Treatment of hepatic encephalopathy based on harrison's
Treatment of Hepatic Encephalopathy
Pathophysiology (Brief)
1. Identify and Correct Precipitating Factors (First Priority)
| Precipitant | Action |
|---|---|
| Volume depletion | Appropriate hydration |
| GI bleeding | Identify and treat bleeding source |
| Hyponatremia | Correct electrolytes |
| Infection (including SBP) | Tap ascites to rule out infection; treat with antibiotics |
| Constipation | Catharsis |
2. Dietary Protein - Do NOT Restrict
3. Lactulose (Mainstay of Treatment)
- Mechanism: Lactulose is a non-absorbable disaccharide that causes colonic acidification (lowers luminal pH), which traps ammonia as NH4+ and promotes its elimination in stool. Catharsis further reduces nitrogenous substrate in the gut.
- Goal: 2-3 soft stools per day.
- Dosing: Patients self-titrate their lactulose dose to achieve this target.
- Duration: Lactulose is typically continued after the initial episode (long-term secondary prevention).
4. Poorly Absorbed Antibiotics (Adjunctive Therapy)
- Have difficulty tolerating lactulose, OR
- Have recurrent episodes of encephalopathy
"Rifaximin, in a dose of 550 mg twice daily, has been shown to be superior to placebo, in addition to lactulose, in preventing recurrent bouts of hepatic encephalopathy."
- Harrison's, p. 2760
5. Special Considerations by Setting
Acute Liver Failure (ALF)
- Encephalopathy in ALF can be associated with life-threatening cerebral edema - a feature not seen in chronic liver disease.
- Treatment of cerebral edema: hypertonic saline or mannitol.
- Cerebral herniation is the feared complication.
Chronic Liver Disease / Cirrhosis
- Focus is on identifying precipitants and initiating lactulose ± rifaximin.
- Patients who have experienced an episode often learn to self-medicate at early signs of recurrence.
6. Liver Transplantation
Summary Table
| Intervention | Role | Notes |
|---|---|---|
| Treat precipitating cause | First-line, always | Volume, infection, GI bleed, electrolytes |
| Protein restriction | Contraindicated | Worsens malnutrition/sarcopenia |
| Lactulose | Mainstay | Target 2-3 soft stools/day; long-term use |
| Rifaximin 550 mg BID | Adjunct / recurrence prevention | Superior to placebo when added to lactulose |
| Hypertonic saline / mannitol | For cerebral edema in ALF only | Not applicable in chronic liver disease |
| Liver transplantation | Definitive | Indicated in refractory/recurrent HE |
Create a treatment algorithm poster for hepatic encephalopathy management
A clean, professional medical treatment algorithm poster for Hepatic Encephalopathy Management based on Harrison's Principles of Internal Medicine. The poster should have: - Title at top: "HEPATIC ENCEPHALOPATHY: Treatment Algorithm" with a subtitle "Based on Harrison's Principles of Internal Medicine 22E" - A flowchart/algorithm with the following steps in order: STEP 1 (top box, red/orange): "DIAGNOSE HEPATIC ENCEPHALOPATHY - Clinical diagnosis: altered mental status + liver disease - Check for asterixis (liver flap) - Rule out alternative causes" STEP 2 (yellow box): "IDENTIFY & CORRECT PRECIPITATING FACTORS" with 5 sub-boxes in a row: "Volume Depletion → Hydrate", "GI Bleeding → Treat", "Infection/SBP → Tap ascites + Antibiotics", "Electrolyte Abnormalities → Correct", "Constipation → Catharsis" STEP 3 (green box): "ACUTE LIVER FAILURE?" with two branches - YES branch (red): "Cerebral edema risk → Hypertonic saline or Mannitol" and NO branch: Continue to Step 4 STEP 4 (blue box, main treatment): "MAINSTAY TREATMENT: LACTULOSE (Non-absorbable disaccharide) - Goal: 2-3 soft stools/day - Patient self-titrates dose - Continue long-term after first episode - Mechanism: colonic acidification → traps NH3 as NH4+" STEP 5 (purple box): "RECURRENT or REFRACTORY EPISODES? Add RIFAXIMIN 550 mg twice daily (superior to placebo when added to lactulose)" IMPORTANT NOTE box (red border): "❌ DO NOT restrict dietary protein — worsens malnutrition and sarcopenia" STEP 6 (dark blue box at bottom): "REFRACTORY HE → Refer for LIVER TRANSPLANTATION (Definitive treatment)" Use color-coded boxes, arrows connecting each step, clean medical typography, white background, professional clinical design suitable for a hospital ward.
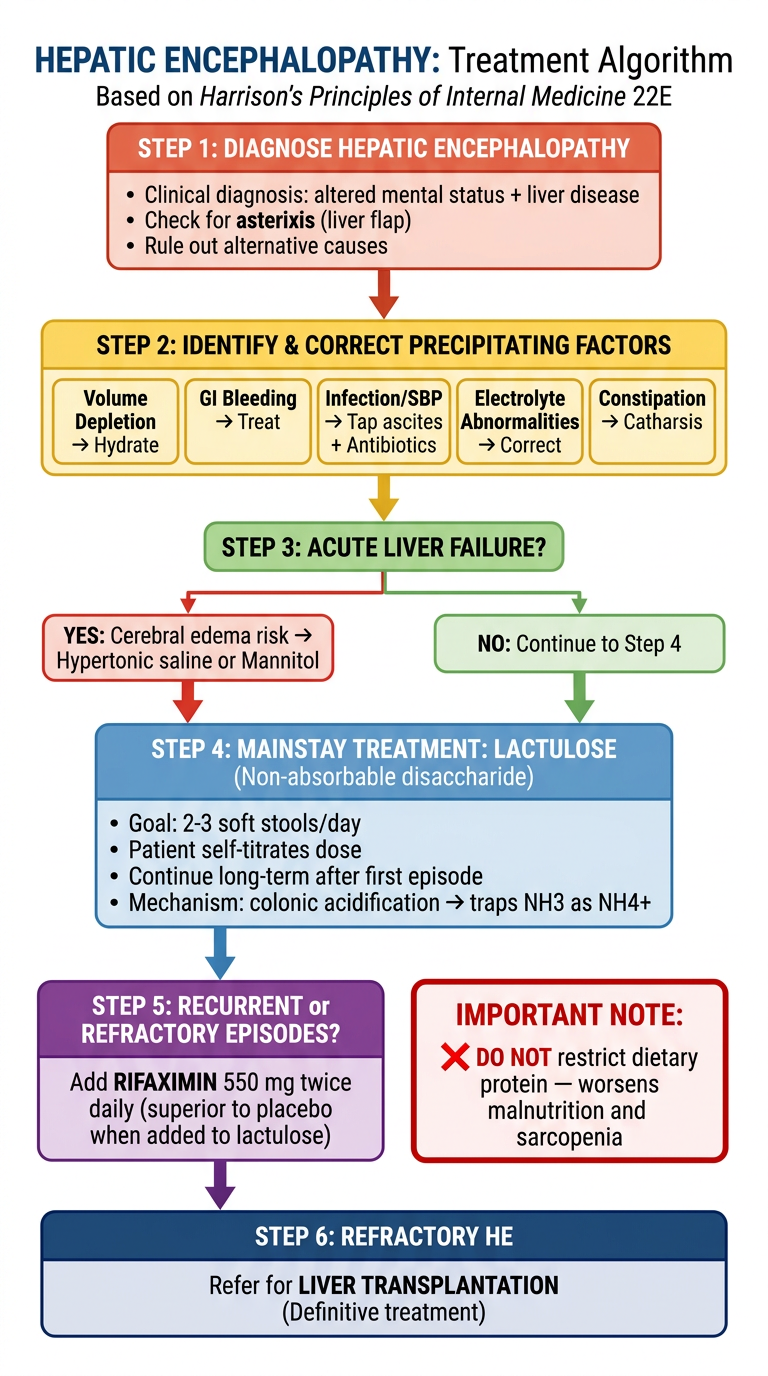
- Diagnose HE - clinical diagnosis with asterixis
- Identify and correct precipitants - the 5 key triggers (volume depletion, GI bleed, infection/SBP, electrolyte abnormalities, constipation)
- Branch for Acute Liver Failure - cerebral edema managed with hypertonic saline or mannitol
- Lactulose as the mainstay treatment (goal: 2-3 soft stools/day)
- Rifaximin 550 mg BID added for recurrent/refractory episodes
- No protein restriction warning (strongly discouraged per Harrison's)
- Liver transplantation for definitive/refractory cases
Ascites ppt based on harrison's
mkdir -p /home/daytona/workspace/ascites-ppt && ls /home/daytona/workspace/ascit…
~/ascites-ppt/create_ascites_ppt.js
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = "LAYOUT_WIDE"; // 13.3" x 7.5"
pres.title = "Ascites - Harrison's Principles of Internal Medicine 22E";
pres.author = "Harrison's PMI 22E";
// ─── COLOR PALETTE ───────────────────────────────────────────────────────────
const DARK_BLUE = "0D2B55"; // dominant navy
const MED_BLUE = "1565C0"; // accent
const LIGHT_BLUE = "E3F0FC"; // slide bg tint
const TEAL = "00796B"; // subheadings
const ORANGE = "E65100"; // warnings / highlights
const WHITE = "FFFFFF";
const LIGHT_GRAY = "F4F7FB";
const MEDIUM_GRAY = "90A4AE";
const DARK_TEXT = "1A2A3A";
const ACCENT_RED = "C62828";
const ACCENT_GOLD = "F9A825";
// ─── HELPER: Slide header band ────────────────────────────────────────────────
function addHeader(slide, title, subtitle) {
// Dark blue top bar
slide.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 13.3, h: 1.0,
fill: { color: DARK_BLUE }, line: { color: DARK_BLUE }
});
// Accent line
slide.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 1.0, w: 13.3, h: 0.06,
fill: { color: ACCENT_GOLD }, line: { color: ACCENT_GOLD }
});
// Title
slide.addText(title, {
x: 0.35, y: 0.08, w: 10, h: 0.55,
fontSize: 22, bold: true, color: WHITE, fontFace: "Calibri", margin: 0
});
if (subtitle) {
slide.addText(subtitle, {
x: 0.35, y: 0.63, w: 10, h: 0.35,
fontSize: 11, color: ACCENT_GOLD, fontFace: "Calibri", margin: 0, italic: true
});
}
// Harrison's badge top right
slide.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 11.2, y: 0.18, w: 1.85, h: 0.62,
fill: { color: MED_BLUE }, line: { color: MED_BLUE }, rectRadius: 0.08
});
slide.addText("Harrison's 22E", {
x: 11.2, y: 0.18, w: 1.85, h: 0.62,
fontSize: 9, bold: true, color: WHITE, align: "center", valign: "middle", fontFace: "Calibri", margin: 0
});
}
// ─── HELPER: Colored box with title + bullets ─────────────────────────────────
function addContentBox(slide, x, y, w, h, headerColor, headerText, bullets, fontSize) {
fontSize = fontSize || 12;
// Header bar
slide.addShape(pres.shapes.RECTANGLE, {
x, y, w, h: 0.42,
fill: { color: headerColor }, line: { color: headerColor }
});
slide.addText(headerText, {
x: x + 0.12, y, w: w - 0.15, h: 0.42,
fontSize: 13, bold: true, color: WHITE, fontFace: "Calibri", valign: "middle", margin: 0
});
// Body
slide.addShape(pres.shapes.RECTANGLE, {
x, y: y + 0.42, w, h: h - 0.42,
fill: { color: LIGHT_GRAY }, line: { color: headerColor, pt: 1.5 }
});
const items = bullets.map((b, i) => ({
text: b,
options: { bullet: true, breakLine: i < bullets.length - 1, fontSize, color: DARK_TEXT, fontFace: "Calibri" }
}));
slide.addText(items, {
x: x + 0.15, y: y + 0.48, w: w - 0.3, h: h - 0.58,
valign: "top"
});
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 1 — TITLE SLIDE
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
// Full background
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 13.3, h: 7.5, fill: { color: DARK_BLUE }, line: { color: DARK_BLUE }
});
// Decorative stripe
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 3.9, w: 13.3, h: 0.09, fill: { color: ACCENT_GOLD }, line: { color: ACCENT_GOLD }
});
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 4.05, w: 13.3, h: 0.04, fill: { color: MED_BLUE }, line: { color: MED_BLUE }
});
s.addText("ASCITES", {
x: 0.8, y: 1.2, w: 11.7, h: 1.5,
fontSize: 72, bold: true, color: WHITE, align: "center", fontFace: "Calibri",
charSpacing: 12
});
s.addText("A Comprehensive Clinical Review", {
x: 0.8, y: 2.8, w: 11.7, h: 0.6,
fontSize: 22, color: ACCENT_GOLD, align: "center", fontFace: "Calibri", italic: true
});
s.addText("Based on Harrison's Principles of Internal Medicine, 22nd Edition (2025)", {
x: 1.5, y: 4.3, w: 10.3, h: 0.5,
fontSize: 14, color: MEDIUM_GRAY, align: "center", fontFace: "Calibri"
});
s.addText("Gastroenterology & Hepatology", {
x: 1.5, y: 4.95, w: 10.3, h: 0.4,
fontSize: 13, color: WHITE, align: "center", fontFace: "Calibri", bold: true
});
// Bottom footnote
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 7.1, w: 13.3, h: 0.4, fill: { color: "0A1F3C" }, line: { color: "0A1F3C" }
});
s.addText("Harrison's Principles of Internal Medicine 22E | Chapter 355: Cirrhosis and Its Complications", {
x: 0.3, y: 7.1, w: 12.7, h: 0.4,
fontSize: 9, color: MEDIUM_GRAY, align: "center", fontFace: "Calibri"
});
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 2 — OVERVIEW & OUTLINE
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:13.3,h:7.5, fill:{color:LIGHT_BLUE}, line:{color:LIGHT_BLUE}});
addHeader(s, "Overview", "Key topics covered in this presentation");
const topics = [
{ num: "01", title: "Definition & Pathogenesis", color: MED_BLUE },
{ num: "02", title: "Clinical Features", color: TEAL },
{ num: "03", title: "Diagnosis & SAAG", color: "6A1B9A" },
{ num: "04", title: "Treatment of Ascites", color: ORANGE },
{ num: "05", title: "Spontaneous Bacterial Peritonitis (SBP)", color: ACCENT_RED },
{ num: "06", title: "Hepatorenal Syndrome (HRS)", color: "37474F" },
{ num: "07", title: "Refractory Ascites", color: MED_BLUE },
];
topics.forEach((t, i) => {
const col = i < 4 ? 0 : 1;
const row = i < 4 ? i : i - 4;
const x = col === 0 ? 0.6 : 7.2;
const y = 1.35 + row * 1.35;
const w = col === 0 ? 6.0 : 5.8;
s.addShape(pres.shapes.RECTANGLE, {
x, y, w, h: 1.1,
fill: { color: t.color }, line: { color: t.color },
shadow: { type: "outer", color: "000000", blur: 6, offset: 2, angle: 135, opacity: 0.15 }
});
s.addText(t.num, {
x: x + 0.1, y, w: 0.6, h: 1.1,
fontSize: 28, bold: true, color: WHITE, valign: "middle", align: "center", fontFace: "Calibri", margin: 0
});
s.addShape(pres.shapes.RECTANGLE, {
x: x + 0.7, y, w: 0.04, h: 1.1, fill: { color: WHITE, transparency: 40 }, line: { color: WHITE, transparency: 40 }
});
s.addText(t.title, {
x: x + 0.85, y, w: w - 0.95, h: 1.1,
fontSize: 16, bold: true, color: WHITE, valign: "middle", fontFace: "Calibri", margin: 0
});
});
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 3 — DEFINITION & PATHOGENESIS
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:13.3,h:7.5, fill:{color:LIGHT_BLUE}, line:{color:LIGHT_BLUE}});
addHeader(s, "Definition & Pathogenesis", "How ascites develops in cirrhosis");
// Definition box
s.addShape(pres.shapes.RECTANGLE, {
x: 0.4, y: 1.25, w: 12.5, h: 0.85,
fill: { color: DARK_BLUE }, line: { color: DARK_BLUE }
});
s.addText([
{ text: "DEFINITION: ", options: { bold: true, color: ACCENT_GOLD, fontSize: 13 } },
{ text: "Ascites is the accumulation of fluid within the peritoneal cavity. The most common cause is ", options: { color: WHITE, fontSize: 13 } },
{ text: "portal hypertension related to cirrhosis", options: { bold: true, color: ACCENT_GOLD, fontSize: 13 } },
{ text: "; malignant, infectious, and cardiac causes must also be considered.", options: { color: WHITE, fontSize: 13 } }
], { x: 0.6, y: 1.28, w: 12.1, h: 0.79, valign: "middle", fontFace: "Calibri" });
// Pathogenesis steps
const steps = [
{ label: "1", title: "↑ Intrahepatic Resistance", desc: "→ Increased portal pressure", color: MED_BLUE },
{ label: "2", title: "Splanchnic Vasodilation", desc: "Nitric oxide → ↑ portal venous inflow", color: TEAL },
{ label: "3", title: "RAAS Activation", desc: "Hyperaldosteronism + sympathetic activation → Na⁺ retention", color: "6A1B9A" },
{ label: "4", title: "Fluid Accumulation", desc: "↓ Oncotic pressure (hypoalbuminemia) → peritoneal fluid", color: ORANGE },
];
steps.forEach((st, i) => {
const x = 0.4 + i * 3.15;
s.addShape(pres.shapes.RECTANGLE, {
x, y: 2.35, w: 3.0, h: 0.62,
fill: { color: st.color }, line: { color: st.color }
});
s.addText(`${st.label}. ${st.title}`, {
x: x + 0.1, y: 2.35, w: 2.8, h: 0.62,
fontSize: 12, bold: true, color: WHITE, valign: "middle", fontFace: "Calibri", margin: 0
});
s.addShape(pres.shapes.RECTANGLE, {
x, y: 2.97, w: 3.0, h: 0.85,
fill: { color: LIGHT_GRAY }, line: { color: st.color, pt: 1.5 }
});
s.addText(st.desc, {
x: x + 0.1, y: 2.97, w: 2.8, h: 0.85,
fontSize: 11, color: DARK_TEXT, valign: "middle", fontFace: "Calibri", margin: 0
});
// Arrow between boxes
if (i < 3) {
s.addText("→", {
x: x + 3.0, y: 2.55, w: 0.15, h: 0.45,
fontSize: 18, bold: true, color: MED_BLUE, align: "center", valign: "middle", margin: 0
});
}
});
// Result
s.addShape(pres.shapes.RECTANGLE, {
x: 0.4, y: 4.05, w: 12.5, h: 0.55,
fill: { color: ACCENT_RED }, line: { color: ACCENT_RED }
});
s.addText("NET RESULT: Fluid constantly leaks into the peritoneal cavity; vascular filling is never achieved — the cycle continues.", {
x: 0.55, y: 4.05, w: 12.2, h: 0.55,
fontSize: 12, bold: true, color: WHITE, valign: "middle", fontFace: "Calibri", margin: 0
});
// Grades
s.addText("Grading of Ascites", {
x: 0.4, y: 4.8, w: 12.5, h: 0.4,
fontSize: 14, bold: true, color: DARK_BLUE, fontFace: "Calibri"
});
const grades = [
{ g: "Grade 1", d: "Detectable only by ultrasonography", c: TEAL },
{ g: "Grade 2", d: "Detectable on physical examination (shifting dullness)", c: MED_BLUE },
{ g: "Grade 3", d: "Marked abdominal distension (massive)", c: ACCENT_RED },
];
grades.forEach((gr, i) => {
const x = 0.4 + i * 4.2;
s.addShape(pres.shapes.RECTANGLE, { x, y: 5.2, w: 4.0, h: 0.42, fill:{color: gr.c}, line:{color: gr.c}});
s.addText(gr.g, { x: x+0.1, y: 5.2, w: 3.8, h: 0.42, fontSize: 13, bold: true, color: WHITE, valign: "middle", fontFace: "Calibri", margin:0 });
s.addShape(pres.shapes.RECTANGLE, { x, y: 5.62, w: 4.0, h: 0.65, fill:{color: LIGHT_GRAY}, line:{color: gr.c, pt:1.5}});
s.addText(gr.d, { x: x+0.1, y: 5.62, w: 3.8, h: 0.65, fontSize: 11, color: DARK_TEXT, valign: "middle", fontFace: "Calibri", margin:0 });
});
// Footer
s.addText("Harrison's Principles of Internal Medicine 22E | Chapter 355", {
x: 0, y: 7.15, w: 13.3, h: 0.35, fontSize: 8, color: MEDIUM_GRAY, align: "center", fontFace: "Calibri"
});
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 4 — CLINICAL FEATURES & DIAGNOSIS
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:13.3,h:7.5, fill:{color:LIGHT_BLUE}, line:{color:LIGHT_BLUE}});
addHeader(s, "Clinical Features & Diagnosis", "Symptoms, signs, and diagnostic workup");
// Left column - Clinical Features
addContentBox(s, 0.35, 1.25, 5.9, 3.0, MED_BLUE, "Clinical Features", [
"Increasing abdominal girth (often insidious)",
"Peripheral edema accompanying fluid accumulation",
"At least 1–2 L needed before patient notices",
"Dyspnea if ascites is massive (diaphragm pressure)",
"Hepatic hydrothorax — more common on the right",
"Muscle wasting, fatigue, and weakness in massive ascites",
"Bulging flanks on examination",
"Fluid wave or shifting dullness on percussion",
], 11);
// Right column - Diagnosis
addContentBox(s, 6.6, 1.25, 6.35, 3.0, TEAL, "Diagnostic Workup", [
"Physical exam: shifting dullness, fluid wave",
"Ultrasound/CT: detect subtle amounts",
"Diagnostic paracentesis recommended on first presentation",
"Ascitic fluid: total protein, albumin, cell count + differential, cultures",
"In cirrhosis: protein usually <2.5 g/dL",
"Amylase if pancreatic ascites suspected; cytology if malignancy suspected",
"Bedside blood culture bottles for cultures (higher yield)",
], 11);
// SAAG section
s.addShape(pres.shapes.RECTANGLE, {
x: 0.35, y: 4.45, w: 12.6, h: 0.42,
fill: { color: "6A1B9A" }, line: { color: "6A1B9A" }
});
s.addText("SERUM ASCITES-ALBUMIN GRADIENT (SAAG)", {
x: 0.5, y: 4.45, w: 12.3, h: 0.42,
fontSize: 14, bold: true, color: WHITE, valign: "middle", fontFace: "Calibri", margin: 0
});
// SAAG formula
s.addShape(pres.shapes.RECTANGLE, {
x: 0.35, y: 4.87, w: 3.4, h: 0.75,
fill: { color: WHITE }, line: { color: "6A1B9A", pt: 2 }
});
s.addText("SAAG = Serum Albumin − Ascitic Fluid Albumin", {
x: 0.45, y: 4.87, w: 3.3, h: 0.75,
fontSize: 11, bold: true, color: "6A1B9A", valign: "middle", align: "center", fontFace: "Calibri", margin: 0
});
const saagData = [
{ label: "SAAG ≥ 1.1 g/dL", title: "Portal Hypertension", examples: "Cirrhosis, cardiac ascites, Budd-Chiari, portal vein thrombosis", color: MED_BLUE },
{ label: "SAAG < 1.1 g/dL", title: "Non-Portal Hypertension", examples: "Malignancy, TB peritonitis, pancreatic ascites, nephrotic syndrome", color: ACCENT_RED },
];
saagData.forEach((d, i) => {
const x = 4.0 + i * 4.45;
s.addShape(pres.shapes.RECTANGLE, { x, y: 4.87, w: 4.25, h: 0.42, fill:{color: d.color}, line:{color: d.color}});
s.addText(`${d.label} → ${d.title}`, { x: x+0.1, y: 4.87, w: 4.1, h: 0.42, fontSize: 12, bold: true, color: WHITE, valign: "middle", fontFace: "Calibri", margin: 0});
s.addShape(pres.shapes.RECTANGLE, { x, y: 5.29, w: 4.25, h: 0.33, fill:{color: LIGHT_GRAY}, line:{color: d.color, pt:1.5}});
s.addText(`e.g. ${d.examples}`, { x: x+0.1, y: 5.29, w: 4.1, h: 0.33, fontSize: 9, color: DARK_TEXT, valign: "middle", fontFace: "Calibri", margin: 0});
});
s.addText("Sensitivity and specificity of SAAG ≥ 1.1 for portal hypertension: ~97%", {
x: 0.35, y: 5.75, w: 12.6, h: 0.35,
fontSize: 11, color: "6A1B9A", bold: true, fontFace: "Calibri"
});
s.addText("Harrison's Principles of Internal Medicine 22E | Chapter 355", {
x: 0, y: 7.15, w: 13.3, h: 0.35, fontSize: 8, color: MEDIUM_GRAY, align: "center", fontFace: "Calibri"
});
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 5 — TREATMENT OF ASCITES
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:13.3,h:7.5, fill:{color:LIGHT_BLUE}, line:{color:LIGHT_BLUE}});
addHeader(s, "Treatment of Ascites", "Stepwise management based on Harrison's 22E");
// Step 1
s.addShape(pres.shapes.RECTANGLE, { x:0.35, y:1.28, w:12.6, h:0.42, fill:{color:TEAL}, line:{color:TEAL}});
s.addText("STEP 1: Sodium Restriction — ALL Patients", { x:0.5, y:1.28, w:12.3, h:0.42, fontSize:14, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0 });
s.addShape(pres.shapes.RECTANGLE, { x:0.35, y:1.7, w:12.6, h:0.55, fill:{color:LIGHT_GRAY}, line:{color:TEAL, pt:1.5}});
s.addText("Restrict dietary sodium to 2 g/day (~¾ tsp salt). Avoid canned/processed foods; prefer fresh or frozen foods. Sodium pamphlets are helpful.", {
x:0.5, y:1.7, w:12.3, h:0.55, fontSize:12, color:DARK_TEXT, valign:"middle", fontFace:"Calibri", margin:0 });
// Step 2 - Diuretics
s.addShape(pres.shapes.RECTANGLE, { x:0.35, y:2.42, w:12.6, h:0.42, fill:{color:MED_BLUE}, line:{color:MED_BLUE}});
s.addText("STEP 2: Diuretic Therapy — Moderate Ascites", { x:0.5, y:2.42, w:12.3, h:0.42, fontSize:14, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0 });
// Two drug boxes
const drugs = [
{ name: "Spironolactone", start: "100 mg/day", max: "400 mg/day", notes: "Aldosterone antagonist — inhibits Na⁺ reabsorption in distal tubule. May cause gynecomastia (switch to amiloride 5–40 mg/d), hyperkalemia, hyponatremia", color: "6A1B9A" },
{ name: "Furosemide", start: "40 mg/day", max: "160 mg/day", notes: "Loop diuretic — used in combination with spironolactone at ratio 40:100. Add especially when peripheral edema is present", color: ORANGE },
];
drugs.forEach((d, i) => {
const x = 0.35 + i * 6.3;
s.addShape(pres.shapes.RECTANGLE, { x, y:2.84, w:6.1, h:0.38, fill:{color:d.color}, line:{color:d.color}});
s.addText(d.name, { x:x+0.1, y:2.84, w:5.9, h:0.38, fontSize:13, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
s.addShape(pres.shapes.RECTANGLE, { x, y:3.22, w:6.1, h:1.05, fill:{color:LIGHT_GRAY}, line:{color:d.color, pt:1.5}});
s.addText([
{ text: `Starting dose: ${d.start} | Max: ${d.max}\n`, options: { bold: true, fontSize: 11, color: DARK_TEXT } },
{ text: d.notes, options: { fontSize: 10, color: DARK_TEXT } }
], { x:x+0.12, y:3.22, w:5.86, h:1.05, valign:"top", fontFace:"Calibri" });
});
// Failure note
s.addShape(pres.shapes.RECTANGLE, { x:0.35, y:4.35, w:12.6, h:0.38, fill:{color:ACCENT_RED, transparency:15}, line:{color:ACCENT_RED}});
s.addText("⚠ Failure of diuretics → first check dietary compliance. If compliant, escalate doses incrementally to maximum before declaring refractory.", {
x:0.5, y:4.35, w:12.3, h:0.38, fontSize:11, color:ACCENT_RED, bold:true, valign:"middle", fontFace:"Calibri", margin:0 });
// Drugs to avoid
s.addShape(pres.shapes.RECTANGLE, { x:0.35, y:4.85, w:12.6, h:0.38, fill:{color:"37474F"}, line:{color:"37474F"}});
s.addText("DRUGS TO AVOID in patients with cirrhosis + ascites:", { x:0.5, y:4.85, w:6, h:0.38, fontSize:12, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
s.addShape(pres.shapes.RECTANGLE, { x:0.35, y:5.23, w:12.6, h:0.55, fill:{color:LIGHT_GRAY}, line:{color:"37474F", pt:1.5}});
s.addText("NSAIDs (risk of renal failure) | Aminoglycosides (nephrotoxic) | ACE inhibitors / ARBs (use with caution — monitor BP and renal function closely)", {
x:0.5, y:5.23, w:12.3, h:0.55, fontSize:11.5, color:DARK_TEXT, valign:"middle", fontFace:"Calibri", margin:0 });
// Prognosis note
s.addShape(pres.shapes.RECTANGLE, { x:0.35, y:5.9, w:12.6, h:0.45, fill:{color:DARK_BLUE}, line:{color:DARK_BLUE}});
s.addText("Prognosis: <50% of patients survive 2 years after onset of ascites → Consider liver transplantation referral", {
x:0.5, y:5.9, w:12.3, h:0.45, fontSize:12, color:ACCENT_GOLD, bold:true, valign:"middle", fontFace:"Calibri", margin:0});
s.addText("Harrison's Principles of Internal Medicine 22E | Chapter 355", {
x:0, y:7.15, w:13.3, h:0.35, fontSize:8, color:MEDIUM_GRAY, align:"center", fontFace:"Calibri" });
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 6 — REFRACTORY ASCITES
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:13.3,h:7.5, fill:{color:LIGHT_BLUE}, line:{color:LIGHT_BLUE}});
addHeader(s, "Refractory Ascites", "Definition, pharmacologic options, and procedural management");
// Definition
s.addShape(pres.shapes.RECTANGLE, { x:0.35, y:1.28, w:12.6, h:0.42, fill:{color:ACCENT_RED}, line:{color:ACCENT_RED}});
s.addText("DEFINITION OF REFRACTORY ASCITES", { x:0.5, y:1.28, w:12.3, h:0.42, fontSize:14, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
s.addShape(pres.shapes.RECTANGLE, { x:0.35, y:1.7, w:12.6, h:0.62, fill:{color:LIGHT_GRAY}, line:{color:ACCENT_RED, pt:1.5}});
s.addText([
{ text: "Diuretic-Resistant: ", options: { bold: true, color: ACCENT_RED } },
{ text: "Persistence of ascites despite sodium restriction + maximum diuretic doses (spiro 400 mg/d + furosemide 160 mg/d) | ", options: { color: DARK_TEXT } },
{ text: "Diuretic-Intractable: ", options: { bold: true, color: MED_BLUE } },
{ text: "Development of side effects that preclude maximum doses", options: { color: DARK_TEXT } },
], { x:0.5, y:1.7, w:12.3, h:0.62, fontSize:11.5, valign:"middle", fontFace:"Calibri" });
// Pharmacologic additions
s.addText("Pharmacologic Additions", { x:0.35, y:2.5, w:5.5, h:0.38, fontSize:13, bold:true, color:DARK_BLUE, fontFace:"Calibri" });
const drugs2 = [
{ name: "Midodrine", detail: "α1-adrenergic agonist\nCounteracts splanchnic vasodilation\nImproves hemodynamics + ascites control", color: "6A1B9A" },
{ name: "Clonidine", detail: "α2-adrenergic agonist\nUsed alone or combined with midodrine\nFurther reduces sympathetic activity", color: TEAL },
{ name: "⚠ Beta-Blockers", detail: "Often used for variceal prophylaxis\nIn refractory ascites: associated with\nDECREASED SURVIVAL — use with caution", color: ACCENT_RED },
];
drugs2.forEach((d, i) => {
const x = 0.35 + i * 4.2;
s.addShape(pres.shapes.RECTANGLE, { x, y:2.9, w:4.0, h:0.38, fill:{color:d.color}, line:{color:d.color}});
s.addText(d.name, { x:x+0.1, y:2.9, w:3.8, h:0.38, fontSize:12, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
s.addShape(pres.shapes.RECTANGLE, { x, y:3.28, w:4.0, h:0.85, fill:{color:LIGHT_GRAY}, line:{color:d.color, pt:1.5}});
s.addText(d.detail, { x:x+0.1, y:3.28, w:3.8, h:0.85, fontSize:10, color:DARK_TEXT, valign:"middle", fontFace:"Calibri", margin:0});
});
// Procedural
s.addText("Procedural Management", { x:0.35, y:4.3, w:8, h:0.38, fontSize:13, bold:true, color:DARK_BLUE, fontFace:"Calibri" });
const procedures = [
{ name: "Large-Volume Paracentesis (LVP)", detail: "Remove >5 L of ascitic fluid\nMust give IV 25% albumin: 6–8 g/L of ascites removed\nPrevents post-paracentesis circulatory dysfunction and death\nRepeated as needed", color: MED_BLUE },
{ name: "TIPS (Transjugular Intrahepatic Portosystemic Shunt)", detail: "Decompresses hepatic sinusoids\nSuperior to LVP for reaccumulation\nNo mortality benefit over LVP\nAssociated with ↑ hepatic encephalopathy\nConsider case-by-case", color: ORANGE },
{ name: "Liver Transplantation", detail: "Definitive treatment\nConsidered in all patients with ascites given poor prognosis (<50% survive 2 years)\nEvaluation should begin early", color: DARK_BLUE },
];
procedures.forEach((p, i) => {
const x = 0.35 + i * 4.3;
s.addShape(pres.shapes.RECTANGLE, { x, y:4.72, w:4.1, h:0.45, fill:{color:p.color}, line:{color:p.color}});
s.addText(p.name, { x:x+0.1, y:4.72, w:3.9, h:0.45, fontSize:10.5, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
s.addShape(pres.shapes.RECTANGLE, { x, y:5.17, w:4.1, h:1.5, fill:{color:LIGHT_GRAY}, line:{color:p.color, pt:1.5}});
s.addText(p.detail, { x:x+0.12, y:5.17, w:3.86, h:1.5, fontSize:10, color:DARK_TEXT, valign:"top", fontFace:"Calibri", margin:0});
});
s.addText("Harrison's Principles of Internal Medicine 22E | Chapter 355", {
x:0, y:7.15, w:13.3, h:0.35, fontSize:8, color:MEDIUM_GRAY, align:"center", fontFace:"Calibri" });
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 7 — SPONTANEOUS BACTERIAL PERITONITIS (SBP)
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:13.3,h:7.5, fill:{color:LIGHT_BLUE}, line:{color:LIGHT_BLUE}});
addHeader(s, "Spontaneous Bacterial Peritonitis (SBP)", "A common and life-threatening complication of ascites");
// Key stats
const stats = [
{ val: "~30%", label: "Incidence in hospitalized cirrhosis patients", color: ACCENT_RED },
{ val: "25%", label: "In-hospital mortality rate", color: ORANGE },
{ val: ">250", label: "Neutrophils/μL in ascitic fluid = diagnostic threshold", color: MED_BLUE },
];
stats.forEach((st, i) => {
const x = 0.35 + i * 4.3;
s.addShape(pres.shapes.RECTANGLE, { x, y:1.28, w:4.1, h:0.85, fill:{color:st.color}, line:{color:st.color}});
s.addText(st.val, { x, y:1.28, w:4.1, h:0.5, fontSize:26, bold:true, color:WHITE, align:"center", valign:"middle", fontFace:"Calibri", margin:0});
s.addText(st.label, { x:x+0.1, y:1.73, w:3.9, h:0.4, fontSize:9.5, color:WHITE, align:"center", fontFace:"Calibri", margin:0});
});
// Left - Pathogenesis + Organisms
addContentBox(s, 0.35, 2.35, 6.0, 2.6, "37474F", "Pathogenesis & Organisms", [
"Mechanism: bacterial translocation — gut flora traverse intestine into mesenteric lymph nodes → bacteremia → seeding of ascitic fluid",
"Most common: Escherichia coli and other gram-negative gut bacteria",
"Gram-positive: Streptococcus viridans, Staphylococcus aureus, Enterococcus spp.",
"If >2 organisms identified → suspect secondary peritonitis (perforated viscus)",
], 11);
// Right - Clinical Features
addContentBox(s, 6.7, 2.35, 6.25, 2.6, TEAL, "Clinical Presentation (may be subtle!)", [
"Fever",
"Abdominal pain or discomfort",
"Altered mental status",
"Elevated WBC count",
"Acute kidney injury",
"⚠ May present without ANY of these features → High clinical suspicion required",
"Peritoneal tap recommended in all cirrhosis patients hospitalized with ascites",
], 11);
// Treatment
s.addShape(pres.shapes.RECTANGLE, { x:0.35, y:5.1, w:12.6, h:0.42, fill:{color:MED_BLUE}, line:{color:MED_BLUE}});
s.addText("TREATMENT", { x:0.5, y:5.1, w:12.3, h:0.42, fontSize:14, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
const txts = [
{ t: "Antibiotic", d: "IV 3rd-generation cephalosporin × 5 days\n(Cefotaxime / Ceftriaxone)" , c: MED_BLUE},
{ t: "Albumin (mandatory)", d: "IV Albumin:\n Day 1: 1.5 g/kg body weight\n Day 3: 1.0 g/kg body weight\nReduces renal failure & improves survival", c: TEAL},
{ t: "Prophylaxis", d: "GI bleeding: SBP prophylaxis at presentation\nPost-SBP: Quinolone antibiotic long-term to prevent recurrence", c: "6A1B9A"},
];
txts.forEach((t, i) => {
const x = 0.35 + i * 4.3;
s.addShape(pres.shapes.RECTANGLE, { x, y:5.52, w:4.1, h:0.38, fill:{color:t.c}, line:{color:t.c}});
s.addText(t.t, { x:x+0.1, y:5.52, w:3.9, h:0.38, fontSize:11, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
s.addShape(pres.shapes.RECTANGLE, { x, y:5.9, w:4.1, h:1.0, fill:{color:LIGHT_GRAY}, line:{color:t.c, pt:1.5}});
s.addText(t.d, { x:x+0.1, y:5.9, w:3.9, h:1.0, fontSize:10, color:DARK_TEXT, valign:"top", fontFace:"Calibri", margin:0});
});
s.addText("Harrison's Principles of Internal Medicine 22E | Chapter 355", {
x:0, y:7.15, w:13.3, h:0.35, fontSize:8, color:MEDIUM_GRAY, align:"center", fontFace:"Calibri" });
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 8 — HEPATORENAL SYNDROME
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:13.3,h:7.5, fill:{color:LIGHT_BLUE}, line:{color:LIGHT_BLUE}});
addHeader(s, "Hepatorenal Syndrome (HRS)", "Functional renal failure in advanced cirrhosis");
// Definition box
s.addShape(pres.shapes.RECTANGLE, { x:0.35, y:1.28, w:12.6, h:0.75, fill:{color:DARK_BLUE}, line:{color:DARK_BLUE}});
s.addText("Functional renal failure without renal pathology; occurs in ~10% of patients with advanced cirrhosis or acute liver failure. Marked renal vasoconstriction + reduced systemic vascular resistance.", {
x:0.5, y:1.28, w:12.3, h:0.75, fontSize:12, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
// Types
s.addText("Classification", { x:0.35, y:2.18, w:5, h:0.38, fontSize:13, bold:true, color:DARK_BLUE, fontFace:"Calibri"});
const types = [
{ type: "HRS-AKI (Type 1 HRS)", def: "Rapid progressive renal impairment\n• Creatinine rise ≥0.3 mg/dL in 48h, OR ≥50% from baseline\n• Poor prognosis", color: ACCENT_RED },
{ type: "HRS-CKD (Type 2 HRS)", def: "Stable reduction in GFR\n• Persistent ↑ creatinine\n• Associated with refractory ascites\n• Relatively better outcome than Type 1", color: ORANGE },
];
types.forEach((t, i) => {
const x = 0.35 + i * 6.3;
s.addShape(pres.shapes.RECTANGLE, { x, y:2.58, w:6.1, h:0.42, fill:{color:t.color}, line:{color:t.color}});
s.addText(t.type, { x:x+0.1, y:2.58, w:5.9, h:0.42, fontSize:12, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
s.addShape(pres.shapes.RECTANGLE, { x, y:3.0, w:6.1, h:0.92, fill:{color:LIGHT_GRAY}, line:{color:t.color, pt:1.5}});
s.addText(t.def, { x:x+0.12, y:3.0, w:5.86, h:0.92, fontSize:11, color:DARK_TEXT, valign:"top", fontFace:"Calibri", margin:0});
});
// Diagnosis
s.addShape(pres.shapes.RECTANGLE, { x:0.35, y:4.1, w:12.6, h:0.42, fill:{color:TEAL}, line:{color:TEAL}});
s.addText("Diagnosis — Exclusion Required (HRS-AKI)", { x:0.5, y:4.1, w:12.3, h:0.42, fontSize:14, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
s.addShape(pres.shapes.RECTANGLE, { x:0.35, y:4.52, w:12.6, h:0.65, fill:{color:LIGHT_GRAY}, line:{color:TEAL, pt:1.5}});
s.addText("1. Stop diuretics | 2. Infuse albumin 1 g/kg/day × 48 hrs without improvement | 3. Exclude intrinsic kidney disease (ATN, AIN, GN) and obstructive uropathy", {
x:0.5, y:4.52, w:12.3, h:0.65, fontSize:11.5, color:DARK_TEXT, valign:"middle", fontFace:"Calibri", margin:0});
// Treatment
s.addShape(pres.shapes.RECTANGLE, { x:0.35, y:5.32, w:12.6, h:0.42, fill:{color:MED_BLUE}, line:{color:MED_BLUE}});
s.addText("TREATMENT — in order of preference", { x:0.5, y:5.32, w:12.3, h:0.42, fontSize:14, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
const hrsTx = [
{ line: "1st Line: Vasoconstrictors", detail: "Terlipressin (preferred) or Norepinephrine (requires ICU monitoring)", c: ACCENT_RED },
{ line: "2nd Line: Midodrine + Octreotide + IV Albumin", detail: "Used in the US (terlipressin availability limited); now considered 3rd line per Harrison's 22E", c: ORANGE },
{ line: "Dialysis / RRT", detail: "If vasoconstrictors fail; bridge to transplant", c: "37474F" },
{ line: "Liver Transplantation", detail: "BEST therapy — recovery of renal function typical", c: DARK_BLUE },
];
hrsTx.forEach((t, i) => {
const x = 0.35 + i * 3.15;
s.addShape(pres.shapes.RECTANGLE, { x, y:5.74, w:3.0, h:0.38, fill:{color:t.c}, line:{color:t.c}});
s.addText(t.line, { x:x+0.08, y:5.74, w:2.84, h:0.38, fontSize:9, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
s.addShape(pres.shapes.RECTANGLE, { x, y:6.12, w:3.0, h:0.7, fill:{color:LIGHT_GRAY}, line:{color:t.c, pt:1.5}});
s.addText(t.detail, { x:x+0.08, y:6.12, w:2.84, h:0.7, fontSize:9, color:DARK_TEXT, valign:"top", fontFace:"Calibri", margin:0});
});
s.addText("Harrison's Principles of Internal Medicine 22E | Chapter 355", {
x:0, y:7.15, w:13.3, h:0.35, fontSize:8, color:MEDIUM_GRAY, align:"center", fontFace:"Calibri" });
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 9 — SUMMARY & KEY TAKE-AWAYS
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:13.3,h:7.5, fill:{color:DARK_BLUE}, line:{color:DARK_BLUE}});
s.addShape(pres.shapes.RECTANGLE, { x:0, y:1.08, w:13.3, h:0.06, fill:{color:ACCENT_GOLD}, line:{color:ACCENT_GOLD}});
s.addShape(pres.shapes.RECTANGLE, { x:0, y:6.8, w:13.3, h:0.06, fill:{color:ACCENT_GOLD}, line:{color:ACCENT_GOLD}});
s.addText("KEY TAKE-AWAYS", {
x:0.5, y:0.22, w:12.3, h:0.78, fontSize:30, bold:true, color:WHITE, align:"center", fontFace:"Calibri", charSpacing:6
});
const points = [
{ icon: "1", text: "Cirrhosis + portal hypertension accounts for >80% of ascites — always consider SAAG to differentiate", color: MED_BLUE },
{ icon: "2", text: "SAAG ≥ 1.1 g/dL → portal hypertension; SAAG < 1.1 → non-portal cause (malignancy, TB, nephrotic syndrome)", color: TEAL },
{ icon: "3", text: "Treatment: Sodium restriction (2 g/day) → Spironolactone + Furosemide (ratio 100:40) → Escalate to max → LVP / TIPS for refractory cases", color: "6A1B9A" },
{ icon: "4", text: "Always give IV albumin 6–8 g/L after LVP of ≥5 L to prevent post-paracentesis circulatory dysfunction", color: ORANGE },
{ icon: "5", text: "SBP: diagnose if ascitic neutrophils >250/µL → Treat with IV 3rd-gen cephalosporin + albumin (1.5 g/kg day 1, 1.0 g/kg day 3)", color: ACCENT_RED },
{ icon: "6", text: "HRS: best treated with liver transplantation. Use terlipressin/norepinephrine as vasoconstrictors; avoid NSAIDs, aminoglycosides, ACE inhibitors", color: "00838F" },
{ icon: "7", text: "Prognosis is poor (<50% survive 2 years) — refer all eligible patients for liver transplant evaluation early", color: ACCENT_GOLD },
];
points.forEach((p, i) => {
const col = i < 4 ? 0 : 1;
const row = i < 4 ? i : i - 4;
const x = col === 0 ? 0.4 : 6.85;
const y = 1.28 + row * 1.3;
const w = col === 0 ? 6.2 : 6.1;
s.addShape(pres.shapes.RECTANGLE, { x, y, w:0.55, h:1.1, fill:{color:p.color}, line:{color:p.color}});
s.addText(p.icon, { x, y, w:0.55, h:1.1, fontSize:22, bold:true, color:WHITE, align:"center", valign:"middle", fontFace:"Calibri", margin:0});
s.addShape(pres.shapes.RECTANGLE, { x:x+0.55, y, w:w-0.55, h:1.1, fill:{color:"0A1F3C"}, line:{color:p.color, pt:1}});
s.addText(p.text, { x:x+0.68, y, w:w-0.75, h:1.1, fontSize:11, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
});
// Bottom reference
s.addText("Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025) | Chapters 39 & 355", {
x:0, y:6.88, w:13.3, h:0.6, fontSize:10, color:MEDIUM_GRAY, align:"center", valign:"middle", fontFace:"Calibri"
});
}
// ─────────────────────────────────────────────────────────────────────────────
// WRITE FILE
// ─────────────────────────────────────────────────────────────────────────────
pres.writeFile({ fileName: "/home/daytona/workspace/ascites-ppt/Ascites_Harrisons_22E.pptx" })
.then(() => console.log("SUCCESS: /home/daytona/workspace/ascites-ppt/Ascites_Harrisons_22E.pptx"))
.catch(err => { console.error("ERROR:", err); process.exit(1); });
cd /home/daytona/workspace/ascites-ppt && node create_ascites_ppt.js
Ascites Harrisons 22E
Presentation · PPTX
| Slide | Content |
|---|---|
| 1 | Title slide |
| 2 | Overview / outline (7 topics) |
| 3 | Definition & Pathogenesis (4-step mechanism + grading) |
| 4 | Clinical Features, Diagnosis & SAAG interpretation |
| 5 | Treatment - sodium restriction, spironolactone + furosemide, drugs to avoid, prognosis |
| 6 | Refractory Ascites - definition, midodrine/clonidine, LVP, TIPS, transplant |
| 7 | Spontaneous Bacterial Peritonitis (SBP) - diagnosis, organisms, treatment with albumin |
| 8 | Hepatorenal Syndrome (HRS) - HRS-AKI vs HRS-CKD, diagnosis, treatment hierarchy |
| 9 | Key Take-Aways summary (7 high-yield points) |
Ppt on Rheumatoid arthritis with images based on harrison's
"cdn.orris.care" in /textbooks/9781265977061
node /home/daytona/skills/shared/scripts/fetch_images.js \ "https://cdn.orris.…
node /home/daytona/skills/shared/scripts/fetch_images.js \ "https://cdn.orris.…
~/ascites-ppt/create_ra_ppt.js
const pptxgen = require("pptxgenjs");
const fs = require("fs");
const pres = new pptxgen();
pres.layout = "LAYOUT_WIDE"; // 13.3" x 7.5"
pres.title = "Rheumatoid Arthritis - Harrison's PMI 22E";
// ─── PALETTE ──────────────────────────────────────────────────────────────────
const DARK = "1A1A2E"; // deep navy-black
const NAVY = "16213E"; // slide backgrounds (dark slides)
const TEAL = "0F3460"; // section headers
const ACCENT = "E94560"; // hot coral accent
const GOLD = "F5A623"; // highlight / warning
const TEAL_LIGHT = "00B4D8"; // info boxes
const GREEN = "00897B"; // positive / treatment
const PURPLE = "7B2D8B"; // autoantibodies
const ORANGE = "E65100"; // warnings
const WHITE = "FFFFFF";
const LIGHT_BG = "F0F4F8";
const CARD_BG = "FFFFFF";
const DARK_TEXT = "1A2A3A";
const GRAY = "90A4AE";
const LIGHT_TEAL = "E0F7FA";
// ─── Image data ───────────────────────────────────────────────────────────────
const img0 = fs.readFileSync("/tmp/ra_img0.b64", "utf8"); // global prevalence map
// ─── HELPERS ──────────────────────────────────────────────────────────────────
function hdr(s, title, sub) {
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:13.3,h:0.95, fill:{color:TEAL}, line:{color:TEAL}});
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0.95,w:13.3,h:0.06, fill:{color:ACCENT}, line:{color:ACCENT}});
s.addText(title, { x:0.35,y:0.08,w:10,h:0.52, fontSize:22, bold:true, color:WHITE, fontFace:"Calibri", margin:0});
if(sub) s.addText(sub, { x:0.35,y:0.6,w:10,h:0.3, fontSize:11, color:GOLD, fontFace:"Calibri", italic:true, margin:0});
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x:11.2,y:0.18,w:1.85,h:0.6, fill:{color:ACCENT}, line:{color:ACCENT}, rectRadius:0.08});
s.addText("Harrison's 22E", { x:11.2,y:0.18,w:1.85,h:0.6, fontSize:9, bold:true, color:WHITE, align:"center", valign:"middle", fontFace:"Calibri", margin:0});
}
function foot(s) {
s.addText("Harrison's Principles of Internal Medicine 22E | Chapter 370: Rheumatoid Arthritis", {
x:0,y:7.17,w:13.3,h:0.33, fontSize:8, color:GRAY, align:"center", fontFace:"Calibri"});
}
function box(s, x, y, w, h, hColor, title, lines, fs_) {
fs_ = fs_||11;
s.addShape(pres.shapes.RECTANGLE, { x,y,w,h:0.4, fill:{color:hColor}, line:{color:hColor}});
s.addText(title, { x:x+0.1,y,w:w-0.15,h:0.4, fontSize:13, bold:true, color:WHITE, fontFace:"Calibri", valign:"middle", margin:0});
s.addShape(pres.shapes.RECTANGLE, { x,y:y+0.4,w,h:h-0.4, fill:{color:LIGHT_BG}, line:{color:hColor, pt:1.5}});
const items = lines.map((b,i)=>({ text:b, options:{ bullet:true, breakLine:i<lines.length-1, fontSize:fs_, color:DARK_TEXT, fontFace:"Calibri"}}));
s.addText(items, { x:x+0.14,y:y+0.46,w:w-0.28,h:h-0.56, valign:"top"});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 1 — TITLE
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
// Dark gradient background via shapes
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:13.3,h:7.5, fill:{color:NAVY}, line:{color:NAVY}});
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:5.5,h:7.5, fill:{color:TEAL}, line:{color:TEAL}});
s.addShape(pres.shapes.RECTANGLE, { x:5.5,y:0,w:0.06,h:7.5, fill:{color:ACCENT}, line:{color:ACCENT}});
// Title text on dark right side
s.addText("RHEUMATOID", { x:5.8,y:1.0,w:7.2,h:1.0, fontSize:52, bold:true, color:WHITE, fontFace:"Calibri", charSpacing:4});
s.addText("ARTHRITIS", { x:5.8,y:1.95,w:7.2,h:1.0, fontSize:52, bold:true, color:ACCENT, fontFace:"Calibri", charSpacing:4});
s.addShape(pres.shapes.RECTANGLE, { x:5.8,y:3.05,w:7.1,h:0.05, fill:{color:GOLD}, line:{color:GOLD}});
s.addText("A Comprehensive Clinical Review", { x:5.8,y:3.2,w:7.1,h:0.45, fontSize:18, color:GOLD, fontFace:"Calibri", italic:true});
s.addText("Based on Harrison's Principles of Internal Medicine\n22nd Edition (2025)", {
x:5.8,y:3.85,w:7.1,h:0.8, fontSize:13, color:GRAY, fontFace:"Calibri"});
// Left-side topic pills
const topics = ["Epidemiology","Pathogenesis","Clinical Features","Diagnosis & Criteria","DMARDs & Biologics","Treatment Algorithm","Extra-articular Features","Prognosis"];
topics.forEach((t,i)=>{
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x:0.2,y:0.3+i*0.88,w:5.1,h:0.7, fill:{color:"0A2240", transparency:0}, line:{color:TEAL_LIGHT, pt:1}, rectRadius:0.06});
s.addText(`${String(i+1).padStart(2,'0')} ${t}`, { x:0.35,y:0.3+i*0.88,w:4.9,h:0.7, fontSize:13, color:WHITE, fontFace:"Calibri", valign:"middle", margin:0});
});
s.addText("Chapter 370 | Rheumatology | Internal Medicine", { x:5.8,y:7.0,w:7.2,h:0.4, fontSize:9, color:GRAY, fontFace:"Calibri"});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 2 — EPIDEMIOLOGY & RISK FACTORS (with prevalence map image)
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:13.3,h:7.5, fill:{color:LIGHT_BG}, line:{color:LIGHT_BG}});
hdr(s,"Epidemiology & Risk Factors","Global burden, genetics, and environmental triggers");
// Stats row
const stats = [
{ v:"0.5–1%", l:"Global prevalence", c:TEAL },
{ v:"3:1", l:"Female-to-Male ratio", c:ACCENT },
{ v:"40-60y", l:"Peak onset age", c:GREEN },
{ v:"~60%", l:"Risk attributed to genetics", c:PURPLE },
{ v:"1.5–3.5×",l:"Smoking risk increase", c:ORANGE },
];
stats.forEach((st,i)=>{
const x = 0.3+i*2.54;
s.addShape(pres.shapes.RECTANGLE, { x,y:1.22,w:2.4,h:0.65, fill:{color:st.c}, line:{color:st.c}});
s.addText(st.v, { x,y:1.22,w:2.4,h:0.42, fontSize:20, bold:true, color:WHITE, align:"center", fontFace:"Calibri", margin:0});
s.addText(st.l, { x:x+0.05,y:1.59,w:2.3,h:0.28, fontSize:8.5, color:WHITE, align:"center", fontFace:"Calibri", margin:0});
});
// Left content boxes
box(s, 0.3, 2.07, 5.9, 2.3, TEAL, "Genetic Risk Factors",[
"HLA-DRB1 shared epitope (SE) — major risk allele",
"*0401/*0404 in Northern Europeans (50–70%); *0405/*0901 in Asians",
"Pima/Tlingit Native Americans: prevalence up to 7% (*1042 allele)",
"PTPN22 gene — regulates T/B cell function; absent in East Asians",
"PADI4 gene — encodes enzyme converting arginine → citrulline",
">100 non-MHC loci identified by GWAS; individually modest effect",
],10.5);
box(s, 0.3, 4.52, 5.9, 2.5, ORANGE, "Environmental Risk Factors",[
"Cigarette smoking: RR 1.5–3.5×; synergizes with SE alleles → 20–40× risk",
"Risk persists 15 years after smoking cessation",
"Almost exclusively ACPA/RF-positive disease",
"Silica inhalation and inhalant occupations",
"Periodontal disease / Porphyromonas gingivalis (PAD enzyme → citrullination)",
"Gut and oral microbiome dysbiosis — emerging evidence",
],10.5);
// Right: Prevalence map image
s.addShape(pres.shapes.RECTANGLE, { x:6.45,y:2.07,w:6.6,h:4.3, fill:{color:WHITE}, line:{color:TEAL, pt:1.5}});
s.addText("FIGURE 370-1 Global Prevalence & Genetic Associations of RA", { x:6.55,y:2.1,w:6.4,h:0.38, fontSize:10, bold:true, color:TEAL, fontFace:"Calibri", margin:0});
s.addImage({ data: img0, x:6.5,y:2.52,w:6.5,h:3.6 });
s.addText("HLA-DRB1 mutations are found globally; specific alleles vary by ethnicity. (Harrison's 22E)", { x:6.5,y:6.17,w:6.5,h:0.3, fontSize:8, color:GRAY, fontFace:"Calibri", italic:true });
foot(s);
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 3 — PATHOGENESIS
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:13.3,h:7.5, fill:{color:LIGHT_BG}, line:{color:LIGHT_BG}});
hdr(s,"Pathogenesis","Autoimmune cascade driving synovial inflammation and joint destruction");
// Cascade flow
const steps = [
{ n:"1", t:"Genetic + Environmental Trigger", d:"SE alleles + smoking → citrullination of self-proteins (ACPA generation)", c:TEAL },
{ n:"2", t:"Autoantibody Production", d:"RF + ACPA produced years before clinical disease. Immune complex deposition in synovium", c:PURPLE },
{ n:"3", t:"Synovial T-cell Activation", d:"CD4+ T cells, B cells infiltrate synovium. Th1/Th17 polarization → cytokine release", c:ACCENT },
{ n:"4", t:"Cytokine Storm", d:"TNF-α, IL-1, IL-6, IL-17 drive pannus formation. Synoviocyte (FLS) proliferation", c:ORANGE },
{ n:"5", t:"Pannus & Joint Destruction", d:"Aggressive granulation tissue (pannus) erodes cartilage and bone. RANKL activates osteoclasts", c:ACCENT },
];
steps.forEach((st,i)=>{
const x = 0.25 + i*2.58;
s.addShape(pres.shapes.RECTANGLE, { x,y:1.22,w:0.6,h:3.2, fill:{color:st.c}, line:{color:st.c}});
s.addText(st.n, { x,y:1.22,w:0.6,h:0.6, fontSize:20, bold:true, color:WHITE, align:"center", valign:"middle", fontFace:"Calibri", margin:0});
s.addShape(pres.shapes.RECTANGLE, { x:x+0.6,y:1.22,w:1.88,h:0.62, fill:{color:st.c}, line:{color:st.c}});
s.addText(st.t, { x:x+0.65,y:1.22,w:1.78,h:0.62, fontSize:11, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
s.addShape(pres.shapes.RECTANGLE, { x:x+0.6,y:1.84,w:1.88,h:2.58, fill:{color:WHITE}, line:{color:st.c, pt:1.5}});
s.addText(st.d, { x:x+0.7,y:1.9,w:1.68,h:2.4, fontSize:10, color:DARK_TEXT, valign:"top", fontFace:"Calibri", margin:0});
if(i<4) s.addText("→", { x:x+2.49,y:2.5,w:0.2,h:0.5, fontSize:20, bold:true, color:st.c, align:"center", valign:"middle", margin:0});
});
// Key mediators
s.addShape(pres.shapes.RECTANGLE, { x:0.25,y:4.62,w:12.8,h:0.42, fill:{color:NAVY}, line:{color:NAVY}});
s.addText("KEY THERAPEUTIC TARGETS in the Pathogenesis Cascade:", { x:0.4,y:4.62,w:12.5,h:0.42, fontSize:12, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
const tgts = [
{ label:"TNF-α", rx:"Etanercept, Infliximab, Adalimumab, Certolizumab, Golimumab", c:ACCENT },
{ label:"IL-6R", rx:"Tocilizumab, Sarilumab", c:TEAL },
{ label:"CD80/86 (T-cell co-stim)", rx:"Abatacept", c:PURPLE },
{ label:"CD20 (B cells)", rx:"Rituximab", c:GREEN },
{ label:"JAK1/2/3", rx:"Tofacitinib, Baricitinib, Upadacitinib", c:ORANGE },
];
tgts.forEach((t,i)=>{
const x = 0.25 + i*2.58;
s.addShape(pres.shapes.RECTANGLE, { x,y:5.04,w:2.45,h:0.42, fill:{color:t.c}, line:{color:t.c}});
s.addText(t.label, { x:x+0.06,y:5.04,w:2.35,h:0.42, fontSize:11, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
s.addShape(pres.shapes.RECTANGLE, { x,y:5.46,w:2.45,h:0.85, fill:{color:LIGHT_BG}, line:{color:t.c, pt:1.5}});
s.addText(t.rx, { x:x+0.07,y:5.46,w:2.31,h:0.85, fontSize:9, color:DARK_TEXT, valign:"middle", fontFace:"Calibri", margin:0});
});
foot(s);
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 4 — CLINICAL FEATURES
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:13.3,h:7.5, fill:{color:LIGHT_BG}, line:{color:LIGHT_BG}});
hdr(s,"Clinical Features","Articular and extra-articular manifestations");
// Articular features
box(s, 0.3,1.2, 4.1, 3.35, TEAL, "Articular Features",[
"Symmetric polyarthritis — hallmark",
"Small joints of hands/wrists/feet first affected",
"Morning stiffness >1 hour (disease activity marker)",
"MCP, PIP joints involved (NOT DIP)",
"Pain, swelling, warmth, tenderness on palpation",
"Soft tissue swelling vs bony enlargement (OA)",
"Pannus erosion → deformity over time",
"Boutonniere deformity, Swan-neck deformity",
"Ulnar deviation of fingers",
"Z-deformity of thumb",
],10.5);
// Joint deformities illustration box
s.addShape(pres.shapes.RECTANGLE, { x:4.55,y:1.2,w:3.6,h:3.35, fill:{color:WHITE}, line:{color:TEAL, pt:1.5}});
s.addText("Joint Deformities in RA", { x:4.65,y:1.25,w:3.4,h:0.4, fontSize:12, bold:true, color:TEAL, fontFace:"Calibri", margin:0});
const deforms = [
{ d:"Boutonnière", m:"PIP flexion + DIP hyperextension" },
{ d:"Swan-neck", m:"PIP hyperextension + DIP flexion" },
{ d:"Ulnar deviation", m:"MCP joint drift toward ulna" },
{ d:"Z-thumb", m:"MCP flexion + IP hyperextension" },
{ d:"Piano-key sign", m:"Subluxation of distal ulna" },
{ d:"Atlanto-axial subluxation", m:"Cervical spine — neurological emergency" },
];
deforms.forEach((d,i)=>{
s.addShape(pres.shapes.RECTANGLE, { x:4.65,y:1.7+i*0.4,w:1.3,h:0.36, fill:{color:TEAL, transparency:i%2===0?0:30}, line:{color:TEAL}});
s.addText(d.d, { x:4.67,y:1.7+i*0.4,w:1.27,h:0.36, fontSize:9, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
s.addShape(pres.shapes.RECTANGLE, { x:5.95,y:1.7+i*0.4,w:2.1,h:0.36, fill:{color:LIGHT_BG}, line:{color:TEAL, pt:0.8}});
s.addText(d.m, { x:6.0,y:1.7+i*0.4,w:2.0,h:0.36, fontSize:9, color:DARK_TEXT, valign:"middle", fontFace:"Calibri", margin:0});
});
// Extra-articular features
s.addShape(pres.shapes.RECTANGLE, { x:8.3,y:1.2,w:4.7,h:3.35, fill:{color:WHITE}, line:{color:ACCENT, pt:1.5}});
s.addShape(pres.shapes.RECTANGLE, { x:8.3,y:1.2,w:4.7,h:0.4, fill:{color:ACCENT}, line:{color:ACCENT}});
s.addText("Extra-articular Features", { x:8.4,y:1.2,w:4.5,h:0.4, fontSize:13, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
const eaf = [
{ sys:"Skin", feat:"Rheumatoid nodules (20–30%), vasculitis" },
{ sys:"Pulmonary", feat:"ILD (UIP/NSIP), pleuritis, nodules, Caplan syndrome" },
{ sys:"Cardiac", feat:"Pericarditis, myocarditis, ↑ CVD risk" },
{ sys:"Eye", feat:"Keratoconjunctivitis sicca, scleritis, episcleritis" },
{ sys:"Haematologic", feat:"Felty syndrome (RA + neutropenia + splenomegaly)" },
{ sys:"Neurologic", feat:"Mononeuritis multiplex, cervical myelopathy" },
{ sys:"Renal", feat:"Amyloidosis (secondary), drug-related" },
{ sys:"Systemic", feat:"Fatigue, weight loss, low-grade fever" },
];
eaf.forEach((e,i)=>{
s.addShape(pres.shapes.RECTANGLE, { x:8.35,y:1.65+i*0.34,w:1.05,h:0.3, fill:{color:ACCENT, transparency:i%2===0?0:25}, line:{color:ACCENT}});
s.addText(e.sys, { x:8.37,y:1.65+i*0.34,w:1.0,h:0.3, fontSize:8.5, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
s.addShape(pres.shapes.RECTANGLE, { x:9.4,y:1.65+i*0.34,w:3.5,h:0.3, fill:{color:LIGHT_BG}, line:{color:ACCENT, pt:0.8}});
s.addText(e.feat, { x:9.45,y:1.65+i*0.34,w:3.4,h:0.3, fontSize:8.5, color:DARK_TEXT, valign:"middle", fontFace:"Calibri", margin:0});
});
// Disease activity & labs
s.addShape(pres.shapes.RECTANGLE, { x:0.3,y:4.7,w:12.7,h:0.4, fill:{color:NAVY}, line:{color:NAVY}});
s.addText("Laboratory Findings & Autoantibodies", { x:0.45,y:4.7,w:12.4,h:0.4, fontSize:13, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
const labs = [
{ l:"RF (Rheumatoid Factor)", d:"IgM anti-IgG. Positive in ~75–80%. NOT specific — also in SLE, Sjögren's, infections, healthy elderly", c:PURPLE },
{ l:"Anti-CCP (ACPA)", d:"Highly specific (~95%) and sensitive (~70%). Predictive of erosive disease. Present years before symptoms", c:TEAL },
{ l:"ESR / CRP", d:"Elevated in active disease. Useful to monitor response to treatment. CRP also predicts CV risk", c:GREEN },
{ l:"ANA", d:"Positive in ~30% of RA patients. Low titer. Does not indicate SLE", c:ORANGE },
];
labs.forEach((l,i)=>{
const x=0.3+i*3.17;
s.addShape(pres.shapes.RECTANGLE, { x,y:5.1,w:3.05,h:0.38, fill:{color:l.c}, line:{color:l.c}});
s.addText(l.l, { x:x+0.08,y:5.1,w:2.89,h:0.38, fontSize:10, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
s.addShape(pres.shapes.RECTANGLE, { x,y:5.48,w:3.05,h:1.35, fill:{color:LIGHT_BG}, line:{color:l.c, pt:1.5}});
s.addText(l.d, { x:x+0.09,y:5.53,w:2.87,h:1.25, fontSize:9.5, color:DARK_TEXT, valign:"top", fontFace:"Calibri", margin:0});
});
foot(s);
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 5 — 2010 ACR/EULAR CLASSIFICATION CRITERIA
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:13.3,h:7.5, fill:{color:LIGHT_BG}, line:{color:LIGHT_BG}});
hdr(s,"2010 ACR/EULAR Classification Criteria for RA","Score ≥6/10 = definite RA (requires at least 1 joint with synovitis not explained by another diagnosis)");
// Score table
s.addShape(pres.shapes.RECTANGLE, { x:0.3,y:1.22,w:12.7,h:0.45, fill:{color:TEAL}, line:{color:TEAL}});
const cols = ["DOMAIN","FINDING","SCORE"];
const cx = [0.35, 3.2, 12.35];
const cw = [2.8, 8.95, 0.6];
cols.forEach((c,i)=> s.addText(c, { x:cx[i],y:1.22,w:cw[i],h:0.45, fontSize:12, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0, align: i===2?"center":"left"}));
const criteria = [
{ dom:"Joint Involvement", find:"1 large joint (shoulder, elbow, hip, knee, ankle)", score:"0" },
{ dom:"", find:"2–10 large joints", score:"1" },
{ dom:"", find:"1–3 small joints (MCP, PIP, wrist, 2nd–5th MTP)", score:"2" },
{ dom:"", find:"4–10 small joints", score:"3" },
{ dom:"", find:">10 joints (at least 1 small joint)", score:"5" },
{ dom:"Serology", find:"Negative RF AND negative ACPA", score:"0" },
{ dom:"", find:"Low-positive RF OR low-positive ACPA (≤3× ULN)", score:"2" },
{ dom:"", find:"High-positive RF OR high-positive ACPA (>3× ULN)", score:"3" },
{ dom:"Acute-Phase Reactants", find:"Normal CRP AND normal ESR", score:"0" },
{ dom:"", find:"Abnormal CRP OR abnormal ESR", score:"1" },
{ dom:"Duration of Symptoms", find:"<6 weeks", score:"0" },
{ dom:"", find:"≥6 weeks", score:"1" },
];
const rowColors = [TEAL,TEAL,"","","",PURPLE,PURPLE,PURPLE,GREEN,GREEN,ORANGE,ORANGE];
criteria.forEach((r,i)=>{
const y = 1.67 + i*0.42;
const bg = i%2===0 ? WHITE : LIGHT_BG;
s.addShape(pres.shapes.RECTANGLE, { x:0.3,y,w:12.7,h:0.42, fill:{color:bg}, line:{color:"D0D8E0", pt:0.5}});
if(r.dom) {
s.addShape(pres.shapes.RECTANGLE, { x:0.3,y,w:2.85,h:0.42, fill:{color:rowColors[i]||TEAL}, line:{color:rowColors[i]||TEAL}});
s.addText(r.dom, { x:0.38,y,w:2.7,h:0.42, fontSize:10, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
}
s.addText(r.find, { x:3.25,y,w:8.8,h:0.42, fontSize:10, color:DARK_TEXT, valign:"middle", fontFace:"Calibri", margin:0});
s.addShape(pres.shapes.RECTANGLE, { x:12.25,y,w:0.75,h:0.42, fill:{color:Number(r.score)>=3?ACCENT:Number(r.score)>=1?GOLD:LIGHT_BG}, line:{color:"D0D8E0"}});
s.addText(r.score, { x:12.25,y,w:0.75,h:0.42, fontSize:12, bold:true, color:Number(r.score)>=1?WHITE:DARK_TEXT, align:"center", valign:"middle", fontFace:"Calibri", margin:0});
});
s.addShape(pres.shapes.RECTANGLE, { x:0.3,y:6.7,w:12.7,h:0.42, fill:{color:ACCENT}, line:{color:ACCENT}});
s.addText("SCORE ≥ 6/10 = DEFINITE RHEUMATOID ARTHRITIS", { x:0.4,y:6.7,w:12.5,h:0.42, fontSize:13, bold:true, color:WHITE, align:"center", valign:"middle", fontFace:"Calibri", margin:0});
foot(s);
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 6 — TREATMENT OVERVIEW
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:13.3,h:7.5, fill:{color:LIGHT_BG}, line:{color:LIGHT_BG}});
hdr(s,"Treatment of Rheumatoid Arthritis","Treat-to-target: goal is remission or low disease activity");
// Principle
s.addShape(pres.shapes.RECTANGLE, { x:0.3,y:1.22,w:12.7,h:0.55, fill:{color:NAVY}, line:{color:NAVY}});
s.addText([
{ text:"Treat-to-Target (T2T): ", options:{ bold:true, color:GOLD, fontSize:12 }},
{ text:"Target is remission (DAS28 <2.6) or low disease activity. Reassess every 1–3 months. Escalate DMARD therapy if target not met within 3–6 months.", options:{ color:WHITE, fontSize:12 }},
],{ x:0.45,y:1.22,w:12.4,h:0.55, valign:"middle", fontFace:"Calibri"});
// Drug categories
const cats = [
{ title:"NSAIDs", color:TEAL_LIGHT, tc:TEAL,
points:["Adjunctive agents only (not disease-modifying)","COX-1 and COX-2 inhibition → analgesic + anti-inflammatory","Minimize chronic use: GI toxicity (peptic ulcer, gastritis), renal injury","Roughly equivalent efficacy; individual response varies"] },
{ title:"Glucocorticoids", color:"FFF3E0", tc:ORANGE,
points:["Bridge therapy while DMARD takes effect (weeks–months)","Acute flare management: short burst (1–2 weeks)","Chronic low-dose: ≤5–10 mg/day prednisone","⚠ Long-term risks: osteoporosis, infection, metabolic effects","Intra-articular injection for mono/oligoarticular flare"] },
{ title:"csDMARDs (Conventional)", color:"E8F5E9", tc:GREEN,
points:["Methotrexate (MTX): DRUG OF CHOICE for early RA","Start MTX 7.5–15 mg/week; up to 25 mg/week","Always supplement with folic acid","Other csDMARDs: hydroxychloroquine, sulfasalazine, leflunomide","Triple therapy (MTX + HCQ + SSZ) = proven superiority over MTX alone"] },
];
cats.forEach((c,i)=>{
const x=0.3+i*4.28;
s.addShape(pres.shapes.RECTANGLE, { x,y:1.95,w:4.1,h:0.42, fill:{color:c.tc}, line:{color:c.tc}});
s.addText(c.title, { x:x+0.1,y:1.95,w:3.9,h:0.42, fontSize:13, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
s.addShape(pres.shapes.RECTANGLE, { x,y:2.37,w:4.1,h:2.35, fill:{color:LIGHT_BG}, line:{color:c.tc, pt:1.5}});
const items=c.points.map((p,j)=>({ text:p, options:{ bullet:true, breakLine:j<c.points.length-1, fontSize:10.5, color:DARK_TEXT, fontFace:"Calibri"}}));
s.addText(items, { x:x+0.12,y:2.43,w:3.86,h:2.23, valign:"top"});
});
// Biologic section header
s.addShape(pres.shapes.RECTANGLE, { x:0.3,y:4.85,w:12.7,h:0.42, fill:{color:ACCENT}, line:{color:ACCENT}});
s.addText("BIOLOGIC DMARDs (bDMARDs) — Used when csDMARDs are inadequate", { x:0.45,y:4.85,w:12.4,h:0.42, fontSize:13, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
const bios = [
{ n:"Anti-TNF", d:"Etanercept, Infliximab, Adalimumab, Certolizumab, Golimumab", c:ACCENT },
{ n:"Anti-IL-6R", d:"Tocilizumab, Sarilumab", c:TEAL },
{ n:"Anti-CD80/86", d:"Abatacept (CTLA4-Ig)\nT-cell co-stimulation blockade", c:PURPLE },
{ n:"Anti-CD20", d:"Rituximab\nB-cell depletion", c:GREEN },
{ n:"JAK Inhibitors", d:"Tofacitinib, Baricitinib, Upadacitinib\n(tsDMARDs — oral)", c:ORANGE },
];
bios.forEach((b,i)=>{
const x=0.3+i*2.55;
s.addShape(pres.shapes.RECTANGLE, { x,y:5.27,w:2.42,h:0.4, fill:{color:b.c}, line:{color:b.c}});
s.addText(b.n, { x:x+0.08,y:5.27,w:2.26,h:0.4, fontSize:11, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
s.addShape(pres.shapes.RECTANGLE, { x,y:5.67,w:2.42,h:1.15, fill:{color:LIGHT_BG}, line:{color:b.c, pt:1.5}});
s.addText(b.d, { x:x+0.09,y:5.7,w:2.24,h:1.1, fontSize:9, color:DARK_TEXT, valign:"top", fontFace:"Calibri", margin:0});
});
foot(s);
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 7 — DMARDs TABLE
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:13.3,h:7.5, fill:{color:LIGHT_BG}, line:{color:LIGHT_BG}});
hdr(s,"Key DMARDs — Dosing, Mechanism & Toxicity","Based on Table 370-3, Harrison's 22E");
const hdr2 = ["Drug","Mechanism","Dose","Key Toxicities","Monitoring"];
const hx=[0.25,2.4,5.0,6.65,10.0]; const hw=[2.1,2.55,1.6,3.3,3.05];
s.addShape(pres.shapes.RECTANGLE, { x:0.25,y:1.22,w:12.8,h:0.42, fill:{color:NAVY}, line:{color:NAVY}});
hdr2.forEach((h,i)=> s.addText(h, { x:hx[i]+0.05,y:1.22,w:hw[i]-0.1,h:0.42, fontSize:11, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0}));
const rows=[
{ drug:"Methotrexate", mech:"Inhibits DHFR; anti-inflammatory via adenosine", dose:"7.5–25 mg/wk", tox:"Hepatotoxicity, mucositis, myelosuppression, teratogenic, pneumonitis", mon:"LFTs, CBC, Cr q4–8wk; avoid alcohol", c:GREEN},
{ drug:"Hydroxychloroquine", mech:"Inhibits TLR signalling, lysosomal acidification", dose:"≤5 mg/kg/d", tox:"Retinal toxicity (maculopathy)", mon:"Annual ophthalmology exam", c:TEAL},
{ drug:"Sulfasalazine", mech:"Anti-inflammatory; unknown exact mechanism", dose:"1–1.5 g BID", tox:"GI upset, rash, leukopenia, hepatitis", mon:"CBC, LFTs q3mo", c:TEAL_LIGHT},
{ drug:"Leflunomide", mech:"Inhibits pyrimidine synthesis (DHODH)", dose:"20 mg/d", tox:"Hepatotoxicity, HTN, teratogenic, diarrhea", mon:"LFTs, BP monthly × 6mo then q6mo", c:PURPLE},
{ drug:"Adalimumab", mech:"Monoclonal Ab; neutralizes TNF-α", dose:"40 mg q2wk SC",tox:"Infection (TB reactivation), demyelination, lymphoma risk", mon:"TB screen before start; CBC, LFTs", c:ACCENT},
{ drug:"Etanercept", mech:"Fusion protein; binds TNF-α + TNF-β", dose:"50 mg/wk SC", tox:"Injection site reactions, infection, heart failure", mon:"TB screen before start", c:ACCENT},
{ drug:"Tocilizumab", mech:"Blocks IL-6 receptor (soluble + membrane-bound)", dose:"162 mg/wk SC", tox:"↑ LFTs, ↑ lipids, GI perforation, cytopenias", mon:"LFTs, lipids, CBC q4–8wk", c:ORANGE},
{ drug:"Abatacept", mech:"CTLA4-Ig; blocks CD80/CD86:CD28 co-stimulation", dose:"SC weekly or IV monthly", tox:"Infection, COPD exacerbation", mon:"Watch for TB, hepatitis", c:PURPLE},
{ drug:"Rituximab", mech:"Anti-CD20; depletes B lymphocytes", dose:"1000 mg IV ×2 (2wk apart)", tox:"Infusion reaction, PML (rare), immunosuppression", mon:"Immunoglobulin levels before each cycle", c:GREEN},
{ drug:"Tofacitinib", mech:"JAK1/3 inhibitor → blocks cytokine signalling", dose:"5 mg BID oral",tox:"VTE (↑ risk), serious infection, CV risk, malignancy", mon:"CBC, LFTs, lipids; avoid with live vaccines", c:"8D6A9F"},
];
rows.forEach((r,i)=>{
const y=1.64+i*0.54;
const bg=i%2===0?WHITE:LIGHT_BG;
s.addShape(pres.shapes.RECTANGLE, { x:0.25,y,w:12.8,h:0.54, fill:{color:bg}, line:{color:"D0D8E0", pt:0.5}});
s.addShape(pres.shapes.RECTANGLE, { x:0.25,y,w:2.1,h:0.54, fill:{color:r.c}, line:{color:r.c}});
s.addText(r.drug, { x:0.3,y,w:2.0,h:0.54, fontSize:10, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
s.addText(r.mech, { x:hx[1]+0.05,y,w:hw[1]-0.1,h:0.54, fontSize:8.5, color:DARK_TEXT, valign:"middle", fontFace:"Calibri", margin:0});
s.addText(r.dose, { x:hx[2]+0.05,y,w:hw[2]-0.1,h:0.54, fontSize:8.5, color:DARK_TEXT, valign:"middle", fontFace:"Calibri", margin:0});
s.addText(r.tox, { x:hx[3]+0.05,y,w:hw[3]-0.1,h:0.54, fontSize:8, color:DARK_TEXT, valign:"middle", fontFace:"Calibri", margin:0});
s.addText(r.mon, { x:hx[4]+0.05,y,w:hw[4]-0.1,h:0.54, fontSize:8, color:DARK_TEXT, valign:"middle", fontFace:"Calibri", margin:0});
});
foot(s);
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 8 — TREATMENT ALGORITHM
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:13.3,h:7.5, fill:{color:LIGHT_BG}, line:{color:LIGHT_BG}});
hdr(s,"Treatment Algorithm","Step-up strategy with treat-to-target approach (Harrison's 22E + ACR 2021 Guidelines)");
// Step boxes with arrows
const steps = [
{ n:"STEP 1", t:"Diagnosis + Early DMARD Start", d:"Start MTX as soon as possible after diagnosis. Add folic acid.\nBridge with low-dose glucocorticoids if needed.", c:GREEN },
{ n:"STEP 2", t:"Reassess at 3 months", d:"If LDA/remission not achieved:\nEscalate MTX dose to maximum tolerated (25 mg/wk)\nConsider adding HCQ and/or SSZ (triple therapy)", c:TEAL },
{ n:"STEP 3", t:"Moderate–High Disease Activity persists", d:"Add biologic DMARD or JAK inhibitor to MTX:\nFirst choice: Anti-TNF agents (most data)\nAlternatives: abatacept, tocilizumab, rituximab", c:ACCENT },
{ n:"STEP 4", t:"Inadequate response / toxicity", d:"Switch biologic (different mechanism class)\nor switch to JAK inhibitor\nor trial of combination bDMARD strategies", c:PURPLE },
{ n:"STEP 5", t:"Refractory / Ongoing Activity", d:"Re-evaluate diagnosis\nReferral to tertiary rheumatology\nConsider clinical trial enrollment\nAddress comorbidities (CVD, osteoporosis)", c:ORANGE },
];
steps.forEach((st,i)=>{
const y=1.22+i*1.18;
s.addShape(pres.shapes.RECTANGLE, { x:0.3,y,w:1.2,h:0.9, fill:{color:st.c}, line:{color:st.c}});
s.addText(st.n, { x:0.3,y,w:1.2,h:0.9, fontSize:11, bold:true, color:WHITE, align:"center", valign:"middle", fontFace:"Calibri", margin:0});
s.addShape(pres.shapes.RECTANGLE, { x:1.5,y,w:3.0,h:0.9, fill:{color:st.c}, line:{color:st.c}});
s.addText(st.t, { x:1.58,y,w:2.84,h:0.9, fontSize:12, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
s.addShape(pres.shapes.RECTANGLE, { x:4.5,y,w:8.55,h:0.9, fill:{color:LIGHT_BG}, line:{color:st.c, pt:1.5}});
s.addText(st.d, { x:4.62,y:y+0.04,w:8.33,h:0.82, fontSize:11, color:DARK_TEXT, valign:"middle", fontFace:"Calibri", margin:0});
if(i<4) {
s.addShape(pres.shapes.RECTANGLE, { x:0.82,y:y+0.9,w:0.16,h:0.28, fill:{color:st.c}, line:{color:st.c}});
}
});
// Key principle box
s.addShape(pres.shapes.RECTANGLE, { x:0.3,y:7.08,w:12.7,h:0.35, fill:{color:NAVY}, line:{color:NAVY}});
s.addText("Key principle: Escalate therapy every 3 months if treatment target (remission / LDA) not achieved | Combination > Monotherapy in most patients", {
x:0.4,y:7.08,w:12.5,h:0.35, fontSize:9.5, color:GOLD, bold:true, valign:"middle", fontFace:"Calibri", margin:0});
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 9 — DISEASE ACTIVITY INDICES & MONITORING
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:13.3,h:7.5, fill:{color:LIGHT_BG}, line:{color:LIGHT_BG}});
hdr(s,"Disease Activity Measurement & Monitoring","Tools for tracking RA and guiding treatment decisions");
// Indices
s.addShape(pres.shapes.RECTANGLE, { x:0.3,y:1.22,w:6.2,h:0.42, fill:{color:TEAL}, line:{color:TEAL}});
s.addText("Disease Activity Indices", { x:0.4,y:1.22,w:6.0,h:0.42, fontSize:13, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
const indices = [
{ name:"DAS28 (Disease Activity Score)", comp:"28 tender + swollen joint counts, ESR/CRP, patient VAS", use:"<2.6 = remission; 2.6–3.2 = LDA; 3.2–5.1 = MDA; >5.1 = HDA", c:TEAL },
{ name:"SDAI (Simplified DA Index)", comp:"28 SJC + 28 TJC + patient VAS + physician VAS + CRP", use:"≤3.3 = remission; 3.4–11 = LDA", c:GREEN },
{ name:"CDAI (Clinical DA Index)", comp:"28 SJC + 28 TJC + patient VAS + physician VAS (no labs)", use:"≤2.8 = remission; 2.9–10 = LDA; useful in clinical practice", c:PURPLE },
{ name:"ACR 20/50/70 Response", comp:"20/50/70% improvement in joint counts + 3 of 5 other measures", use:"Primary endpoint in clinical trials", c:ORANGE },
{ name:"RAPID3", comp:"Patient self-report only (no joint counts)", use:"Simple; for busy clinical settings", c:TEAL_LIGHT },
];
indices.forEach((r,i)=>{
const y=1.64+i*0.9;
s.addShape(pres.shapes.RECTANGLE, { x:0.3,y,w:2.6,h:0.9, fill:{color:r.c}, line:{color:r.c}});
s.addText(r.name, { x:0.38,y,w:2.44,h:0.9, fontSize:9.5, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
s.addShape(pres.shapes.RECTANGLE, { x:2.9,y,w:1.8,h:0.9, fill:{color:LIGHT_BG}, line:{color:r.c, pt:1}});
s.addText(r.comp, { x:2.97,y,w:1.66,h:0.9, fontSize:8.5, color:DARK_TEXT, valign:"middle", fontFace:"Calibri", margin:0});
s.addShape(pres.shapes.RECTANGLE, { x:4.7,y,w:1.8,h:0.9, fill:{color:LIGHT_BG}, line:{color:r.c, pt:1}});
s.addText(r.use, { x:4.77,y,w:1.66,h:0.9, fontSize:8.5, color:DARK_TEXT, valign:"middle", fontFace:"Calibri", margin:0});
});
// Monitoring right panel
s.addShape(pres.shapes.RECTANGLE, { x:6.75,y:1.22,w:6.25,h:0.42, fill:{color:ACCENT}, line:{color:ACCENT}});
s.addText("Ongoing Monitoring of RA Patients", { x:6.85,y:1.22,w:6.05,h:0.42, fontSize:13, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
const monitors = [
{ cat:"Clinical", items:"Joint counts (TJC/SJC), morning stiffness duration, functional disability (HAQ), patient VAS, physician global assessment" },
{ cat:"Laboratory", items:"CRP, ESR, CBC, LFTs, creatinine — frequency depends on DMARD used (q4–8 weeks when initiating, then q3 months)" },
{ cat:"Imaging", items:"X-rays of hands/feet at baseline and annually to detect erosions. MRI/ultrasound more sensitive for early erosions and synovitis" },
{ cat:"Comorbidities", items:"Cardiovascular risk (RA doubles CV mortality) — screen lipids, BP. Osteoporosis screening — DEXA scan. Infection risk — vaccinate (flu, pneumococcal, zoster)" },
{ cat:"Drug Toxicity", items:"MTX: LFTs, CBC, creatinine. Anti-TNF: TB screen, hepatitis B, infection surveillance. JAK inhibitors: lipids, VTE risk, CBC" },
];
monitors.forEach((m,i)=>{
const y=1.64+i*0.95;
const c=i%2===0?ACCENT:PURPLE;
s.addShape(pres.shapes.RECTANGLE, { x:6.75,y,w:1.4,h:0.95, fill:{color:c}, line:{color:c}});
s.addText(m.cat, { x:6.78,y,w:1.34,h:0.95, fontSize:10, bold:true, color:WHITE, valign:"middle", fontFace:"Calibri", margin:0});
s.addShape(pres.shapes.RECTANGLE, { x:8.15,y,w:4.85,h:0.95, fill:{color:LIGHT_BG}, line:{color:c, pt:1.5}});
s.addText(m.items, { x:8.22,y,w:4.72,h:0.95, fontSize:9.5, color:DARK_TEXT, valign:"middle", fontFace:"Calibri", margin:0});
});
foot(s);
}
// ═══════════════════════════════════════════════════════════════════════════════
// SLIDE 10 — KEY TAKE-AWAYS
// ═══════════════════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x:0,y:0,w:13.3,h:7.5, fill:{color:NAVY}, line:{color:NAVY}});
s.addShape(pres.shapes.RECTANGLE, { x:0,y:1.08,w:13.3,h:0.06, fill:{color:ACCENT}, line:{color:ACCENT}});
s.addShape(pres.shapes.RECTANGLE, { x:0,y:6.9,w:13.3,h:0.06, fill:{color:GOLD}, line:{color:GOLD}});
s.addText("KEY TAKE-AWAYS", {
x:0.5,y:0.18,w:12.3,h:0.82, fontSize:28, bold:true, color:WHITE, align:"center", fontFace:"Calibri", charSpacing:8});
const pts = [
{ n:"1", t:"RA is a symmetric polyarthritis", d:"Predominantly small joints (MCP, PIP, wrists). Morning stiffness >1 hour is hallmark. DIP sparing differentiates from OA.", c:TEAL },
{ n:"2", t:"RF + Anti-CCP (ACPA)", d:"ACPA is highly specific (~95%) and predictive of erosive disease. Present years before symptoms = preclinical RA.", c:PURPLE },
{ n:"3", t:"2010 ACR/EULAR criteria", d:"Score ≥6/10 = definite RA. Domains: joint involvement, serology, acute-phase reactants, symptom duration.", c:GREEN },
{ n:"4", t:"Methotrexate is drug of first choice", d:"csDMARD of choice for early RA. Always give folic acid. Escalate to 25 mg/wk. Triple therapy > monotherapy.", c:GOLD },
{ n:"5", t:"Treat-to-Target (T2T)", d:"Reassess every 1–3 months. Escalate if target (remission/LDA) not met within 3–6 months.", c:ACCENT },
{ n:"6", t:"Biologics for inadequate csDMARD response", d:"Anti-TNF agents are first-line biologics. Alternatives: tocilizumab, abatacept, rituximab. Oral JAK inhibitors available.", c:TEAL_LIGHT },
{ n:"7", t:"Screen before biologics", d:"TB, hepatitis B, varicella screen mandatory. Do not start anti-TNF in active infection.", c:ORANGE },
{ n:"8", t:"RA doubles cardiovascular mortality", d:"Monitor and treat CV risk factors aggressively. Osteoporosis prophylaxis in steroid users.", c:ACCENT },
];
pts.forEach((p,i)=>{
const col=i<4?0:1;
const row=i<4?i:i-4;
const x=col===0?0.3:6.85;
const y=1.22+row*1.35;
const w=6.25;
s.addShape(pres.shapes.RECTANGLE, { x,y,w:0.65,h:1.2, fill:{color:p.c}, line:{color:p.c}});
s.addText(p.n, { x,y,w:0.65,h:1.2, fontSize:22, bold:true, color:WHITE, align:"center", valign:"middle", fontFace:"Calibri", margin:0});
s.addShape(pres.shapes.RECTANGLE, { x:x+0.65,y,w:w-0.65,h:1.2, fill:{color:"0A1F3C"}, line:{color:p.c, pt:1}});
s.addText(p.t, { x:x+0.75,y:y+0.05,w:w-0.8,h:0.4, fontSize:11, bold:true, color:GOLD, fontFace:"Calibri", margin:0});
s.addText(p.d, { x:x+0.75,y:y+0.43,w:w-0.82,h:0.72, fontSize:10, color:"CBD5E0", fontFace:"Calibri", margin:0});
});
s.addText("Source: Harrison's Principles of Internal Medicine 22E (2025) | Chapter 370: Rheumatoid Arthritis", {
x:0,y:6.98,w:13.3,h:0.5, fontSize:9, color:GRAY, align:"center", valign:"middle", fontFace:"Calibri"});
}
// ─── WRITE ────────────────────────────────────────────────────────────────────
pres.writeFile({ fileName:"/home/daytona/workspace/ascites-ppt/RA_Harrisons_22E.pptx" })
.then(()=> console.log("SUCCESS: RA_Harrisons_22E.pptx"))
.catch(err=>{ console.error("ERROR:",err); process.exit(1); });
cd /home/daytona/workspace/ascites-ppt && node create_ra_ppt.js
RA Harrisons 22E
Presentation · PPTX
| Slide | Content |
|---|---|
| 1 | Title slide with 8-topic agenda panel |
| 2 | Epidemiology & Risk Factors - 5 key statistics + genetic risk factors + environmental triggers + embedded Harrison's global prevalence map (Figure 370-1) |
| 3 | Pathogenesis - 5-step cascade (Genetic trigger → Autoantibodies → T-cell activation → Cytokine storm → Pannus/joint destruction) + key therapeutic targets per mechanism |
| 4 | Clinical Features - Articular features, joint deformities table (Boutonnière, Swan-neck, ulnar deviation), extra-articular features by organ system, autoantibodies (RF, ACPA, ESR/CRP, ANA) |
| 5 | 2010 ACR/EULAR Classification Criteria - Full scoring table with color-coded scores (max 10; ≥6 = definite RA) |
| 6 | Treatment Overview - NSAIDs, glucocorticoids, csDMARDs (MTX as drug of choice), biologic DMARDs with 5 mechanism classes |
| 7 | DMARDs Table - 10 drugs with mechanism, dose, key toxicities, and monitoring requirements |
| 8 | Treatment Algorithm - 5-step escalation strategy with treat-to-target principle |
| 9 | Disease Activity Indices & Monitoring - DAS28, SDAI, CDAI, ACR criteria + clinical/lab/imaging/comorbidity monitoring |
| 10 | Key Take-Aways - 8 high-yield clinical pearls |
Find latest EULAR 2024 RA management guidelines with evidence summaries
EULAR recommendations management rheumatoid arthritis
EULAR 2024 rheumatoid arthritis management guidelines update
https://www.news-medical.net/news/20260313/Updated-EULAR-rec…
EULAR recommendations rheumatoid arthritis DMARDs 2025 update Smolen
Smolen EULAR 2025 RA recommendations annals rheumatic diseases DOI 10.1016/j.ard.2026.01.023
PMID: 41826212
PMID: 41997804
PMID: 41951459
https://www.guidelinecentral.com/guideline/5135295
EULAR 2025 RA Management Recommendations
Correct name: "2025 Update" (not 2024) Full citation: Smolen JS, Edwards CJ, Konzett V, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biologic disease-modifying antirheumatic drugs: 2025 update. Ann Rheum Dis. 2026 Jun;85(6):991-1009. doi:10.1016/j.ard.2026.01.023 | PMID: 41826212 Published online: 12 March 2026. This is the 5th update since EULAR first published RA recommendations in 2010.
What Changed vs. 2022?
| Change | Previous (2022) | New (2025) |
|---|---|---|
| Recommendations count | 12 | 9 (streamlined) |
| Risk stratification after first DMARD failure | Stratify by risk factors for bad outcome | Removed - DMARD failure itself is already a risk factor |
| DMARD tapering in sustained remission | Dose reduction "may be considered" | Preference for continuation; tapering still possible but explicit caution added |
| JAK inhibitors | Considered after bDMARD failure | May be considered after csDMARD failure, but risk factors must be assessed first |
| Pre-RA prevention | Not addressed | Acknowledged but insufficient evidence for a recommendation yet |
5 Overarching Principles
- Treatment must be aimed at best care and based on shared decision-making between patient and rheumatologist.
- Treatment decisions are based on disease activity, safety, and other patient factors (comorbidities, structural damage progression).
- Rheumatologists are the specialists who should primarily care for RA patients.
- Patients require access to multiple drugs with different modes of action due to RA heterogeneity; they may require successive therapies throughout life.
- RA incurs high individual, medical, and societal costs - all should be considered in management.
9 Individual Recommendations
Recommendation 1 - Start DMARDs Immediately
- LoE 1a | SoR A
Recommendation 2 - Treat-to-Target (T2T)
- LoE 1a | SoR A
- Monitor every 1-3 months in active disease
- If no improvement by 3 months → adjust therapy
- If target not reached by 6 months → adjust therapy
Recommendation 3 - MTX First
- LoE 1a | SoR A
- If contraindicated or not tolerated early: use leflunomide or sulfasalazine
Recommendation 4 - Glucocorticoids as Bridge
- LoE 1a | SoR A
- Purpose: bridging while awaiting DMARD effect - NOT long-term agents
Recommendation 5 - Escalate to bDMARD After csDMARD Failure
- Efficacy: LoE 1a | SoR A
- Safety: LoE 2a | SoR B
- JAK inhibitor risk factors to assess: MACEs, malignancy, VTE, age >65, long-term smoker, serious cardiovascular risk
Recommendation 6 - Combine bDMARDs/tsDMARDs with csDMARDs
- LoE 1a | SoR A
- Rationale: IL-6 inhibitors and JAKi have efficacy as monotherapy; TNF inhibitors and abatacept are less effective without MTX
Recommendation 7 - Switching After First bDMARD/JAKi Failure
- No mandatory class-switching required
- Both within-class and between-class switching are acceptable
Recommendation 8 - Tapering in Sustained Remission
- LoE 5 | SoR D (key change: explicit preference for continuation over stopping)
- Stopping treatment frequently leads to flare, especially with bDMARDs and JAKi
Recommendation 9 - Safety Monitoring
- JAKi: MACE, malignancy, VTE/PE, herpes zoster
- TNF inhibitors: TB reactivation, infections, demyelination
- All DMARDs: infection risk, immunizations before starting
Evidence Base: Supporting Systematic Literature Reviews
SLR 1 - Efficacy (PMID: 41997804)
- Searched: Jan 2022 - Jan 2025 | 12,567 references screened | 72 studies included
- Key findings:
- Strategic trials confirmed bDMARD/tsDMARD strategies superior to csDMARD monotherapy in inadequate responders
- Precision-medicine approaches (synovial biopsy-guided therapy, therapeutic drug monitoring) show promise but not yet practice-ready
- Evidence on DMARD tapering reinforced caution against stopping
- Nintedanib and pirfenidone evaluated for RA-ILD (included in ILD subgroup)
- 7 studies on DMARDs for RA prevention in at-risk populations - insufficient for recommendation
SLR 2 - Safety (PMID: 41951459)
- Searched: Jan 2022 - Jan 2025 | 3,837 articles | 71 studies included
- Key safety signals:
| Safety Domain | Key Finding |
|---|---|
| Serious infections | More common with bDMARDs than csDMARDs |
| Herpes zoster | Higher with JAKi than bDMARDs |
| Tuberculosis | Higher with infliximab/adalimumab vs etanercept; NOT increased with JAKi vs bDMARDs |
| MACE (cardiac events) | No consistent increased risk with JAKi vs bDMARDs in new data |
| VTE/PE | Elevated with JAKi vs bDMARDs, driven mainly by pulmonary embolism |
| Malignancy | Increased NMSC with DMARDs overall vs general population; no drug-specific link |
| Glucocorticoid safety | Under-studied in this period (surprisingly few new studies) |
Additional 2024 EULAR Update Relevant to RA
Rüegg L, et al. Ann Rheum Dis. 2025;84(6):910-26.
- Methotrexate and leflunomide: contraindicated in pregnancy (teratogenic) - washout required
- Hydroxychloroquine: safe in pregnancy and breastfeeding
- TNF inhibitors: most can be continued into pregnancy (certolizumab has lowest placental transfer)
- JAK inhibitors: avoid in pregnancy - insufficient safety data
Summary: What This Means in Practice
- Start MTX + short-course glucocorticoids immediately on diagnosis
- Reassess at 3 months - escalate if no improvement; target remission/LDA by 6 months
- If csDMARD fails → add bDMARD first (anti-TNF remains first choice by experience); JAKi are an option but screen for cardiovascular risk, VTE risk, malignancy history, and age >65 first
- Any bDMARD/JAKi failure → switch class or within-class - both acceptable
- In sustained remission → keep the DMARD (reduce dose if needed, but don't stop)
- No new drugs approved since 2022 - guidance refined by strategic and safety evidence
Make flowchar on treatment
A professional clinical treatment flowchart for Rheumatoid Arthritis management based on EULAR 2025 recommendations. Clean white background, medical style, color-coded boxes with arrows. Title at top: "RHEUMATOID ARTHRITIS: Treatment Algorithm" with subtitle "EULAR 2025 Recommendations | Smolen et al., Ann Rheum Dis 2026" The flowchart flows top-to-bottom with clear arrows: START BOX (dark navy blue, rounded): "NEW DIAGNOSIS OF RA" with note: "Start DMARDs IMMEDIATELY after diagnosis" ↓ arrow STEP 1 BOX (green): "FIRST-LINE: csDMARD Therapy" • Methotrexate (MTX) — drug of first choice • If MTX contraindicated: Leflunomide or Sulfasalazine • Add short-term Glucocorticoids as bridge (taper ASAP) • Add Folic acid with MTX ↓ arrow DECISION DIAMOND (orange): "Reassess at 3 months — Target achieved? (Remission or LDA)" Two branches: → YES branch (right side, green): "CONTINUE current therapy. Monitor every 1–3 months. If sustained remission → prefer DMARD continuation; dose reduction may be considered" → NO branch (downward, red): "Not at target by 3–6 months → ESCALATE" ↓ from NO STEP 2 BOX (blue): "ADD bDMARD (preferred) or consider JAKi" Preferred bDMARDs: • Anti-TNF: Adalimumab, Etanercept, Infliximab, Certolizumab, Golimumab • Abatacept (anti-CD80/86) • Tocilizumab / Sarilumab (IL-6 inhibitors) • Rituximab (anti-CD20) JAK Inhibitors (assess risk first): ⚠ Screen for: MACE risk, VTE/PE risk, malignancy history, age >65, heavy smoker • Tofacitinib, Baricitinib, Filgotinib, Upadacitinib Important note box (yellow): "Combine bDMARD/JAKi with csDMARD. If csDMARD not tolerated: IL-6i or JAKi preferred (effective as monotherapy)" ↓ arrow DECISION DIAMOND (orange): "Response adequate? Target reached?" → YES (green right branch): "Continue. Sustained remission → prefer continuation, reduce dose cautiously" → NO (red downward): "bDMARD or JAKi failure" ↓ STEP 3 BOX (purple): "SWITCH bDMARD or JAKi" • Switch to different class bDMARD, OR • Switch within same class, OR • Switch to JAKi (if not used; assess risks) • Both within-class and between-class switching acceptable ↓ arrow BOTTOM BOX (dark navy): "Throughout all steps: Reassess every 1–3 months | Glucocorticoids: bridge only — taper and stop | Shared decision-making with patient at every step" Small red warning box on side: "⚠ JAKi Risk Factors — Assess before use: Age >65 | Cardiovascular disease | Prior malignancy | VTE/Pulmonary embolism history | Long-term smoker" The flowchart uses color-coded sections: green for first-line, blue for second-line, purple for third-line, orange for decision points, red arrows for failure paths, green arrows for success paths.
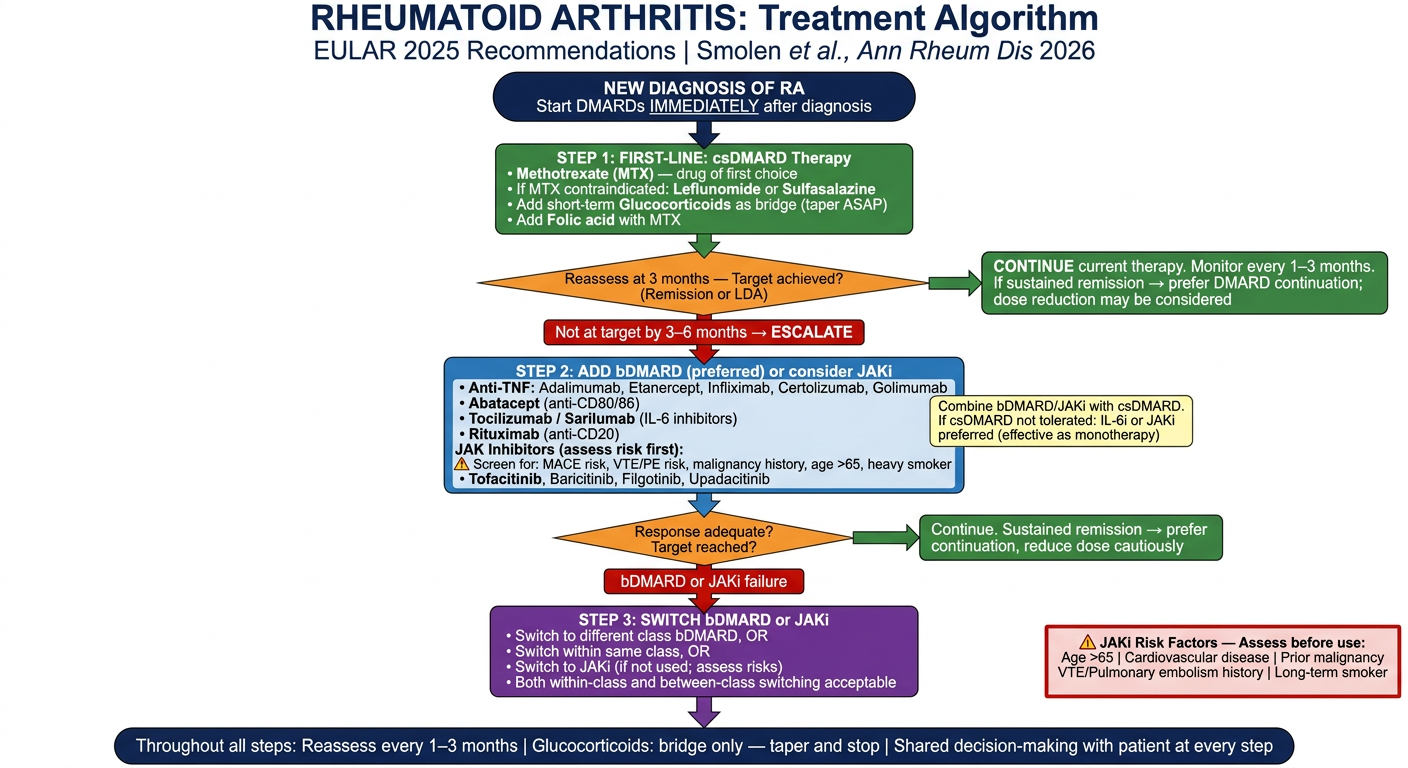
- Yes → Continue + monitor
- No → Escalate
Treatment of tuberculosis based on harrison's
Treatment of Tuberculosis
Part 1: Latent TB Infection (LTBI) Treatment
| Regimen | Dose | Duration | Notes |
|---|---|---|---|
| Isoniazid + Rifapentine (3HP) | INH 900 mg + RPT 900 mg, once weekly | 3 months | Regimen of choice in children >2 yr and all adults including HIV+. DOT recommended. Not for pregnant women. |
| Rifampin alone | 600 mg/day (10 mg/kg) | 4 months | Preferred in HIV-negative individuals; insufficient data for HIV+ |
| Isoniazid + Rifampin | INH 300 mg/d + RIF 600 mg/d | 3 months | Higher hepatotoxicity risk vs individual drugs |
| Isoniazid alone | 300 mg/d (or 900 mg twice weekly) | 6-9 months | 9 months more effective but higher hepatotoxicity; twice-weekly requires DOT |
Key principle: Shorter rifamycin-based regimens (3HP, 4R, or 3HR) are currently preferred over 6-9 months of isoniazid alone in adults and children for effectiveness, safety, and tolerability.
Part 2: Active TB Disease - Drug-Susceptible (Standard Treatment)
Standard 6-Month Regimen (HRZE → HR)
| Phase | Drugs | Duration | Frequency |
|---|---|---|---|
| Intensive phase | HINH + Rifampin + ZPyrazinamide + Ethambutol | 2 months | Daily (preferred); 3×/week with dose adjustment acceptable in non-HIV, non-cavitary |
| Continuation phase | HINH + Rifampin | 4 months | Daily or 5 days/week |
| Total | 6 months |
When to Extend the Continuation Phase
| Situation | Extension |
|---|---|
| HIV+ and NOT on ART | Extend continuation phase to 7 months (total 9 months) |
| Prolonged culture conversion (>2 months) | Extend continuation phase to 7 months |
| Cavitation on chest X-ray | Extend continuation phase to 7 months |
| Culture-negative TB | Continuation phase only 2 months (total 4 months); extend to 4 months if HIV+ |
New 4-Month Regimen (2023/2025 Evidence)
- Rifapentine + Isoniazid + Pyrazinamide + Moxifloxacin (8 weeks) → Rifapentine + Isoniazid + Moxifloxacin (9 weeks)
- Non-inferior to standard 6-month HRZE regimen
- Includes HIV+ patients with CD4 >100
- Conditional recommendation by WHO and US guidelines
- Concerns: higher pill burden, moxifloxacin side effects, need for fluoroquinolone resistance testing in high-resistance areas
Part 3: First-Line Antituberculosis Drugs
Isoniazid (INH / H)
- Mechanism: Prodrug activated by KatG catalase-peroxidase → inhibits InhA (ketoenoyl-reductase) → blocks mycolic acid synthesis + free radical release
- Dose: 300 mg/day (or 5 mg/kg/day); 900 mg twice weekly for intermittent regimens
- Key toxicities: Hepatotoxicity (monitor LFTs), peripheral neuropathy (prevent with pyridoxine 25-50 mg/day), drug-induced lupus
- Always give with pyridoxine (Vitamin B6) 25-50 mg/day to prevent neuropathy
- Diffuses into CSF at concentrations comparable to serum - effective for TB meningitis
- Resistance: ~7-8% primary resistance in the US (katG and inhA gene mutations)
Rifampin (RIF / R)
- Mechanism: Inhibits DNA-dependent RNA polymerase (rpoB gene) → blocks mRNA transcription
- Dose: 600 mg/day (10 mg/kg/day)
- Key features: Bactericidal AND sterilizing activity against both dividing and non-dividing organisms. Introduced in 1968 - allowed shortening of treatment from years to 6 months
- Key toxicities: Hepatotoxicity, orange discoloration of secretions/urine, drug interactions (potent CYP450 inducer - lowers levels of protease inhibitors, OCPs, warfarin, etc.)
- Resistance: rpoB mutations in 95% of cases
Pyrazinamide (PZA / Z)
- Mechanism: Active at acidic pH within macrophages → kills intracellular organisms
- Dose: 25 mg/kg/day
- Key feature: Its inclusion for 2 months allows shortening treatment from 9 to 6 months and decreases relapse rates
- Key toxicities: Hepatotoxicity, hyperuricemia/gout, arthralgia
- Avoid in liver failure and in pregnant women (US guidelines - insufficient safety data)
- Resistance: pncA gene mutations (up to 98%)
Ethambutol (EMB / E)
- Mechanism: Inhibits arabinosyltransferase (EmbB) → disrupts arabinogalactan in cell wall
- Dose: 15-20 mg/kg/day
- Key toxicity: Optic neuritis (dose-dependent) - monthly visual acuity + color vision testing
- Used in intensive phase to prevent emergence of resistance; can be stopped once drug susceptibility confirmed
- Resistance: embB gene mutations (50-65%)
- Avoid or monitor carefully in renal failure (requires level monitoring)
Part 4: Extrapulmonary TB - Duration Modifications
| Site | Standard Recommendation | Extended Duration |
|---|---|---|
| Most extrapulmonary TB (including miliary) | Standard 6-month HRZE/HR regimen | No extension needed |
| TB Meningitis | HRZE × 2 months + HR × 7-10 months (ATS/CDC/IDSA) | Total: 9-12 months |
| Bone & Joint TB | 6 months standard; some extend to 9 months | Children: up to 12 months (WHO) |
| Silicotuberculosis | Extend by at least 2 extra months | |
| Always add glucocorticoids in TB meningitis | Dexamethasone reduces mortality |
Part 5: Drug-Resistant TB
Definitions
- Isoniazid-resistant TB (Hr-TB): Resistant to INH only; rifampin susceptible
- RR-TB: Rifampin-resistant (any)
- MDR-TB: Resistant to both isoniazid AND rifampin
- Pre-XDR-TB: MDR + resistant to any fluoroquinolone
- XDR-TB: MDR + resistant to fluoroquinolone + at least one Group A drug (bedaquiline or linezolid)
Isoniazid-Resistant TB (Hr-TB)
- Fluoroquinolone must be confirmed susceptible before use
- If fluoroquinolone contraindicated: RIF + EMB + PZA × 6 months
RR-TB / MDR-TB
| Regimen | Drugs | Duration | Eligibility |
|---|---|---|---|
| BPaLM (preferred) | Bedaquiline + Pretomanid + Linezolid + Moxifloxacin | 6 months | Pre-XDR or XDR or intolerant/resistant to first-line agents |
| WHO Short-Course | Bedaquiline + fluoroquinolone + linezolid + clofazimine ± others | 9 months | No prior second-line exposure; fluoroquinolone susceptible |
| Extended regimen | Individualized based on DST | 18-20 months | Those not qualifying for short-course regimens |
Cardinal rule in failing regimens: Always add more than one drug (2-3) at a time to a failing regimen - never add a single agent (causes acquired resistance).
Part 6: TB in Special Populations
TB + HIV
- Start anti-TB treatment first, then initiate ART within 2 weeks (especially if CD4 <50/µL)
- Exception: TB Meningitis - delay ART for 8 weeks regardless of CD4 count (paradoxical IRIS risk is severe)
- Use rifampin-compatible ART: Dolutegravir (double dose) or Raltegravir + 2 NRTIs; OR Efavirenz + 2 NRTIs
- Avoid intermittent regimens in all HIV+ TB patients - daily rifampin only
- Standard 6-month daily regimen is equally effective in HIV+ and HIV- patients with drug-susceptible TB
TB in Pregnancy
- Avoid streptomycin - causes 8th cranial nerve damage in fetus (cochleotoxicity)
- Pyrazinamide - not recommended in the US (insufficient safety data); WHO recommends it
- Avoid: Thioamides (ethionamide/prothionamide), bedaquiline, delamanid in MDR-TB in pregnancy
- Breastfeeding is NOT contraindicated; drug levels in breast milk are too low to be therapeutic
TB in Renal Failure
- Never use aminoglycosides
- Ethambutol: use only if serum levels can be monitored
- INH, RIF, PZA: usual doses in mild-moderate renal failure; reduce PZA dose in severe renal failure
TB in Hepatic Disease
- Severe hepatic disease: Use EMB + streptomycin ± fluoroquinolone (avoid hepatotoxic drugs)
- Avoid PZA in liver failure
- INH and RIF may be used under close supervision if required
Part 7: TB Preventive Treatment (TPT) - Summary Table
| Regimen | Dose | Duration | Adverse Events |
|---|---|---|---|
| Isoniazid + Rifapentine (3HP) | INH 900 mg + RPT 900 mg weekly | 3 months | Systemic drug reaction, flu-like symptoms, hepatotoxicity |
| Rifampin (4R) | 600 mg/day | 4 months | Hepatotoxicity, drug interactions |
| Isoniazid + Rifampin (3HR) | INH 300 mg/d + RIF 600 mg/d | 3 months | Higher hepatotoxicity risk |
| Isoniazid (6H or 9H) | 300 mg/day or 900 mg twice weekly | 6-9 months | Hepatotoxicity (dose and duration dependent), neuropathy |
Part 8: Directly Observed Therapy (DOT)
- DOT is recommended for all intermittent regimens and for patients with:
- History of non-adherence
- Substance use disorders
- MDR/XDR-TB
- Homelessness or social instability
- Patient support and supervision are critical principles: "sound treatment = at least 2 susceptible bactericidal drugs + DOT + verification of course completion"