Indication , procedure and complication of endoscopic orbital decompression in detail according to standard ent textbook
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, detailed information from Cummings Otolaryngology (the gold-standard ENT textbook). Let me compile the full detailed answer:
Endoscopic Orbital Decompression
Source: Cummings Otolaryngology Head and Neck Surgery, Chapters 49 and 125
Background and Historical Context
Orbital decompression was first described by Dollinger (lateral orbital wall removal into the temporal fossa - Kronlein procedure). Naffziger later reported transcranial removal of the orbital roof. Sewell described decompression into the maxillary sinus. Walsh and Ogura combined the inferior and medial approaches into a single transantral two-wall decompression (Caldwell-Luc approach).
In 1990, Kennedy et al. described the first endoscopic medial and inferior orbital decompression for Graves orbitopathy. Since early 1990s studies demonstrated equivalent results to the transantral approach, endoscopic techniques have become the preferred surgical treatment. The endoscopic approach offers improved visualization and access to the orbital walls while avoiding disruption of normal external structures.
I. INDICATIONS
Primary Indication
Graves Orbitopathy (GO) / Thyroid Eye Disease - accounts for the vast majority of cases. In GO, orbital soft tissue volume increases due to inflammation and deposition of glycosaminoglycans within orbital fat and extraocular muscles (EOMs), leading to increased intraorbital pressure.
Specific Operative Indications:
| Indication | Details |
|---|---|
| Exophthalmos / Proptosis | Most common indication; cosmetically and functionally disabling "thyroid stare" |
| Exposure Keratopathy | From lid retraction + lagophthalmos; if untreated progresses to corneal ulceration or perforation with permanent visual loss |
| Compressive Optic Neuropathy (CON) | EOM hypertrophy at orbital apex compresses the optic nerve - an urgent indication for decompression |
| Diplopia | Though surgery can also cause diplopia (paradoxically), significant pre-existing diplopia may be addressed |
| Psychosocial / Cosmetic | Even without corneal or optic nerve threat, significant disfigurement is a legitimate elective indication |
| Failure of Medical Management | Failure to adequately respond to steroids, immunomodulators, or inability to tolerate them |
Clinical Signs Suggesting Urgency (CON):
- Dyschromatopsia (color vision loss)
- Relative afferent pupillary defect (RAPD)
- Decreased visual acuity
- These mandate urgent decompression before permanent visual loss ensues
II. PREOPERATIVE EVALUATION
Ophthalmologic Assessment
- Exophthalmometry - quantifies degree of proptosis (also used postoperatively to measure decompression)
- Extraocular movements and diplopia assessment - absence of diplopia preoperatively may invoke a "diplopia-sparing" technique
- Color vision testing (dyschromatopsia)
- RAPD assessment
- Visual acuity
Imaging
- CT orbits and sinuses WITHOUT contrast - evaluates bony orbital walls and sinonasal anatomy; also used for intraoperative image guidance
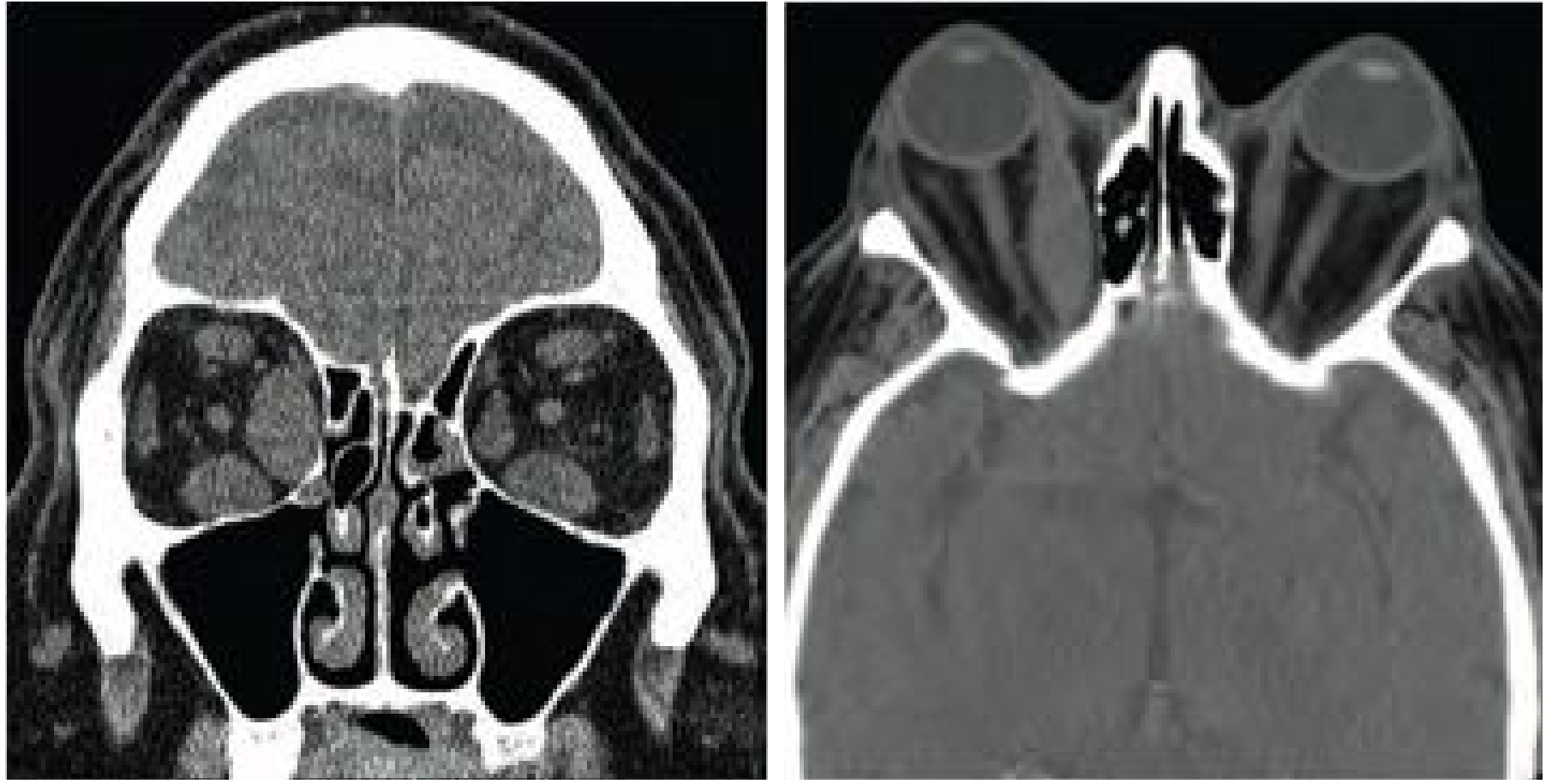
- Important: IV contrast is strictly avoided in Graves orbitopathy - reported cases of severe and immediate exacerbation following iodine-rich contrast administration
- MRI - generally not necessary if diagnosis is clear
Fig. 49.10 - Coronal and axial CT of Graves orbitopathy: note hypertrophied extraocular muscles, increased orbital volume and proptosis:
III. PROCEDURE (SURGICAL TECHNIQUE)
Anesthesia
- Performed under general anesthesia in most cases
- Local anesthesia with sedation is an option for patients with contraindications to GA, or if operating on the only-seeing eye (allows intraoperative monitoring of visual function)
Setup
- Patient in supine position (as for endoscopic sinus surgery)
- Eyes kept in the surgical field to check pupils and EOM motility throughout the case
- Scleral shields placed for corneal protection
- Topical vasoconstrictive agent applied
- Intranasal injections: 1% lidocaine with 1:100,000 epinephrine at axilla of middle turbinate and along the lateral nasal wall
- Stereotactic image navigation (CT-guided): widely used to identify anatomic structures, localize ethmoidal neurovascular bundles, and improve outcomes while decreasing operative times
Step 1: Exposure (Endoscopic Sinus Surgery Phase)
- Uncinectomy - uncinate process removed
- Maxillary antrostomy - large antrostomy contiguous with the natural os, extended posterior to the posterior maxillary wall and inferiorly to the superior edge of the inferior turbinate
- Purpose: access to orbital floor AND prevention of postobstructive maxillary sinusitis from herniation of orbital fat
- Total ethmoidectomy - exposing the ethmoid roof superiorly and lamina papyracea laterally
- Thorough posterior ethmoidectomy = maximal decompression
- Anterior-most and superior-most ethmoid air cells (frontal sinus outflow tract) are preserved to prevent postobstructive frontal sinusitis
- Wide sphenoidotomy - performed if orbital apex decompression is needed (on the planum sphenoidale superiorly and orbital apex laterally)
- Middle turbinate: generally preserved unless it precludes adequate decompression; if removed, it facilitates wider exposure
- Mucosa overlying lamina papyracea is removed; maxillary sinus mucosa is temporarily reflected then redraped at completion to facilitate remucosalization
Step 2: Bony Decompression (Medial Wall - Lamina Papyracea)
- An elevator or curette fractures the mid-portion of the lamina papyracea in a controlled fashion
- Posterior bone fragments elevated and removed from underlying periorbita - from sphenoid face posteriorly to the frontal process of the maxilla anteriorly
- Superiorly, lamina removed to the frontoethmoid suture (except near the frontal sinus outflow tract)
- Care is taken to avoid premature violation of periorbita (which causes early fat herniation, compromising visualization)
- The annulus of Zinn is encountered as a thickening of periorbita approximately 2 mm from the sphenoid rostrum - this marks the posterior limit of dissection
Step 3: Bony Decompression (Inferior Wall - Orbital Floor)
- Visualized using an angled endoscope
- Inferomedial strut preservation option: A high-speed curved drill with diamond burr thins the bone lateral to the inferomedial orbital strut and medial to the infraorbital nerve; further bone removed using ball-tipped probe + frontal sinus punch/through-cutting instruments
- Without strut preservation: Periorbita elevated from orbital floor using ball-tipped probe, followed by controlled down-fracture using curette
- Fracture line extends to the infraorbital canal - the lateral limit of endoscopic inferior wall decompression
- Infraorbital nerve = lateral limit of inferior wall dissection
- For compressive optic neuropathy: orbital apex decompression accomplished by removal of the orbital process of the palatine bone using a high-speed drill; if severe CON unresponsive to high-dose steroids, optic nerve decompression is considered
Step 4: Periorbita Opening (Soft Tissue Decompression)
- A sickle knife penetrates the periorbita posteriorly first then carries the incision anteriorly
- Posterior-to-anterior direction prevents fat prolapse from blocking visualization
- Two parallel horizontal incisions can be made on the periorbita
- Orbital sling technique (diplopia-sparing): a 10-mm strip of periorbita is preserved overlying the medial rectus muscle (coinciding with its upper and lower borders) to act as a sling, preventing prolapse into the ethmoid cavity
- Not used when vision is threatened (CON) - complete periorbita removal is preferred in those cases
- Additional sickle knife incisions release fibrous adhesions within orbital fat to facilitate herniation
- Hemostasis confirmed
- No nasal packing is placed - to avoid pressure along the orbital apex and optic nerve
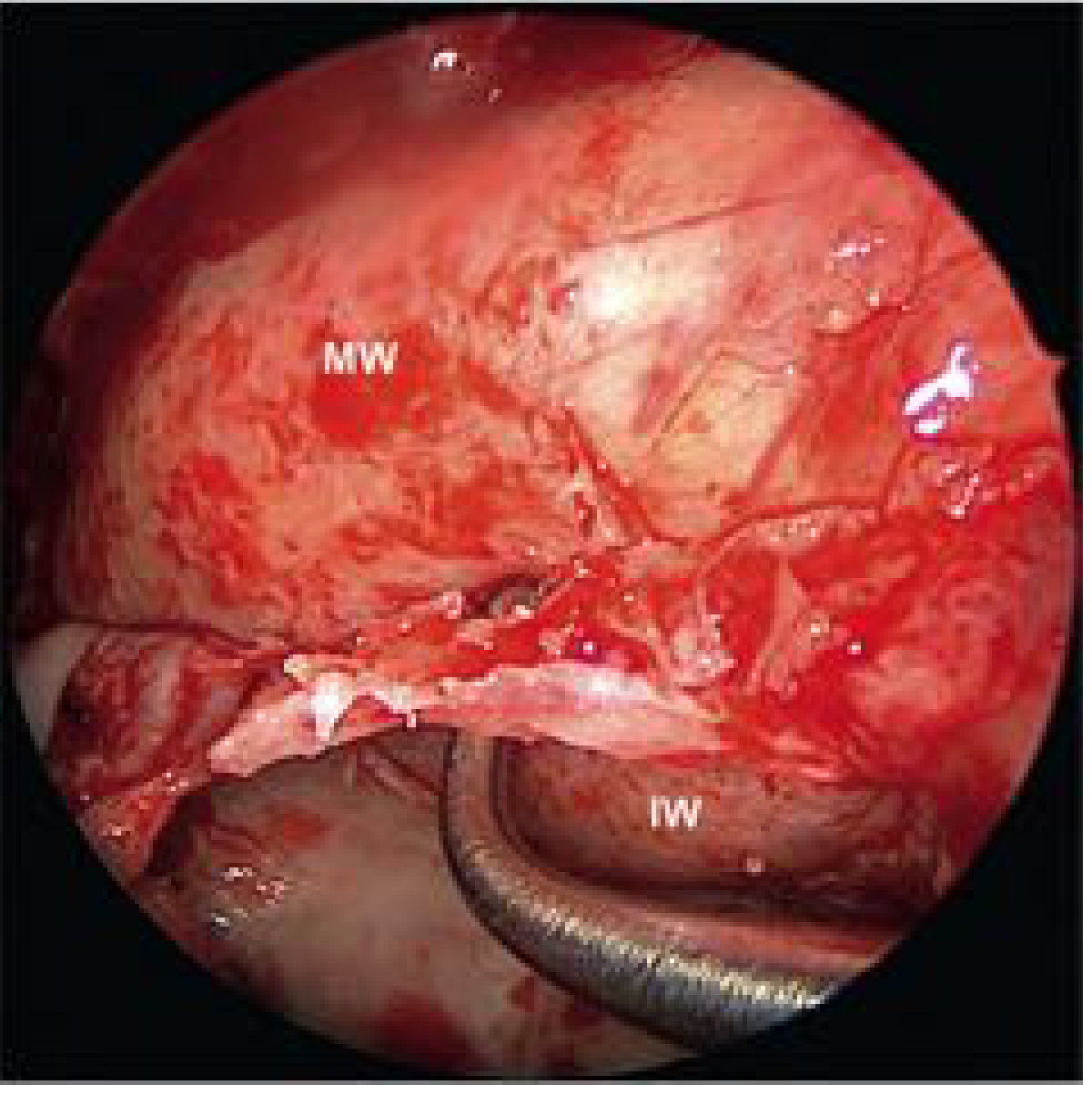
Fig. 49.11 - Endoscopic view of inferomedial orbital strut preservation (MW = medial wall periorbita; IW = inferior wall periorbita):
Special Diplopia-Sparing Strategies (Summary)
| Technique | Mechanism | Effect on Diplopia |
|---|---|---|
| Inferomedial orbital strut preservation | Preserves triangular bony junction of medial + inferior walls | No new-onset diplopia in strut-preserved cases (feasible in 71-100%) |
| Orbital sling / periorbital strip | 10-mm periorbita strip over medial rectus prevents prolapse | Significantly lower new-onset diplopia vs conventional technique |
| Balanced decompression | Concurrent medial (endoscopic) + lateral (external) decompression, without floor removal | Diplopia 0-15%; avoids asymmetric EOM displacement |
Note: Both strut preservation and orbital sling techniques can decrease the degree of decompression - therefore not recommended in cases with CON.
IV. BALANCED ORBITAL DECOMPRESSION
A modification in which the medial and lateral orbital walls are decompressed without decompressing the floor, to maintain a neutral medial-to-lateral globe position:
- Lateral wall decompression performed via upper eyelid or lateral canthotomy incision, removing bone between lateral orbital rim and sphenoid trigone
- Medial decompression via endoscopic transnasal approach
- Decompresses equally medially and laterally - less likely to affect globe position
- If orbital fat is resected concurrently, degree of decompression equals three-wall (medial-inferior-lateral) decompression
- Postoperative new-onset diplopia: 0% to 15%
- Requires collaboration between rhinology and ophthalmology
V. OUTCOMES
- Average proptosis reduction with endoscopic medial + inferior wall decompression: 3.2 ± 1.1 mm (range 3.2 to 5.1 mm)
- Adding lateral wall decompression provides an additional 2.4 mm reduction (total 5.6 ± 1.7 mm)
- Balanced decompression (with preserved medial sling): 5.1 ± 1.1 mm reduction
- Strut preservation: mean reduction of 3.60 mm
- Significant improvements in SNOT-22 scores at 1 year - procedure does not negatively impair long-term sinonasal physiologic function
VI. COMPLICATIONS
A. Intraoperative Complications
| Complication | Notes |
|---|---|
| Premature fat prolapse | From inadvertent periorbita violation; compromises visualization and thoroughness of decompression |
| Ethmoidal artery injury | Retraction into orbit can cause retrobulbar hematoma; managed by endoscopic orbital decompression with cautery/clipping, or external ethmoidectomy |
| CSF leak | From inadvertent skull base injury |
| Orbital contents injury | Direct injury to EOMs, optic nerve, or neurovascular bundles |
B. Postoperative Complications
1. New-Onset Diplopia (most common complication)
- Most common complication - reported in 30% to 64% depending on technique
- Even with endoscopic approach: 19% to 45% rate
- Mechanisms: direct muscular or neurovascular injury, significant orbital tissue prolapse, disruption of extraocular muscle axes, globe prolapse
- Management: diplopia-sparing techniques (strut, sling, balanced decompression) intraoperatively; corrective eye muscle surgery when permanent
- Surgical intervention for GO is typically reserved for optic nerve involvement or medical treatment failure given this risk
2. Postoperative Epistaxis
- Uncommon: less than 5% of patients
- Typically originates along the remnant middle turbinate
- Bedside nasal packing is specifically contraindicated - due to exposed orbital contents (packing pressure transmitted to orbit)
- Management: return to OR for endoscopic cauterization; in severe cases, sphenopalatine artery ligation
- Prevention: intraoperative cauterization of remnant middle turbinate edges
3. Retrobulbar Hematoma
- Due to intraorbital dissection nature
- Even though orbit is decompressed, risk of permanent visual loss remains
- Additional decompression via lateral canthotomy with inferior cantholysis may be necessary
4. Postoperative Compressive Optic Neuropathy
- From postoperative edema
- Prevention and management: intraoperative and postoperative corticosteroids with a taper
5. Sinusitis / Mucocele
- Secondary to obstruction from herniated orbital fat into the sinonasal cavity
- Can be postobstructive maxillary sinusitis, frontal sinusitis, or sphenoid sinusitis
- Generally a late complication - may occur even decades after original decompression
- Prevention: prophylactic sinusotomy and judicious mucosal stripping; the anterior-superior orbit should NOT be decompressed (to protect frontal sinus outflow)
6. CSF Leak (from transantral open approach)
- Reported in 3% in large series (Garrity et al.) for transantral approach
- Minimized with endoscopic modification
7. Other Less Common Complications (from large series)
- Sinusitis: 4%
- Lower eyelid entropion: 9% (infra-orbital nerve paresthesia may contribute)
- Frontal lobe hematoma: 0.2%
- Blindness from optic nerve injury or orbital hemorrhage: rare but reported
VII. POSTOPERATIVE CARE
- Similar to routine endoscopic sinus surgery
- Oral antibiotics
- Twice-daily nasal saline irrigations
- Endoscopic debridement in the office at 1 week postoperatively
- Intraoperative and postoperative corticosteroids with taper (to reduce edema and prevent compressive optic neuropathy)
- No nasal packing is placed
VIII. SEQUENCING OF SURGICAL REHABILITATION IN GRAVES ORBITOPATHY
When multiple procedures are needed, they must be staged in the correct order:
- Orbital decompression first (if proptosis is severe)
- Extraocular muscle surgery - delayed at least 2 to 3 months after decompression (recession of globe is progressive for several months)
- Eyelid surgery last - delayed at least 1 year after disease stabilization
Cummings Otolaryngology Head and Neck Surgery, 7th Edition - Chapter 49 (Endoscopic Orbital Decompression) and Chapter 125 (Orbital Decompression)
This is a shared conversation. Sign in to Orris to start your own chat.