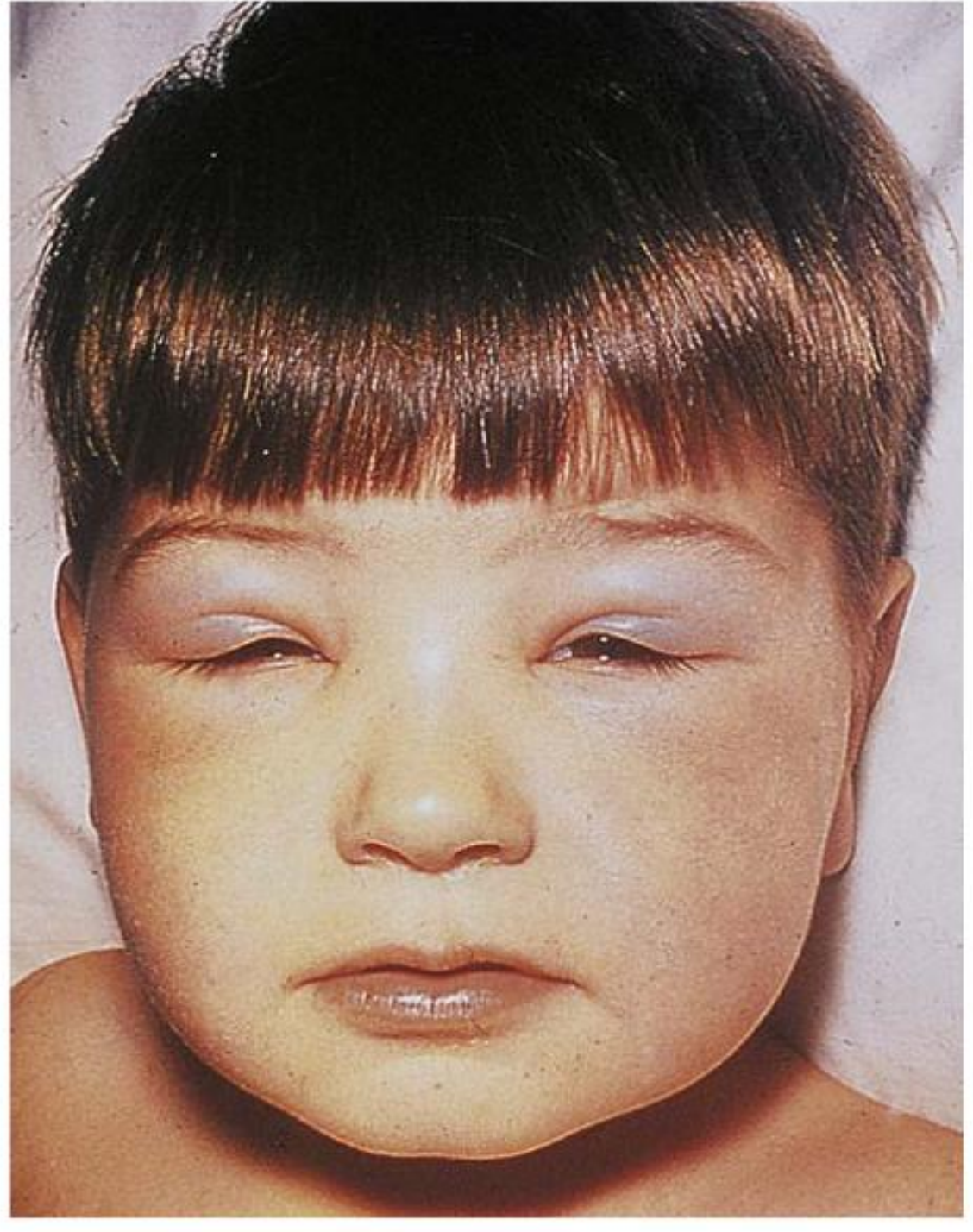
Puffiness under eye dd
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Here is a structured differential diagnosis for puffiness/swelling under the eye (periorbital/infraorbital region):
Differential Diagnosis: Puffiness / Swelling Under the Eye
1. Inflammatory / Infectious Causes (usually erythematous, tender)
| Condition | Key Features |
|---|---|
| Preseptal (periorbital) cellulitis | Acute eyelid erythema, edema, warmth; anterior to orbital septum; no proptosis or restricted motility |
| Orbital cellulitis | Proptosis + restricted ocular motility + pain on eye movement; posterior to septum; EMERGENCY |
| Hordeolum (stye) | Tender eyelid nodule from blocked meibomian/Zeis gland |
| Chalazion | Chronic, non-tender lid nodule (blocked meibomian gland); may cause lower lid swelling |
| Dacryoadenitis | Erythema/swelling outer one-third upper lid; S-shaped lid; preauricular lymphadenopathy |
| Blepharitis | Lid margin inflammation, crusting, bilateral, chronic |
| Conjunctivitis | Accompanying discharge, chemosis |
| Herpes simplex / Varicella zoster dermatitis | Vesicular rash, dermatomal distribution |
| Contact dermatitis | Allergen/irritant exposure; itch, eczematous changes |
| Erysipelas | Streptococcal skin infection; sharply demarcated, bright red, indurated |
| Insect bite | History of bite; acute onset, asymmetric |
2. Non-inflammatory Causes (soft, non-tender, no erythema)
| Condition | Key Features |
|---|---|
| Orbital fat prolapse / festoons | Chronic, bilateral, soft herniation of orbital fat; most common cosmetic complaint |
| Allergic / angioedema | Rapid onset, bilateral, itching; urticarial elsewhere; associated with food/drug/environmental trigger |
| Renal disease (nephrotic syndrome) | Bilateral periorbital puffiness, worse in morning; proteinuria, hypoalbuminemia |
| Hypothyroidism / Myxedema | Diffuse non-pitting periorbital edema; dry skin, fatigue, bradycardia |
| Thyroid eye disease (Graves') | Bilateral proptosis, lid retraction, lid lag, chemosis, restricted motility |
| Superior vena cava (SVC) syndrome | Bilateral facial/periorbital edema + neck/arm engorgement; venous distension |
| Cardiac disease | Bilateral dependent/periorbital edema; usually signs of systemic fluid overload |
| Eyelid/lacrimal gland mass | Unilateral, firm, progressive; globe displacement in malignant tumors |
| Dermoid cyst (leaking) | Superolateral or superomedial; leakage causes acute inflammatory reaction |
| Idiopathic orbital inflammatory syndrome (IOIS) | Painful proptosis, afebrile, normal WBC; responds to steroids not antibiotics |
| Rhabdomyosarcoma | Most common pediatric orbital malignancy; rapid onset |
| Lymphoproliferation / sarcoidosis / IgG4-related disease | Indolent, painless; often bilateral |
3. Traumatic
- Periorbital hematoma ("black eye") — ecchymosis, history of trauma
- Foreign body with secondary inflammation
Distinguishing Features at a Glance
| Feature | Think of |
|---|---|
| Morning bilateral puffiness, soft | Renal/thyroid/cardiac, sleep position, allergy |
| Unilateral, red, tender, fever | Cellulitis (preseptal vs. orbital), hordeolum |
| Proptosis + restricted gaze | Orbital cellulitis, Graves', IOIS, tumor |
| Rapid onset, itchy, bilateral | Angioedema/allergic |
| Chronic, progressive, painless | Fat prolapse, lacrimal gland mass, lymphoma |
| Vesicular rash | Herpes/VZV |
| Child, rapid, painless mass | Rhabdomyosarcoma |
Key red flags warranting urgent evaluation: proptosis, restricted extraocular movements, pain on eye movement, vision change, fever with unilateral swelling → rule out orbital cellulitis, cavernous sinus thrombosis, or malignancy.
— The Wills Eye Manual, Office and Emergency Room Diagnosis and Treatment of Eye Disease
Test to be done
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Here is a comprehensive, diagnosis-guided approach to investigations for puffiness under the eye:
Investigations for Puffiness Under the Eye
Step 1 — Clinical Examination First (Before Tests)
| Parameter | What to Check |
|---|---|
| Pain on eye movement | Suggests orbital (postseptal) cellulitis |
| Proptosis | Orbital cellulitis, Graves', tumor |
| Restricted extraocular motility | Orbital process |
| Afferent pupillary defect / colour vision | Optic nerve involvement |
| Vesicular rash | Herpes simplex / VZV |
| Vitals (temp, BP) | Fever → infection; raised BP → renal cause |
| Lymph nodes (head & neck) | Malignancy, infectious |
| Facial sensation (V1/V2) | Orbital/cavernous sinus pathology |
| Disc edema on fundoscopy | Raised ICP / cavernous sinus thrombosis |
Step 2 — Laboratory Tests
| Test | Indication / What It Detects |
|---|---|
| CBC with differential | Leukocytosis → cellulitis / infection; eosinophilia → allergy |
| Blood culture | Severe/febrile preseptal or orbital cellulitis |
| Wound/discharge Gram stain & culture | Any open wound or purulent drainage |
| Serum creatinine + BUN | Renal disease (nephrotic/nephritic syndrome) |
| Urine routine & microscopy | Proteinuria → nephrotic syndrome; RBC casts → nephritic |
| Serum albumin | Low in nephrotic syndrome → periorbital edema |
| TSH + free T4 | Hypothyroidism (myxedema) or hyperthyroidism (Graves') |
| TRAb / TSH receptor antibodies | Thyroid eye disease (Graves') |
| Serum IgE + eosinophil count | Allergic etiology |
| ANA, anti-dsDNA, complement | Autoimmune (lupus, dermatomyositis) |
| Serum ACE, calcium | Sarcoidosis |
| IgG4 levels | IgG4-related orbital disease |
| Serum LDH, β2-microglobulin | Lymphoma |
| Blood glucose / HbA1c | Diabetic nephropathy (if renal edema suspected) |
Step 3 — Imaging
| Test | When to Order | Findings |
|---|---|---|
| CT orbits + sinuses (axial & coronal, with contrast) | ANY suspicion of orbital cellulitis, subperiosteal abscess, sinusitis, trauma, foreign body, or tumor | Differentiates preseptal vs. postseptal; shows abscess, fat stranding, sinusitis |
| CT brain | Fever + altered sensorium, signs of cavernous sinus thrombosis | Cavernous sinus thrombosis, intracranial extension |
| MRI orbit / brain with contrast | Suspected cavernous sinus thrombosis, intracranial pathology, soft tissue masses, or if CT inconclusive | Better soft tissue resolution; cavernous sinus pathology |
| MR angiography / venography | Suspected cavernous sinus thrombosis | Venous sinus occlusion |
| Thyroid ultrasound | Thyroid eye disease | Thyroid anatomy |
| Chest X-ray | Cardiac failure, sarcoidosis, lymphoma | Cardiomegaly, hilar lymphadenopathy |
| Echocardiography | Suspected cardiac cause of bilateral edema | Systolic/diastolic dysfunction |
Step 4 — Special Tests (Targeted)
| Test | Indication |
|---|---|
| Skin patch testing | Contact dermatitis |
| Allergy skin prick / RAST | Allergic angioedema |
| Serum tryptase / complement C4 | Hereditary angioedema (C1-inhibitor deficiency) |
| Skin biopsy | Dermatomyositis, lupus, lymphoma |
| Fine needle aspiration / biopsy | Lacrimal gland mass, lymphoma |
| 24-hour urine protein | Quantify proteinuria in nephrotic syndrome |
Quick Decision Guide
| Clinical Scenario | Priority Investigation |
|---|---|
| Unilateral, red, tender, febrile | CBC + blood culture + contrast CT orbit & sinuses |
| Bilateral, morning puffiness, non-tender | Urinalysis, serum albumin, creatinine, TSH |
| Rapid bilateral onset, itchy | IgE, eosinophils, C4 (angioedema screen) |
| Proptosis + lid retraction | TSH, TRAb, thyroid USS, CT/MRI orbit |
| Painless progressive unilateral | CT orbit, biopsy (rule out tumor/lymphoma) |
| Child with rapid painful mass | Urgent CT orbit (rule out rhabdomyosarcoma/abscess) |
| Bilateral + dyspnoea + JVD | CXR, ECG, echo (cardiac cause) |
— The Wills Eye Manual, Office and Emergency Room Diagnosis and Treatment of Eye Disease; Tintinalli's Emergency Medicine: A Comprehensive Study Guide
Bilateral, morning puffiness, non-tender, but the puffiness presist since start for 2 days
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Based on the textbook content retrieved, here is a focused clinical assessment for this scenario:
Clinical Scenario: Bilateral, Non-tender, Persistent Periorbital Puffiness × 2 Days
Key features to narrow the differential:
- Bilateral → systemic cause (not local infection/mass)
- Non-tender, non-erythematous → non-inflammatory
- Worse in morning → fluid redistribution while supine overnight
- Persistent 2 days → beyond simple fatigue/allergy trigger
Most Likely Diagnoses
🔴 1. Nephrotic Syndrome (Top Priority)
The classic cause of bilateral morning periorbital puffiness.
"In the nephrotic patient, edema is often periorbital in the morning — the edema resolves during the day under the influence of gravity." — Comprehensive Clinical Nephrology, 7th Ed.
Mechanism: Hypoalbuminemia → ↓ oncotic pressure → fluid leaks into interstitium
Associated features to ask about:
Associated features to ask about:
- Frothy urine (proteinuria)
- Ankle swelling (worsens by evening)
- Decreased urine output
- Abdominal bloating (ascites)
- Fatigue
🟡 2. Hypothyroidism / Myxedema
"Facial puffiness, periorbital edema, and enlargement of the tongue can occur. This appears as non-pitting cutaneous edema with firm texture and pale waxy appearance." — Tietz Textbook of Laboratory Medicine, 7th Ed.
Non-pitting, bilateral, firm periorbital edema is a hallmark of myxedema (severe hypothyroidism).
Associated features: Weight gain, cold intolerance, dry skin, hair loss, constipation, bradycardia, fatigue, somnolence, hoarse voice
Associated features: Weight gain, cold intolerance, dry skin, hair loss, constipation, bradycardia, fatigue, somnolence, hoarse voice
🟡 3. Allergic Reaction / Angioedema
- Subacute onset (can persist 2 days), bilateral, non-tender, itchy
- Drug-induced (ACE inhibitors classically), food allergy, idiopathic
- Hereditary angioedema (C1-inhibitor deficiency): recurrent episodes, no urticaria, no itch, does not respond to antihistamines
Associated features: Urticaria elsewhere, lip/tongue swelling, drug history (especially ACEi/ARB, NSAIDs)
🟠 4. Cardiac Failure
- Bilateral periorbital edema is less typical than ankle edema, but can occur in severe cases
- Usually: orthopnea, PND, bilateral leg edema, raised JVP, S3 gallop
🟠 5. Hepatic Cirrhosis / Hypoalbuminemia
- Periorbital edema from hypoalbuminemia
- Associated: ascites, jaundice, spider naevi, palmar erythema, alcohol history
🟢 6. Other Considerations (2 days, bilateral)
| Cause | Clue |
|---|---|
| Sleep deprivation / fluid retention | Self-limiting, no systemic symptoms |
| Excess salt/fluid intake | Dietary history |
| Premenstrual fluid retention | Cyclical, in women |
| Dermatomyositis | Heliotrope rash (violaceous periorbital discolouration) + proximal myopathy |
| SVC syndrome | + neck/arm venous engorgement, plethora |
Recommended Investigations (Targeted for This Scenario)
Urine
| Test | Rationale |
|---|---|
| Urine dipstick | Proteinuria → nephrotic syndrome |
| Urine routine & microscopy | RBC casts → nephritic; fatty casts → nephrotic |
| 24-hour urine protein OR spot PCR (protein:creatinine ratio) | Quantify proteinuria (>3.5 g/day = nephrotic range) |
Blood
| Test | Rationale |
|---|---|
| Serum albumin | Low → nephrotic/cirrhosis/malnutrition |
| Serum creatinine + BUN + eGFR | Kidney function |
| TSH + free T4 | Hypothyroidism |
| Lipid profile | Hyperlipidaemia in nephrotic syndrome |
| CBC | Anaemia, eosinophilia (allergy) |
| LFTs + serum bilirubin + PT/INR | Liver/cirrhosis |
| Fasting blood glucose / HbA1c | Diabetic nephropathy |
| C3, C4, CH50 | Complement → lupus nephritis, MPGN, post-streptococcal GN |
| ANA, anti-dsDNA | Lupus |
| ASO titre | Post-streptococcal GN (especially children) |
| Serum IgE | Allergy |
| C1-inhibitor level + function | Hereditary angioedema (if recurrent, no itch) |
Imaging
| Test | Rationale |
|---|---|
| Kidney ultrasound | Kidney size, rule out obstruction |
| CXR | Pleural effusion (nephrotic/cardiac), cardiomegaly |
| Echocardiography | If cardiac failure suspected |
Most Urgent Next Step
Given 2 days of persistent bilateral morning puffiness with no inflammation:
Check urine dipstick for protein first — if 2+ or more, proceed with spot protein:creatinine ratio and serum albumin. This will confirm or exclude nephrotic syndrome rapidly and guide further workup.
— Comprehensive Clinical Nephrology, 7th Edition; Tietz Textbook of Laboratory Medicine, 7th Edition
The puffiness is on the skin of lower orbiculatis ovculus
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
This is an important anatomical clarification. The puffiness is specifically in the skin overlying the lower orbicularis oculi muscle — this is the infraorbital / lower eyelid skin region, which helps narrow things significantly.
Anatomical Context
The lower eyelid layers from superficial to deep:
Skin → Orbicularis oculi (pretarsal + preseptal) → Orbital septum → Orbital fat (3 compartments) → Tarsal plate
Puffiness in the skin of the lower orbicularis oculi = fluid/swelling in the skin and subcutaneous tissue just below the lower lid margin — this is a very specific and clinically important location.
Revised Differential — Bilateral Skin-Level Swelling Over Lower Orbicularis Oculi × 2 Days, Non-tender
🔴 1. Allergic / Contact Dermatitis
The lower eyelid skin is extremely thin (~0.5 mm) and highly reactive to allergens.
- Contact allergens: Eye drops, cosmetics (mascara, eyeliner, eye shadow), nail polish (transferred by rubbing), face creams, preservatives (benzalkonium chloride)
- Atopic dermatitis: Pre-existing eczema
- Features: Bilateral (cosmetic use is bilateral), fine skin wrinkling, mild erythema possible, +/- itch
- 2 days duration fits a new allergen exposure
🔴 2. Angioedema
- Deep dermal/subdermal oedema of the lower eyelid skin
- Non-pitting, non-tender, no erythema
- Drug-induced (ACEi, NSAIDs), food, idiopathic, or hereditary (C1-INH deficiency)
- Bilateral distribution is classic
- Can persist 24–72 hours per episode
🟡 3. Nephrotic Syndrome
- Hypoalbuminaemia → fluid accumulates in the loose subcutaneous tissue of the lower eyelid preferentially
- Worse in morning (recumbent position equalises fluid)
- The lower orbicularis skin is the earliest and most obvious site in children and young adults
- Associated: frothy urine, periankle oedema by end of day
🟡 4. Dermatomyositis — Heliotrope Sign
"A pink-violet colour, primarily of the eyelids and periorbital skin, which may have associated oedema." — Dermatology, 5th Edition (Bolognini)
- Bilateral periorbital oedema with violaceous (heliotrope) discolouration of the eyelid skin
- Often subtle — can be mistaken for allergic dermatitis
- Ask about: proximal muscle weakness (difficulty climbing stairs, raising arms), Gottron papules on knuckles, V-neck rash on chest
🟡 5. Hypothyroidism (Myxedema)
- Non-pitting, firm, bilateral lower eyelid skin oedema
- Pale, waxy, doughy feel
- Ask about: fatigue, cold intolerance, dry skin, constipation, weight gain, bradycardia
🟠 6. Trichinosis (Trichinella spiralis)
- Classic teaching: bilateral periorbital oedema (lower lid) + fever + myalgia + eosinophilia
- From undercooked meat
- Rare but pathognomonic when present
🟢 7. Renal / Cardiac / Hepatic Oedema
- Less likely to be confined only to the lower eyelid skin without other signs
- Still worth excluding with basic labs
Key History to Ask NOW
| Question | Points Toward |
|---|---|
| Any new cosmetics, eye drops, creams started? | Contact dermatitis |
| Any itching? | Allergic (contact dermatitis, angioedema) |
| Any lip/tongue swelling? | Angioedema |
| Frothy urine? Ankle swelling? | Nephrotic syndrome |
| Fatigue, weight gain, cold intolerance? | Hypothyroidism |
| Muscle weakness (arms/legs)? | Dermatomyositis |
| Undercooked pork/wild meat? Muscle pain? Fever? | Trichinosis |
| Family history of similar episodes? | Hereditary angioedema |
| Violaceous/purple colour of the skin? | Dermatomyositis |
| ACEi / NSAID use? | Drug-induced angioedema |
Focused Investigations
| Test | Target |
|---|---|
| Urine dipstick + spot protein:creatinine ratio | Nephrotic syndrome |
| Serum albumin, creatinine | Nephrotic, cirrhosis |
| TSH + free T4 | Hypothyroidism |
| CBC with differential | Eosinophilia → allergy/trichinosis |
| Serum IgE | Atopic/allergic |
| C4 + C1-inhibitor level/function | Hereditary angioedema |
| CK, aldolase, LDH | Dermatomyositis (muscle enzymes) |
| ANA, anti-Jo-1, anti-Mi-2 | Dermatomyositis |
| Trichinella serology | If fever + myalgia + eosinophilia |
| Patch testing (dermatology referral) | Contact allergen identification |
Bottom Line
The most common cause of bilateral, non-tender, persistent skin-level swelling over the lower orbicularis oculi for 2 days is:
- Allergic contact dermatitis (new cosmetic/eye product — most common in adults)
- Angioedema (drug/food/idiopathic)
- Nephrotic syndrome (if frothy urine or other systemic oedema)
- Dermatomyositis (if subtle violaceous hue — do not miss)
— Dermatology, 5th Edition (Bolognini); Comprehensive Clinical Nephrology, 7th Ed.; The Wills Eye Manual
This is a shared conversation. Sign in to Orris to start your own chat.