
IMG_20260622_140553987.jpg
Solve
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Now I have all the material I need. Here are the complete, exam-ready answers:
ABVIMS & Dr. RML Hospital - OBG MBBS 3rd Year Exam Answers
Q1. Case: 34-year-old primigravida, 26 weeks gestation, 2-hr post 75g glucose = 190 mg/dL [25 marks]
Q1.1 - Probable Diagnosis [2 marks]
Gestational Diabetes Mellitus (GDM)
Using IADPSG (International Association of Diabetes and Pregnancy Study Groups) criteria - the cut-off for 2-hour post-load glucose after a 75g OGTT is ≥153 mg/dL. This patient's value of 190 mg/dL clearly exceeds this threshold, confirming GDM.
(Note: A random plasma glucose ≥200 mg/dL would indicate overt diabetes - this patient falls in the GDM range.)
Q1.2 - Diagnostic Tests for GDM [3 marks]
Two major screening/diagnostic approaches:
A. One-Step Approach (IADPSG/WHO - widely used internationally):
- Single 75g OGTT at 24-28 weeks (non-fasting not required, but fasting recommended)
- GDM diagnosed if ANY ONE value is met:
| Time point | Threshold |
|---|---|
| Fasting | ≥ 92 mg/dL |
| 1-hour post-load | ≥ 180 mg/dL |
| 2-hour post-load | ≥ 153 mg/dL |
B. Two-Step Approach (ACOG/US standard):
- Step 1: 50g Glucose Challenge Test (GCT) - non-fasting, 1-hour value ≥140 mg/dL is positive
- Step 2 (if GCT positive): 100g OGTT over 3 hours; GDM if 2 or more values are met (Carpenter-Coustan or NDDG criteria)
Additional investigations once GDM is diagnosed:
- HbA1c (if elevated >6.5%, suggests pre-existing diabetes)
- Fasting plasma glucose
- Urine for glucose/ketones
- Renal function tests (baseline)
- Ophthalmologic evaluation (if pre-existing diabetes suspected)
Q1.3 - Maternal and Fetal Complications [4 marks]
Maternal Complications:
| Short-term | Long-term |
|---|---|
| Preeclampsia / hypertension | T2DM (50% risk within 5-10 years) |
| Polyhydramnios | Recurrent GDM in future pregnancies |
| Increased risk of caesarean section | Cardiovascular disease |
| Urinary tract infections | Metabolic syndrome |
| Preterm labor | |
| Shoulder dystocia (due to macrosomia) | |
| HELLP syndrome | |
| Postpartum hemorrhage |
Fetal/Neonatal Complications:
| Fetal | Neonatal |
|---|---|
| Macrosomia (birth weight >4 kg) | Neonatal hypoglycemia |
| Intrauterine growth restriction (in poorly managed cases) | Respiratory distress syndrome (RDS) |
| Stillbirth | Neonatal hyperbilirubinemia (jaundice) |
| Congenital anomalies (if pre-existing DM) | Polycythemia |
| Fetal distress / asphyxia | Hypocalcemia, hypomagnesemia |
| Increased risk of obesity/T2DM in offspring | Birth injuries (clavicle fracture, brachial plexus injury) |
Q1.4 - Indications for Caesarean Section in GDM [4 marks]
GDM itself is not an absolute indication for CS, but the following are indications in this condition:
Obstetric indications specific to GDM:
- Macrosomia - Estimated fetal weight >4,500 g (some guidelines use >4,000 g with poor glycemic control) - prophylactic CS to prevent shoulder dystocia
- Previous caesarean section with macrosomic fetus
- Shoulder dystocia in previous delivery
- Cephalopelvic disproportion (CPD) - common due to large fetal size
- Failed induction of labor - GDM patients are often induced at 38-39 weeks; if labor fails to progress, CS is indicated
- Fetal distress intrapartum (non-reassuring CTG, abnormal FHR patterns)
- Malpresentation (breech, transverse lie) - more common with macrosomia/polyhydramnios
- Polyhydramnios causing cord prolapse or malpresentation
- Pre-eclampsia with severe features requiring immediate delivery with an unfavorable cervix
- Placenta previa (associated with GDM)
- Previous uterine surgery / classical CS scar
Q1.5 - Medical Nutrition Therapy (MNT) and Its Basic Principles [6 marks]
Definition:
Medical Nutrition Therapy is a structured dietary intervention prescribed and monitored by a registered dietitian/physician to manage blood glucose, provide adequate nutrition for fetal growth, and minimize maternal and neonatal complications in GDM.
Basic Principles of MNT in GDM:
-
Caloric requirements:
- Adequate calories to support fetal growth without promoting hyperglycemia
- Typically: 30-35 kcal/kg/day for normal BMI; 25 kcal/kg/day for overweight; 12-15 kcal/kg/day for obese women
- Total weight gain goal: 11-16 kg for normal BMI, 7-11 kg for overweight, 5-9 kg for obese
-
Carbohydrate restriction and distribution:
- Carbohydrates should constitute 33-40% of total calories (some guidelines: 40-45%)
- Carbohydrates are distributed across 3 main meals + 2-3 snacks to avoid postprandial glucose spikes
- Breakfast carbohydrates should be limited (15-30g) as insulin resistance is highest in the morning
- Emphasize complex carbohydrates with low glycemic index (whole grains, legumes, vegetables)
- Avoid simple sugars, refined carbohydrates, fruit juices, and sugar-sweetened beverages
-
Protein intake:
- 20% of total calories from protein
- Sources: lean meat, fish, eggs, legumes, dairy
-
Fat intake:
- 40% of total calories; emphasis on unsaturated fats
- Limit saturated fats and trans fats
-
Fiber:
- ≥28g/day recommended - slows glucose absorption, improves postprandial glycemia
-
Monitoring response:
- Blood glucose targets: Fasting <95 mg/dL, 1-hr postprandial <140 mg/dL, 2-hr postprandial <120 mg/dL
- Self-monitoring of blood glucose 4 times daily (fasting + post-meals)
- Urine ketones monitored to avoid starvation ketosis
-
Exercise:
- 30 minutes of moderate aerobic exercise (walking) after meals complements MNT
- Reduces insulin resistance and postprandial glucose levels
Q1.6 - Drugs Used to Treat GDM: Types, Onset, Duration [6 marks]
When MNT and lifestyle modification fail to achieve target glucose levels, pharmacotherapy is initiated.
A. INSULIN (Drug of Choice in GDM)
| Type | Drug | Onset of Action | Peak | Duration |
|---|---|---|---|---|
| Rapid-acting | Insulin Lispro (Humalog) | 15 min | 30-90 min | 3-5 hrs |
| Rapid-acting | Insulin Aspart (NovoLog) | 10-20 min | 40-50 min | 3-5 hrs |
| Short-acting (Regular) | Regular Insulin (Actrapid) | 30-60 min | 2-4 hrs | 5-8 hrs |
| Intermediate-acting | NPH (Isophane) Insulin | 1-3 hrs | 4-8 hrs | 12-18 hrs |
| Long-acting | Insulin Glargine (Lantus) | 2-4 hrs | Peakless | 20-24 hrs |
| Long-acting | Insulin Detemir (Levemir) | 1-2 hrs | 6-8 hrs | 17-24 hrs |
Use in GDM:
- Basal-bolus regimen: Long-acting insulin (glargine/detemir) once daily + rapid-acting (lispro/aspart) with meals
- NPH + Regular insulin: Twice-daily "split-mixed" regimen (still widely used)
- Insulin does NOT cross the placenta - hence safe for fetus
B. ORAL HYPOGLYCEMICS
Note: Use is controversial and off-label in many countries; not first-line in most guidelines, but used in some settings
| Drug | Class | Onset | Duration | Notes |
|---|---|---|---|---|
| Metformin | Biguanide | 2-3 hrs | 8-12 hrs | Crosses placenta; reasonable safety data; reduces insulin resistance; may be used when patient refuses insulin |
| Glyburide (Glibenclamide) | Sulfonylurea | 2-4 hrs | 16-24 hrs | Crosses placenta (fetal hypoglycemia risk); higher failure rate; not preferred by ACOG |
Starting thresholds for insulin: If fasting glucose consistently >95 mg/dL or 2-hr postprandial >120 mg/dL despite MNT for 1-2 weeks.
Q2. Short Notes [5 × 5 = 25 marks]
Q2.1 - POP-Q Classification for Prolapse [5 marks]
The Pelvic Organ Prolapse Quantification (POP-Q) system is the internationally standardized classification approved by the International Continence Society (ICS) for grading female pelvic organ prolapse.
Reference Point: The hymen is the fixed reference (= 0). Measurements proximal to the hymen are negative (-), distal are positive (+).
Nine Measurement Points:
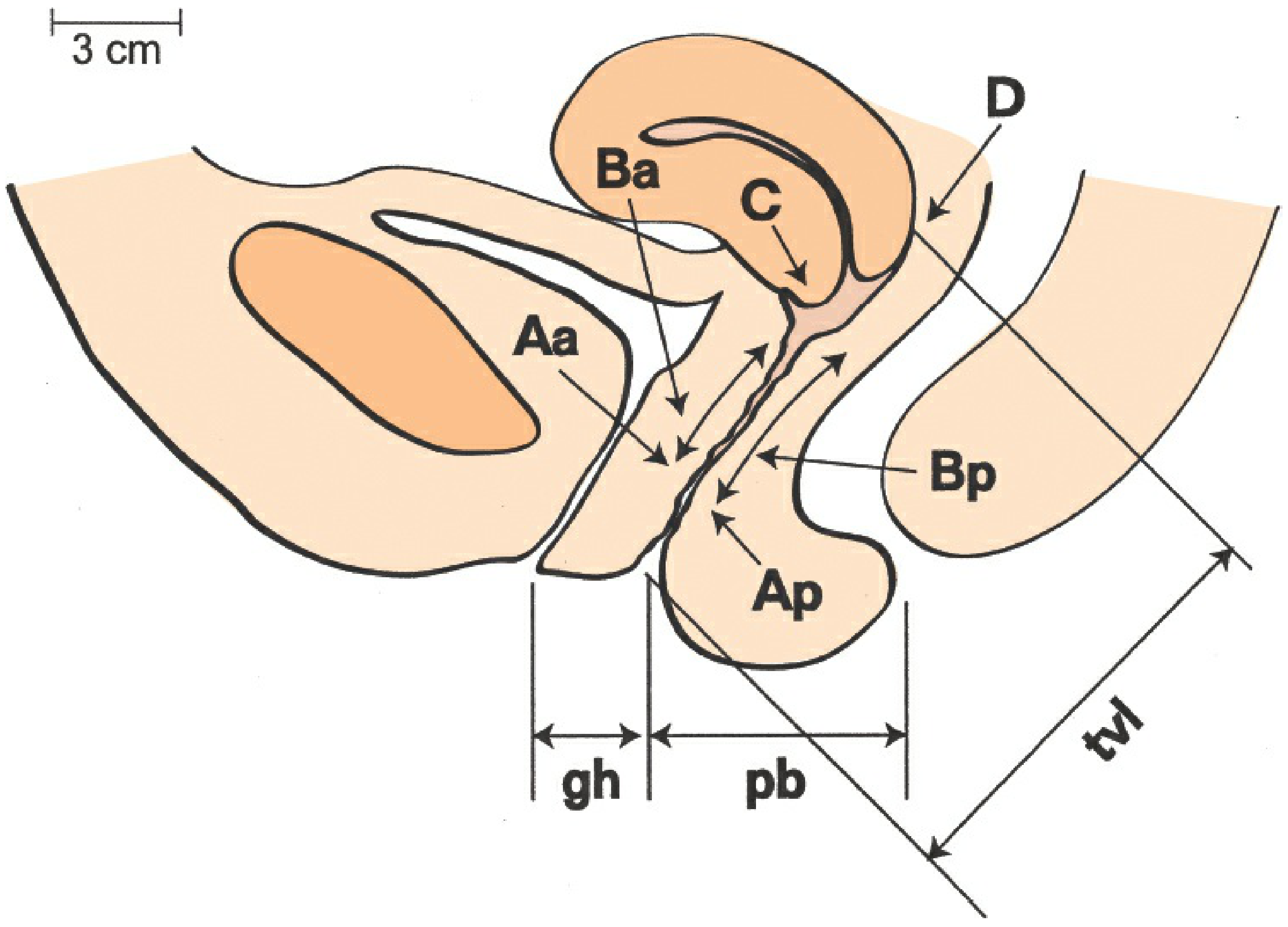
| Point | Location | Normal Value |
|---|---|---|
| Aa | Anterior vaginal wall, 3 cm proximal to external urethral meatus (bladder neck) | -3 cm |
| Ba | Most distal point of anterior vaginal wall (between Aa and cervix/cuff) | -3 cm |
| C | Cervix or vaginal cuff (post-hysterectomy) | Varies |
| D | Posterior fornix (omitted post-hysterectomy) | Varies |
| Ap | Posterior vaginal wall, 3 cm proximal to hymen | -3 cm |
| Bp | Most distal point of posterior vaginal wall (between Ap and cervix/cuff) | -3 cm |
| gh | Genital hiatus - from urethral meatus to posterior midline hymen | ~2-3 cm |
| pb | Perineal body - from posterior margin of gh to mid-anal opening | ~2-3 cm |
| tvl | Total vaginal length - greatest depth when apex is fully reduced | ~8-10 cm |
Staging (0 to IV):
| Stage | Description |
|---|---|
| Stage 0 | No prolapse; Aa, Ba, Ap, Bp all at -3 cm; C or D ≤ -(tvl-2) cm |
| Stage I | Most distal point of prolapse >1 cm above the hymen (< -1 cm) |
| Stage II | Most distal point within 1 cm of the hymen (-1 to +1 cm) |
| Stage III | Most distal point >1 cm below the hymen but protrudes less than (tvl-2) cm |
| Stage IV | Complete eversion/procidentia; most distal point ≥ (tvl-2) cm |
Advantages over older systems:
- Standardized, reproducible, quantitative measurements
- Multiple vaginal compartments assessed simultaneously
- Reference point (hymen) is constant and independent of patient position
- Can track disease progression accurately over time
Q2.2 - Clinical Presentations of Fibroid Uterus and Management [5 marks]
Uterine fibroids (leiomyomas) are the most common benign tumors of the uterus, arising from smooth muscle cells.
Classification by location:
- Submucosal - beneath endometrium, project into uterine cavity (most symptomatic)
- Intramural - within the myometrium (most common)
- Subserosal - beneath the serosa, project outward
- Pedunculated - attached by a stalk (submucosal or subserosal)
- Cervical - located in cervix
- Broad ligament (parasitic) - in broad ligament
Clinical Presentations:
-
Abnormal uterine bleeding (AUB):
- Most common symptom, especially with submucosal fibroids
- Menorrhagia (heavy, prolonged periods), metrorrhagia
- Secondary iron-deficiency anemia, fatigue, pallor
-
Pelvic pressure/pain:
- Heaviness, dragging sensation in pelvis
- Dysmenorrhea (painful periods)
- Acute pain - torsion of pedunculated fibroid, red degeneration (in pregnancy)
- Chronic pelvic pain
-
Pressure symptoms:
- Urinary: Frequency, urgency, retention, hydroureter (anterior fibroid pressing on bladder)
- Bowel: Constipation, tenesmus (posterior fibroid pressing on rectum)
-
Infertility and reproductive problems:
- Submucosal fibroids distort the uterine cavity and impair implantation
- Recurrent miscarriage
- Obstruction of fallopian tube ostia
-
Abdominal mass:
- Firm, irregular, non-tender enlarged uterus palpable abdominally when fibroids are large
-
Pregnancy complications:
- Red degeneration (carneous degeneration) - acute painful episode in pregnancy
- Malpresentation, obstructed labor
- Postpartum hemorrhage
Management:
A. Conservative (Asymptomatic / small fibroids):
- Regular monitoring with pelvic ultrasound every 6-12 months
- Observation especially in perimenopausal women (fibroids shrink after menopause)
B. Medical Management:
- GnRH agonists (Leuprolide, Goserelin): Reduce fibroid size by 30-50%; used preoperatively; max 6 months (bone loss risk)
- Progesterone receptor modulators (Ulipristal acetate): Reduces bleeding and fibroid size
- Levonorgestrel IUS (Mirena): Controls menorrhagia with intramural/small submucosal fibroids
- Combined OCP / progestins: Control bleeding, not fibroid size
- Tranexamic acid / NSAIDs: Symptomatic relief of menorrhagia/dysmenorrhea
- Iron supplementation: For anemia
C. Surgical Management:
- Myomectomy (fibroid removal with uterine preservation): For women desiring future fertility; can be done hysteroscopically (submucosal), laparoscopically, or via laparotomy
- Hysterectomy (definitive cure): For women who have completed childbearing with severe symptoms
- Hysteroscopic resection: Best for submucosal fibroids (type 0, 1, 2)
D. Minimally Invasive / Radiological:
- Uterine Artery Embolization (UAE): Blocks blood supply to fibroids; good for symptomatic women who want to avoid surgery; not recommended if future fertility is desired
- MRI-guided Focused Ultrasound (MRgFUS): Non-invasive ablation; suitable for selected cases
Q2.3 - Eclampsia Management [5 marks]
Definition: Eclampsia is the occurrence of grand mal seizures in a woman with preeclampsia, not attributable to other causes.
Immediate Management (ABC approach):
Step 1 - Secure Airway and Prevent Injury:
- Place patient in left lateral position
- Padded side-rails; bite block if safe
- Suction oropharynx; administer oxygen (6-8 L/min by face mask)
- Establish IV access (two large-bore IVs)
Step 2 - Control Seizures (MAGNESIUM SULFATE - drug of choice):
- Loading dose: 4-6 g IV in 100 mL normal saline over 15-20 minutes
- Maintenance dose: 2 g/hour by IV infusion
- Monitor for magnesium toxicity (check every 1-2 hours):
- Urine output >25 mL/hr (must be maintained)
- Patellar/knee reflexes present (lost at ~7-10 mg/dL)
- Respiratory rate >12/min (depression at ~12 mg/dL)
- Serum Mg2+ if needed (therapeutic range: 4-7 mg/dL)
- Antidote for Mg toxicity: Calcium gluconate 1g IV slowly
If seizures recur despite magnesium: Additional 2g Mg bolus IV; alternatively diazepam, phenytoin, or thiopentone
Step 3 - Control Hypertension:
- Target: systolic <160 mmHg, diastolic <105 mmHg
- Hydralazine: 5-10 mg IV push, repeat every 20-30 min (first-line)
- Labetalol: 20 mg IV bolus, repeat every 10 min up to 300 mg total
- Nifedipine: 10-20 mg oral (sublingual avoided - precipitous drop)
- Avoid diuretics and hyperosmotic agents (worsen intravascular depletion)
Step 4 - Investigations:
- CBC, platelet count (rule out HELLP syndrome)
- LFTs, serum creatinine, uric acid
- Urine protein (24-hr or spot protein:creatinine ratio)
- Coagulation profile (PT, aPTT, fibrinogen)
- CT head if: decreased consciousness, persistent seizures, lateralizing signs
- Fetal monitoring: CTG, BPP, Doppler
Step 5 - Fluid Management:
- Restrict IV fluids to 80-100 mL/hr (oliguria expected; avoid pulmonary edema)
- Maintain urine output >25-30 mL/hr
- Foley catheter for strict I/O monitoring
Step 6 - Delivery (Definitive Treatment):
- Eclampsia at any gestational age is an indication for delivery
- Stabilize patient first (seizure control, BP control)
- Mode of delivery: vaginal delivery preferred if cervix is favorable; CS for obstetric indications
- After delivery: continue Mg sulfate for at least 24-48 hours postpartum
Postpartum care:
- Continue antihypertensives as needed
- Watch for late postpartum eclampsia (up to 4 weeks)
- Counsel about recurrence risk (25% in subsequent pregnancies)
Q2.4 - Balloon Tamponade [5 marks]
Definition: Balloon tamponade is a mechanical, minimally invasive method used to control postpartum hemorrhage (PPH) by inserting an inflatable balloon into the uterine cavity to exert direct pressure on bleeding sinusoids.
Principle: Applies intrauterine pressure exceeding the arterial perfusion pressure, thereby tamponading bleeding vessels - particularly effective for uterine atony (most common cause of PPH).
Indications:
- Uterine atony not responding to uterotonics (oxytocin, ergometrine, carboprost)
- Low-lying placenta / placenta previa with bleeding after delivery
- Step-up in conservative PPH management (after uterotonics, before surgical intervention)
- "Tamponade test" - if balloon controls bleeding, avoids need for surgery/embolization
Types of Balloons:
| Device | Capacity | Notes |
|---|---|---|
| Bakri balloon | Up to 500-800 mL | Purpose-designed for PPH; has drainage channel to monitor ongoing bleeding |
| BT-Cath (Balloon Tamponade Catheter) | Up to 500 mL | Dual-channel design |
| Sengstaken-Blakemore tube | Modified use | Originally for esophageal varices |
| Condom catheter | Variable | Low-cost improvised device; widely used in resource-limited settings (e.g., condom tied over Foley catheter) |
| Foley catheter | 30-80 mL | For minor bleeding, especially at lower segment/placenta bed |
Procedure (Bakri Balloon):
- Examine for lacerations and repair them first
- Insert balloon transcervically into uterine cavity under ultrasound guidance
- Inflate with warm normal saline (typically 250-500 mL) until bleeding stops ("tamponade test")
- Leave inflated for 12-24 hours
- Oxytocin infusion continued during balloon placement
- Deflate gradually after 12-24 hours; monitor for rebleeding
- If tamponade test negative (bleeding continues despite inflation) - proceed to surgical intervention (B-Lynch suture, devascularization, or hysterectomy)
Advantages:
- Simple, quick, does not require general anesthesia
- Preserves uterus and fertility
- Buys time for resuscitation, transfer, or arranging definitive care
- Effective in 70-90% of uterine atony cases
Contraindications:
- Infection / chorioamnionitis (relative)
- Uterine rupture (primary surgical repair needed)
- Cervical/vaginal lacerations (must be repaired first)
Part of the "HAEMOSTASIS" stepwise algorithm: Balloon tamponade comes after uterotonics and before surgical steps.
Q2.5 - Management of HIV-Positive Mother During Labour [5 marks]
The goals of management are: prevent mother-to-child transmission (MTCT), protect healthcare workers, and ensure safe delivery for mother and baby.
MTCT occurs in 3 phases: Antepartum (25%), intrapartum (60-70%), postpartum via breastfeeding (15%).
A. Antiretroviral Therapy (ART) During Labour:
-
All HIV-positive pregnant women should be on combination ART (cART) throughout pregnancy, labor, and postpartum (regardless of CD4 count) - "Option B+" (WHO recommendation)
-
Standard regimen: TDF (Tenofovir) + 3TC (Lamivudine) + EFV (Efavirenz) - continued throughout labor
-
If woman presents in labor NOT on ART (unbooked case):
- Give single-dose Nevirapine (sdNVP) 200 mg orally immediately
- Add AZT (Zidovudine) + 3TC orally during labor
- Continue postpartum ART
-
If woman has high viral load (>1000 copies/mL) at time of delivery despite ART:
- IV Zidovudine infusion during labor (loading 2 mg/kg over 1 hr, then 1 mg/kg/hr until delivery) - recommended in some guidelines for high VL
B. Mode of Delivery:
- Vaginal delivery is acceptable if: woman is on effective cART with viral load <50-200 copies/mL (undetectable) near term
- Elective Caesarean section at 38 weeks is recommended if:
- Viral load >1000 copies/mL near term
- Not on ART / late presentation
- Coinfection with Hepatitis C (increases transmission risk)
- Previous infant with HIV infection
C. Intrapartum Precautions:
- Minimize invasive procedures: Avoid fetal scalp electrodes, fetal blood sampling, artificial rupture of membranes (ARM) unless essential
- If ARM required, delay as long as possible - prolonged rupture of membranes (>4 hours) increases MTCT risk
- Avoid episiotomy unless absolutely necessary
- Forceps/vacuum delivery: Use only for standard obstetric indications; instrumentation increases infant exposure to maternal blood
- Universal precautions for all healthcare staff: double gloves, eye protection, safe sharps disposal
D. Third Stage Management:
- Active management of third stage (oxytocin IM/IV) - standard
- Ergometrine: caution with Protease Inhibitors (drug interaction - vasoconstriction); oxytocin preferred
E. Neonatal Prophylaxis (immediately after birth):
- NVP syrup for the neonate: 2 mg/kg once daily for 6 weeks (standard prophylaxis)
- If mother had undetectable viral load: 4 weeks NVP or AZT for neonate
- If mother had high VL or no ART: Dual/Triple ART prophylaxis for neonate for 6 weeks
F. Infant Feeding:
- In resource-rich settings: Avoid breastfeeding completely (formula feeding); eliminates postpartum transmission
- In resource-limited settings (per WHO): Exclusive breastfeeding for 6 months with maternal ART (safer than mixed feeding); NVP prophylaxis for infant throughout breastfeeding
- Virological testing of infant at: birth, 6 weeks, 6 months, and 18 months
G. Postpartum:
- Continue maternal ART indefinitely (lifelong)
- Contraception counseling
- Screen for postnatal depression
- HIV testing of partner
Sources: Creasy & Resnik's Maternal-Fetal Medicine (9780323828499); Berek & Novak's Gynecology (9781496380357); Rosen's Emergency Medicine (9780323757898); Sabiston Textbook of Surgery (9780443124341)
Reload
I'm ready! How can I help you?
Solve again
Here are the complete answers to the ABVIMS & Dr. RML Hospital OBG exam paper:
Q1. 34-year-old Primigravida, 26 weeks, 2-hr post 75g glucose = 190 mg/dL [25 marks]
Q1.1 - Probable Diagnosis [2 marks]
Gestational Diabetes Mellitus (GDM)
By IADPSG criteria, the 2-hour post-load glucose after a 75g OGTT cut-off for GDM is ≥153 mg/dL. This patient's value of 190 mg/dL clearly exceeds this, confirming GDM. (Overt diabetes would require ≥200 mg/dL random or fasting ≥126 mg/dL.)
Q1.2 - Diagnostic Tests for GDM [3 marks]
One-Step Approach (IADPSG/WHO - recommended internationally & in India)
A single 75g OGTT at 24-28 weeks - GDM is diagnosed if ANY ONE value is met:
| Time Point | Threshold |
|---|---|
| Fasting | ≥ 92 mg/dL |
| 1-hour post-load | ≥ 180 mg/dL |
| 2-hour post-load | ≥ 153 mg/dL |
If any value meets the criteria for overt diabetes (fasting ≥126, 2-hr ≥200, random ≥200), it is classified as overt diabetes in pregnancy, not GDM.
Two-Step Approach (ACOG - USA)
- Step 1: 50g Glucose Challenge Test (GCT), non-fasting; if 1-hr value ≥140 mg/dL → proceed to Step 2
- Step 2: 100g 3-hour OGTT; GDM diagnosed if ≥2 values are abnormal (Carpenter-Coustan criteria: Fasting ≥95, 1-hr ≥180, 2-hr ≥155, 3-hr ≥140 mg/dL)
Additional Investigations (after diagnosis)
- HbA1c: If ≥6.5%, suggests pre-existing (pregestational) diabetes
- Fasting plasma glucose
- Urine glucose and ketones
- Renal function tests (baseline)
- Fundoscopy (if pre-existing DM suspected)
Q1.3 - Maternal and Fetal Complications [4 marks]
Maternal Complications
| Short-term | Long-term |
|---|---|
| Pre-eclampsia / hypertension | Type 2 DM (50% risk within 5-10 years) |
| Polyhydramnios | Recurrent GDM in future pregnancies |
| Increased caesarean rate | Metabolic syndrome |
| Urinary tract infections | Cardiovascular disease |
| Shoulder dystocia | |
| Postpartum hemorrhage | |
| Wound infection |
Fetal and Neonatal Complications
| Fetal | Neonatal |
|---|---|
| Macrosomia (birth wt >4 kg) - most common | Neonatal hypoglycemia |
| Intrauterine fetal death / stillbirth | Respiratory distress syndrome (RDS) |
| Congenital malformations (if pre-existing DM) | Neonatal hyperbilirubinemia (jaundice) |
| IUGR (in vascular disease) | Polycythemia |
| Fetal distress / birth asphyxia | Hypocalcemia, hypomagnesemia |
| Malpresentation (due to polyhydramnios) | Birth injuries - clavicle fracture, Erb's palsy |
| Long-term: obesity and T2DM in offspring |
Q1.4 - Indications for Caesarean Section in GDM [4 marks]
GDM is not an absolute indication for CS, but the following situations in GDM mandate or strongly indicate it:
- Macrosomia - Estimated fetal weight >4,500g (some use >4,000g with poor glycemic control) to prevent shoulder dystocia
- Cephalopelvic disproportion (CPD) - common due to fetal macrosomia
- Failed induction of labor - GDM patients are often induced at 38-39 weeks; failure to progress warrants CS
- Fetal distress - non-reassuring CTG, late decelerations, abnormal biophysical profile
- Malpresentation - breech, transverse lie (more common with polyhydramnios/macrosomia)
- Previous CS with large baby or unfavorable conditions for VBAC
- Placenta previa (associated with GDM/obesity)
- Pre-eclampsia with severe features requiring urgent delivery with unfavorable cervix
- Cord prolapse (due to polyhydramnios)
- Previous shoulder dystocia or birth injury in prior pregnancy
- Maternal indications - severe uncontrolled DM with end-organ disease
Q1.5 - Medical Nutrition Therapy (MNT): Definition and Basic Principles [6 marks]
Definition
Medical Nutrition Therapy is a structured, individualized dietary intervention prescribed and monitored by a physician/registered dietitian to achieve target blood glucose levels, provide adequate nutrition for fetal growth, and prevent maternal and neonatal complications in GDM - without causing starvation ketosis.
Basic Principles
1. Caloric Requirements
- Normal BMI: 30-35 kcal/kg ideal body weight/day
- Overweight (BMI 25-29.9): 25 kcal/kg/day
- Obese (BMI ≥30): 12-15 kcal/kg/day (caloric restriction to 1,600-1,800 kcal/day)
- Minimum 1,800 kcal/day recommended in most guidelines to avoid ketosis
- Total gestational weight gain goal: 11-16 kg (normal BMI), 7-11 kg (overweight), 5-9 kg (obese)
2. Carbohydrate Restriction and Distribution
- Carbohydrates: 33-40% of total daily calories (max 45%)
- Distribute across 3 main meals + 2-3 snacks to prevent postprandial spikes
- Breakfast carbs should be lowest (15-30g) - insulin resistance is maximal in the morning
- Choose complex carbs with low glycemic index: whole grains, legumes, vegetables, oats
- Strictly avoid: simple sugars, refined flour, fruit juices, sugar-sweetened beverages, white rice
3. Protein
- 20% of total calories from protein
- Sources: lean meats, fish, eggs, pulses, low-fat dairy
4. Fat
- 40% of total calories; favor monounsaturated and polyunsaturated fats
- Limit saturated fats and eliminate trans fats
5. Dietary Fiber
- ≥28g/day recommended
- Slows glucose absorption, reduces postprandial glycemia, improves satiety
6. Blood Glucose Monitoring Targets
- Fasting: <95 mg/dL
- 1-hour postprandial: <140 mg/dL
- 2-hour postprandial: <120 mg/dL
- Self-monitoring 4 times daily (fasting + after each meal)
- Urine ketones checked daily (morning) to detect starvation ketosis
7. Timing and Frequency of Meals
- Never skip meals; regular intervals (every 3-4 hours)
- Bedtime snack (25g carbs + protein) to prevent overnight fasting hypoglycemia and ketosis
8. Exercise as Adjunct
- 30 minutes of brisk walking or moderate aerobic exercise after meals
- Reduces postprandial glucose and insulin resistance
Q1.6 - Drugs for GDM: Types, Onset, Duration [6 marks]
Pharmacotherapy is started when MNT fails to achieve targets for 1-2 weeks.
A. INSULIN - Drug of Choice in GDM
Insulin does not cross the placenta at therapeutic doses - it is the safest option.
| Category | Drug | Onset | Peak | Duration |
|---|---|---|---|---|
| Ultra-rapid acting | Insulin Lispro (Humalog) | 5-15 min | 30-90 min | 3-5 hours |
| Ultra-rapid acting | Insulin Aspart (NovoLog) | 10-20 min | 40-50 min | 3-5 hours |
| Short-acting (Regular) | Regular Insulin (Actrapid/Humulin R) | 30-60 min | 2-4 hours | 5-8 hours |
| Intermediate-acting | NPH / Isophane Insulin (Humulin N) | 1-3 hours | 4-8 hours | 12-18 hours |
| Long-acting | Insulin Glargine (Lantus) | 2-4 hours | Peakless (flat) | 20-24 hours |
| Long-acting | Insulin Detemir (Levemir) | 1-2 hours | 6-8 hours | 17-24 hours |
Common regimens in GDM:
- Twice-daily split-mixed: NPH + Regular (morning and evening) - widely used in India
- Basal-bolus: Long-acting (Glargine once daily) + Rapid-acting (Lispro/Aspart before meals)
- Insulin doses are adjusted based on blood glucose logs
B. ORAL HYPOGLYCEMIC AGENTS (off-label/second-line in most guidelines)
| Drug | Class | Mechanism | Onset | Duration | Key Note |
|---|---|---|---|---|---|
| Metformin | Biguanide | Reduces hepatic glucose production, improves insulin sensitivity | 2-3 hrs | 8-12 hrs | Crosses placenta; reasonable safety data; used when patient refuses insulin; may be used as adjunct |
| Glyburide (Glibenclamide) | Sulfonylurea (2nd gen) | Stimulates pancreatic insulin secretion | 2-4 hrs | 16-24 hrs | Crosses placenta - neonatal hypoglycemia risk; higher failure rate; NOT preferred by ACOG; rarely used now |
Threshold to initiate pharmacotherapy:
- Fasting glucose consistently >95 mg/dL, OR
- 2-hr postprandial consistently >120 mg/dL despite 1-2 weeks of MNT
Q2. Short Notes [5 × 5 = 25 marks]
Q2.1 - POP-Q Classification for Prolapse [5 marks]
The Pelvic Organ Prolapse Quantification (POP-Q) system is the standardized classification approved by the International Continence Society (ICS) for quantifying female pelvic organ prolapse.
Reference Point
The hymen is the fixed anatomical landmark (= 0 cm). Points proximal to hymen = negative values; points distal to hymen = positive values. All measurements taken at maximal Valsalva (straining), except total vaginal length.
The 9 Measurement Points
| Point | Compartment | Location | Normal Value |
|---|---|---|---|
| Aa | Anterior | 3 cm proximal to external urethral meatus (= bladder neck) | -3 cm |
| Ba | Anterior | Most distal point of anterior vaginal wall (Aa to cervix/cuff) | -3 cm |
| C | Apical | Leading edge of cervix (or vaginal cuff post-hysterectomy) | Variable |
| D | Apical | Posterior fornix / pouch of Douglas (omitted post-hysterectomy) | Variable |
| Ap | Posterior | 3 cm proximal to hymen on posterior vaginal wall | -3 cm |
| Bp | Posterior | Most distal point of posterior wall (Ap to cervix/cuff) | -3 cm |
| gh | - | Genital hiatus: mid-urethral meatus to posterior midline hymen | ~2-3 cm |
| pb | - | Perineal body: posterior margin of gh to mid-anal opening | ~2-3 cm |
| tvl | - | Total vaginal length: greatest depth with apex fully reduced | ~8-10 cm |
POP-Q Staging (based on most advanced point of prolapse)
| Stage | Criteria |
|---|---|
| Stage 0 | No prolapse; all points at -3 cm; C/D ≤ -(tvl-2) cm |
| Stage I | Most distal point > 1 cm above hymen (< -1 cm) |
| Stage II | Most distal point within 1 cm of hymen (-1 to +1 cm) |
| Stage III | Most distal point > 1 cm below hymen but < (tvl-2) cm |
| Stage IV | Complete eversion; most distal point ≥ (tvl-2) cm |
Advantages Over Older Systems (Baden-Walker)
- Quantitative, reproducible measurements at a fixed reference point (hymen)
- Assesses all three vaginal compartments simultaneously
- Can track progression over time and in research studies
- Standardized across centers globally
Q2.2 - Clinical Presentations of Fibroid Uterus and Management [5 marks]
Uterine fibroids (leiomyomas) are the most common benign smooth muscle tumors of the uterus.
Types by Location
- Submucosal (beneath endometrium - most symptomatic for bleeding)
- Intramural (within myometrium - most common)
- Subserosal (beneath uterine serosa - pressure symptoms)
- Pedunculated (on a stalk - torsion risk)
- Cervical and Broad ligament (parasitic)
Clinical Presentations
1. Abnormal Uterine Bleeding (AUB)
- Menorrhagia (heavy, prolonged periods) - especially submucosal fibroids
- Metrorrhagia, intermenstrual spotting
- Secondary iron-deficiency anemia (fatigue, pallor, dyspnea)
2. Pelvic Pain and Pressure
- Heaviness, dragging pelvic discomfort
- Dysmenorrhea
- Acute pain: torsion of pedunculated fibroid, red (carneous) degeneration in pregnancy (most common cause of acute pain with fibroids in pregnancy)
3. Pressure Symptoms
- Anterior fibroids: urinary frequency, urgency, incomplete voiding, retention
- Posterior fibroids: constipation, tenesmus
- Large fibroids: venous compression causing lower limb edema, varicosities
4. Abdominal Mass
- Hard, irregular, non-tender, mobile uterine mass palpable abdominally when fibroids are large (>12-14 weeks size)
5. Infertility and Pregnancy Loss
- Submucosal fibroids distort the cavity, impair implantation, and cause recurrent miscarriage
- Intramural fibroids may obstruct tubal ostia
6. Complications in Pregnancy
- Malpresentation (breech, transverse), obstructed labor
- Preterm labor, IUGR, placental abruption
- PPH (uterine atony from large fibroids)
Management
A. Conservative / Expectant
- Asymptomatic fibroids, small size, perimenopausal women (fibroids regress after menopause)
- 6-12 monthly ultrasound surveillance
B. Medical
| Drug | Mechanism | Use |
|---|---|---|
| GnRH agonists (Leuprolide, Goserelin) | Hypo-oestrogenic state; shrinks fibroid 30-50% | Pre-op to reduce size; max 6 months |
| Progesterone receptor modulators (Ulipristal acetate) | Reduces bleeding + fibroid size | Intermittent medical treatment |
| Levonorgestrel IUS (Mirena) | Local progestogen; reduces bleeding | For menorrhagia with small/intramural fibroids |
| Combined OCP / Progestins | Reduce menstrual flow | Symptomatic relief only |
| Tranexamic acid, NSAIDs | Antifibrinolytic; antiprostaglandin | Acute menorrhagia control |
| Iron supplementation | Corrects anemia | Adjunct |
C. Surgical
- Hysteroscopic myomectomy: Submucosal fibroids (FIGO type 0, 1, 2) - preserves uterus; best for fertility
- Laparoscopic myomectomy: Small-medium intramural/subserosal fibroids - minimally invasive
- Open myomectomy (laparotomy): Large, multiple, or deep intramural fibroids; fertility preserving
- Hysterectomy: Definitive cure; for women who have completed family; total abdominal, vaginal, or laparoscopic
D. Minimally Invasive / Interventional Radiology
- Uterine Artery Embolization (UAE): Occludes uterine arteries; 85-90% success for symptom control; not for those desiring fertility
- MRI-guided Focused Ultrasound (MRgFUS): Non-invasive thermal ablation; suitable for selected symptomatic fibroids
Q2.3 - Eclampsia Management [5 marks]
Definition: Grand mal seizures in a woman with pre-eclampsia, not attributable to other causes (epilepsy, hypoglycemia, etc.)
Immediate Steps (ABCDE)
Step 1 - Airway and Safety
- Left lateral position (reduces aspiration, relieves aortocaval compression)
- Airway secured; oxygen 8-10 L/min by face mask
- Suction oropharynx; padded side-rails
- IV access - two large-bore cannulas
Step 2 - Terminate Seizures: MAGNESIUM SULFATE (Drug of Choice)
- Loading dose: 4-6g IV in 100 mL NS over 15-20 minutes
- Maintenance: 2g/hour by continuous IV infusion
- Continue for 24-48 hours after delivery or last seizure (whichever is later)
Monitoring for Mg toxicity (every 1-2 hours):
| Parameter | Action |
|---|---|
| Urine output | Must be >25 mL/hr; if <25 mL/hr, reduce infusion |
| Patellar reflexes | Must be present; loss occurs at Mg ~7-10 mg/dL |
| Respiratory rate | Must be >12/min; depression at Mg ~12 mg/dL |
| Serum Mg | Therapeutic range: 4-7 mg/dL |
Antidote: Calcium gluconate 1g IV slowly (over 10 min) for toxicity
Recurrent seizures: Additional 2g Mg IV bolus; or diazepam 10mg IV; or phenytoin
Step 3 - Control Blood Pressure
- Target: systolic <160 mmHg, diastolic <105-110 mmHg
- Hydralazine: 5-10 mg IV, repeat every 20-30 min (first-line parenteral)
- Labetalol: 20 mg IV bolus, double dose every 10 min (max 300 mg total)
- Nifedipine: 10-20 mg oral, repeat in 30 min if needed (oral only - not sublingual)
- Avoid diuretics (worsen intravascular volume depletion)
Step 4 - Investigations
- CBC, platelets (rule out HELLP: H-hemolysis, EL-elevated liver enzymes, LP-low platelets)
- LFTs, serum creatinine, uric acid
- Coagulation profile (PT, aPTT, fibrinogen)
- 24-hr urine protein
- CTG + BPP for fetal wellbeing
- CT head if: prolonged unconsciousness, focal neurological signs, recurrent seizures
Step 5 - Fluid Management
- Restrict to 80-100 mL/hr total IV fluid input
- Foley catheter; strict intake-output monitoring
- Maintain urine output >25-30 mL/hr
Step 6 - Delivery (Definitive Treatment)
- Eclampsia at ANY gestational age = indication for delivery after stabilization
- Vaginal delivery preferred if cervix is favorable and maternal/fetal condition stable
- CS for standard obstetric indications
- Continue Mg sulfate through labor and for 24-48 hours postpartum
Postpartum:
- Antihypertensives continued (methyldopa, labetalol, nifedipine)
- Watch for late postpartum eclampsia (up to 4 weeks post-delivery)
- Counseling: 25% recurrence risk in subsequent pregnancies; long-term cardiovascular risk
Q2.4 - Balloon Tamponade [5 marks]
Definition
Balloon tamponade is a minimally invasive, uterus-preserving mechanical method to control postpartum hemorrhage (PPH) by placing an inflatable balloon in the uterine cavity to exert direct hydrostatic pressure on bleeding sinusoids.
Principle
The inflated balloon generates intrauterine pressure exceeding the local arterial perfusion pressure, physically tamponading the bleeding vessels - most effective for uterine atony (responsible for 80% of PPH).
Indications
- Uterine atony not controlled by uterotonics (oxytocin, ergometrine, carboprost, misoprostol)
- PPH secondary to placenta previa / low-lying placenta (after placenta delivered)
- Placenta accreta spectrum (temporizing measure)
- As a "tamponade test": if balloon controls bleeding, avoids need for surgical/radiological intervention
- Step in the stepwise management of PPH (after uterotonics, before B-Lynch/hysterectomy)
Types of Balloon Devices
| Device | Fill Volume | Feature |
|---|---|---|
| Bakri balloon | Up to 500-800 mL | Purpose-designed; drainage channel monitors ongoing bleeding |
| BT-Cath | Up to 500 mL | Dual-channel system |
| Sengstaken-Blakemore tube | Modified use | Original use: esophageal varices; used in emergency |
| Condom catheter | Variable | Low-cost, widely used in resource-limited settings (condom tied to Foley catheter) |
| Foley catheter balloon | 30-80 mL | For minor lower segment bleeding |
Procedure (Bakri Balloon)
- Inspect and repair all cervical and vaginal lacerations first
- Insert balloon into uterine cavity transcervically (manual or under ultrasound guidance)
- Inflate with warm normal saline (typically 250-500 mL, guided by cessation of bleeding)
- Tamponade test: if bleeding stops = tamponade successful; if persists = surgical step needed
- Secure catheter to thigh; leave inflated for 12-24 hours
- Continue oxytocin infusion while balloon is in situ
- Uterine compression sutures + balloon together = "uterine sandwich" (for atony)
- Deflate gradually under observation; monitor for rebleeding
Advantages
- Quick, simple; no general anesthesia needed
- Preserves uterus and future fertility
- Effective in 70-90% of uterine atony cases
- Buys time for resuscitation, transfer, or definitive care
- Can be used at peripheral centers while awaiting transfer
Contraindications
- Uterine rupture (needs immediate surgical repair)
- Uterine infection / chorioamnionitis (relative)
- Must repair lacerations before placement
Place in the HAEMOSTASIS Algorithm
H-Ask for help | A-Assess, resuscitate | E-Establish etiology | M-Massage uterus | O-Oxytocin infusion | S-Shift to theatre | T-Tamponade balloon | A-Apply sutures (B-Lynch) | S-Systematic pelvic devascularization | I-Interventional radiology | S-Subtotal/total hysterectomy
Q2.5 - Management of HIV-Positive Mother During Labour [5 marks]
The three goals are: prevent mother-to-child transmission (MTCT), ensure safe delivery, and protect healthcare workers.
MTCT risk breakdown:
- Antenatal: 25% | Intrapartum: 60-70% (highest risk) | Postnatal (breastfeeding): 15%
- Without any intervention: MTCT rate ~25-45%; with optimal ART: <1-2%
A. Antiretroviral Therapy (ART) During Labour
Women already on ART (Option B+):
- Continue combination ART (cART) throughout labor: standard regimen = TDF + 3TC + EFV (Tenofovir + Lamivudine + Efavirenz) - taken orally
- Do NOT stop ART at any point during labor
Woman presents in labor WITHOUT prior ART (unbooked):
- Give single-dose Nevirapine (sdNVP) 200 mg orally immediately
- Add AZT (Zidovudine) 300 mg + 3TC (Lamivudine) 150 mg orally at onset of labor
- Initiate lifelong cART postpartum
Woman with high viral load (>1,000 copies/mL) despite ART:
- Consider IV Zidovudine infusion: loading 2 mg/kg over 1 hour, then 1 mg/kg/hour until delivery
B. Mode of Delivery
| Viral Load Status | Recommended Mode |
|---|---|
| Undetectable (<50-200 copies/mL) on cART | Vaginal delivery acceptable |
| VL >1,000 copies/mL at 36 weeks | Elective CS at 38 weeks |
| Not on ART / late booking | Elective CS at 38 weeks |
| Coinfection with Hepatitis C | Elective CS (increased transmission risk) |
C. Intrapartum Precautions
- Minimize invasive procedures that expose baby to maternal blood:
- Avoid fetal scalp electrode (FSE), fetal blood sampling (FBS)
- Avoid artificial rupture of membranes (ARM) unless essential - prolonged ROM >4 hours increases MTCT
- If ARM needed, perform as close to delivery as possible
- Avoid episiotomy unless absolutely necessary
- Instrumental delivery (forceps/vacuum): only for standard obstetric indications; minimize time
- Universal precautions for all staff: double gloves, eye protection, face shield, safe sharps disposal
D. Third Stage
- Oxytocin preferred over ergometrine (ergometrine interacts with protease inhibitors - severe vasoconstriction risk)
- Active management of third stage otherwise standard
E. Neonatal Prophylaxis (immediately post-delivery)
| Maternal Status | Neonatal Prophylaxis |
|---|---|
| On ART, undetectable VL | NVP syrup 2 mg/kg once daily for 4-6 weeks |
| Not on ART / high VL | Dual/triple ART for infant: AZT + NVP for 6 weeks |
| Unknown HIV status | Test mother stat; treat infant empirically if high risk |
Baby should be bathed immediately after delivery to remove maternal blood/secretions.
F. Infant Feeding
- Resource-rich settings: Complete avoidance of breastfeeding; exclusive formula feeding (eliminates postnatal MTCT)
- Resource-limited settings (WHO): Exclusive breastfeeding for 6 months with maternal cART + infant NVP prophylaxis (safer than mixed feeding)
- Never mix breastfeeding and formula ("mixed feeding" greatly increases transmission risk)
G. Infant Follow-up
- HIV virological testing (PCR): at birth, 6 weeks, 6 months, 18 months
- If any test positive: start infant on cART immediately
H. Postpartum Maternal Care
- Continue lifelong cART (regardless of CD4 count)
- Contraception counseling (avoid OCP if on enzyme-inducing ARVs; IUCD or barrier methods preferred)
- Screen for postnatal depression
- Partner testing and counseling
Sources: Creasy & Resnik's Maternal-Fetal Medicine; Berek & Novak's Gynecology; Rosen's Emergency Medicine; Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.