = micturition begins
Afferent (Sensory)
- Stretch receptors → via pelvic splanchnic (S2-4) → sense fullness
- Pain fibres → via sympathetic (T11-L2) → referred to hypogastrium / perineum / inner thigh
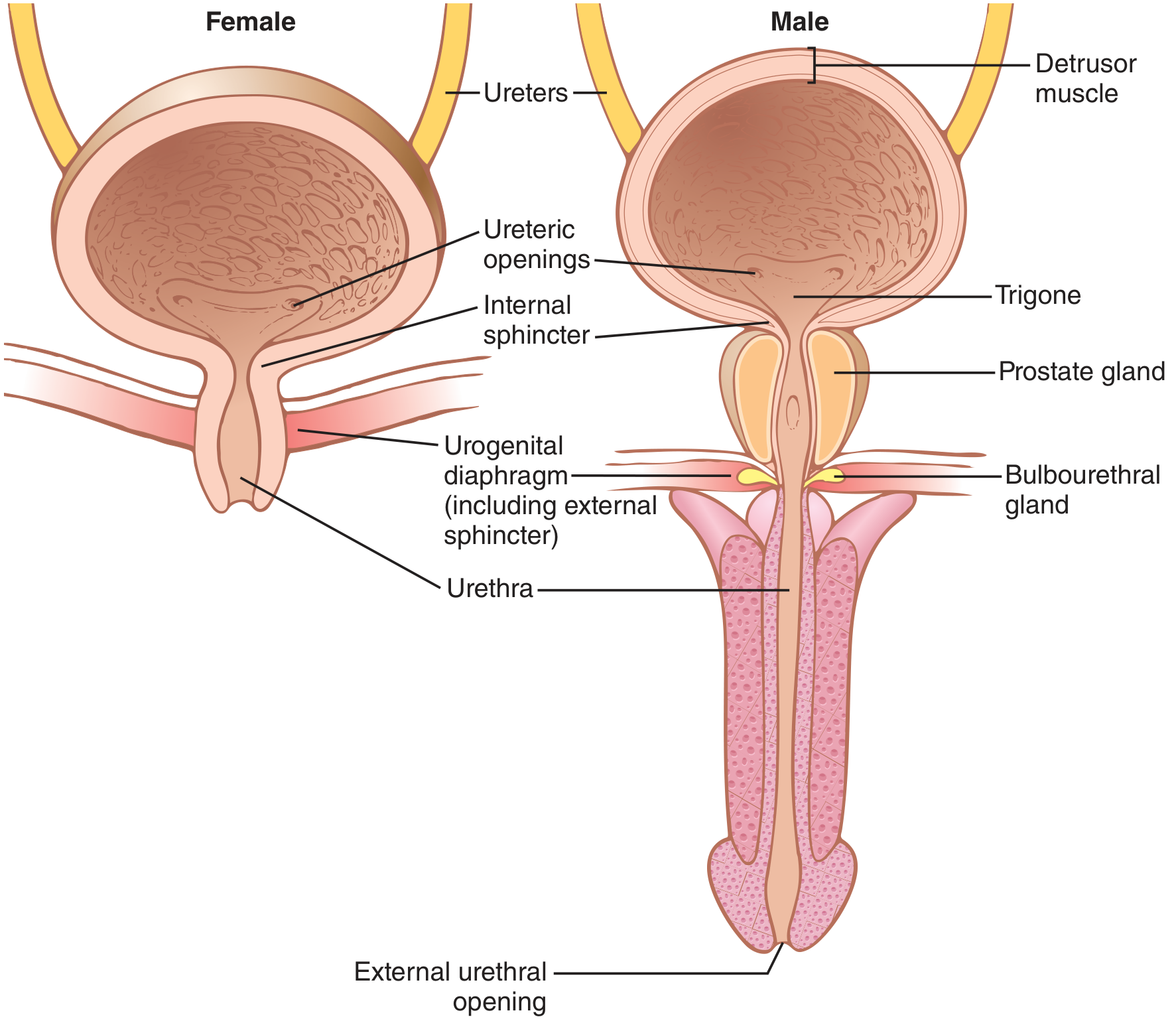
9. SPHINCTERS
| Feature | Internal Sphincter | External Sphincter |
|---|---|---|
| Muscle type | Smooth (involuntary) | Skeletal (voluntary) |
| Location | Bladder neck | Membranous urethra (deep perineal pouch) |
| Nerve | Sympathetic (α₁) contracts; Parasympathetic relaxes | Pudendal nerve S2-4 |
| Control | Autonomic | Voluntary (cortical) |
10. MICTURITION REFLEX
FILLING PHASE:
Bladder fills → stretch receptors quiet
Sympathetic dominates:
→ Detrusor RELAXES (β₃)
→ Int. sphincter CONTRACTS (α₁)
→ Pudendal → Ext. sphincter CONTRACTS
→ CONTINENT ✓
VOIDING PHASE:
~300 mL → stretch receptors fire → S2-4
Parasympathetic dominates:
→ Detrusor CONTRACTS (M3)
→ Int. sphincter RELAXES (NO)
→ Pudendal inhibited → Ext. sphincter RELAXES
→ MICTURITION ✓
VOLUNTARY CONTROL:
Pontine micturition centre (Barrington's nucleus)
+ Frontal cortex inhibit until appropriate
11. EMBRYOLOGY
Development Timeline
| Week | Event |
|---|---|
| Week 4 | Cloaca forms = expanded terminal hindgut |
| Week 4–7 | Urorectal septum divides cloaca → Urogenital sinus (ant.) + Rectum (post.) |
| Week 5–7 | UG sinus divides into 3 parts: Vesical (→ bladder body) + Pelvic (→ urethra) + Phallic |
| Week 7 | Allantois obliterates → Urachus (fibrous cord, apex to umbilicus) |
| Adult | Urachus → Median Umbilical Ligament |
| Week 8–12 | Mesonephric ducts absorbed → contribute to trigone connective tissue |
Epithelial Origins
- Bladder body epithelium → Endoderm of cloaca
- Trigone epithelium → Mesoderm (mesonephric duct)
Urachal Remnants — "PCSD + Ca" Mnemonic
| Type | What's Open | Feature |
|---|---|---|
| Patent urachus | Both ends | Urine drips from umbilicus |
| Cyst | Middle only | Midline infraumbilical swelling; can get infected |
| Sinus | Umbilical end | Discharges at umbilicus |
| Diverticulum | Bladder end | Outpouching at apex of bladder |
| Urachal Ca | — | Rare adenocarcinoma at dome; mucin-secreting |
12. CLINICAL APPLIED ANATOMY (HIGH YIELD)
① Suprapubic Cystostomy
- Distended bladder rises above pubic symphysis
- Peritoneum peels off anterior abdominal wall → extraperitoneal access
- Needle inserted just above symphysis pubis → taps bladder without entering peritoneum
- Used in: urethral trauma, BPH, post-op urinary retention
② Vesicoureteric Reflux (VUR)
- Ureters enter bladder obliquely through detrusor (2–3 cm intramural course)
- Detrusor tone compresses ureter = natural antireflux valve
- If intramural segment too short → urine refluxes to kidney → recurrent UTI, hydronephrosis, renal scarring
- Grade I–V; treat with antibiotics → surgical reimplantation (Cohen/Politano-Leadbetter)
③ Neurogenic Bladder
| Lesion | Type | Features |
|---|---|---|
| UMN (above S2-4) | Spastic / Reflex bladder | Small capacity, detrusor overactivity, urge incontinence, high pressure |
| LMN (S2-4 / conus medullaris) | Flaccid / Autonomous bladder | Large residual volume, overflow incontinence, low pressure, retention |
④ Bladder Injuries
| Type | Cause | Feature |
|---|---|---|
| Intraperitoneal rupture | Blunt trauma to full bladder (dome ruptures) | Urine into peritoneum → peritonitis, ileus |
| Extraperitoneal rupture | Pelvic fracture lacerates anterolateral wall | Urine in retropubic / perivesical fat |
| Iatrogenic | Midline incision extended to pubis | Full bladder at risk if not displaced |
⑤ Bladder Carcinoma
- Most common: TCC / Urothelial carcinoma (~90%)
- Classic presentation: Painless haematuria
- Trigone = most common site
- Lymphatic spread: External iliac → Internal iliac → Para-aortic
- Schistosoma haematobium → Squamous cell carcinoma (calcification on X-ray / KUB)
- Risk factors: Smoking (#1), aniline dyes, cyclophosphamide (→ haemorrhagic cystitis → Ca), radiation
⑥ Vesical Fistulae
| Fistula | Cause | Hallmark |
|---|---|---|
| Vesicovaginal | Obstructed labour, gynae surgery | Continuous urinary incontinence per vagina |
| Vesicointestinal (colovesical) | Diverticular disease, Crohn's, colorectal Ca | Pneumaturia + fecaluria = pathognomonic |
| Vesicouterine | LSCS complication | Youssef's syndrome = cyclical haematuria + amenorrhoea |
| Urethrovaginal | Obstetric trauma | Positional incontinence into vagina |
⑦ Space of Retzius (Retropubic Space)
- Potential extraperitoneal space between pubic bones/rectus and anterior bladder wall
- Contains loose areolar tissue, fat, vesical venous plexus
- Used in: suprapubic cystostomy, radical prostatectomy, TVT for stress incontinence
- Retropubic haematoma after pelvic fracture fills this space
⑧ Cystoscopy Landmarks
- Trigone → smooth, pale, most common tumor/schistosomiasis site
- Ureteric orifices → slit-like; visible efflux of urine (peristaltic jets)
- Interureteric ridge → visible as transverse mucosal fold
- Uvula vesicae (male) → elevation above internal meatus (median lobe of prostate)
- Bladder dome/walls → rugae present when empty
⑨ TURBT Hazards
- Dome resection → risk of intraperitoneal perforation
- Lateral wall resection → obturator reflex (nerve stimulation → adductor spasm → bladder perforation)
- Managed by: obturator nerve block, low current cutting, saline distension (non-electrolyte)
13. MNEMONICS SUMMARY
| Mnemonic | Meaning |
|---|---|
| A Big Fat Neck | Apex, Body, Fundus, Neck |
| S2-3-4 keeps urine off the floor | Parasympathetic voiding via pelvic splanchnic |
| SIVA | Superior vesical, Inferior vesical, Vesical plexus, All from internal iliac |
| 2U + 1U = Trigone | 2 Ureteric orifices + 1 Urethral orifice |
| PCSD | Patent, Cyst, Sinus, Diverticulum (urachal remnants) |
| TCC SMOKES | TCC, Cyclophosphamide, Schistosomiasis, Male, painless haematuria, K=know trigone, External iliac nodes, Smoking |
| Ext. wall → Ext. nodes | Lateral walls → External iliac; Base → Internal iliac |
📌 Exam Tips:
- Trigone = smooth, no rugae, mesodermal origin, no muscularis mucosae
- Most fixed part = neck; most mobile = dome/apex
- Suprapubic puncture safe because peritoneum peels away from anterior wall when bladder is full
- Painless haematuria = bladder Ca until proven otherwise
- Pneumaturia = colovesical fistula (diverticular disease most common cause in adults)
- VUR = short intramural ureteric segment → loss of antireflux mechanism