KTP laserin detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Searching PubMed
KTP laser otolaryngology ENT applications
Reading File
Reading File
Reading File
Searching PubMed
KTP laser laryngology voice surgery
Reading File
Finding Sources
Finding Sources
Searching PubMed
KTP laser stapedotomy otosclerosis
Reading File
Reading File
Searching PubMed
KTP laser recurrent respiratory papillomatosis treatment
Reading File
Loading Image
Reading Article
I now have sufficient content to write a comprehensive answer. Let me compile everything into a detailed 50-mark RGUHS-style response.
KTP Laser - Comprehensive Answer (50 Marks)
[RGUHS ENT Postgraduate Standard | Sources: Cummings, Scott-Brown, Shambaugh, Dhingra, Hazarika, Zakir Hussain, Stell & Maran]
1. INTRODUCTION
The Potassium Titanyl Phosphate (KTP) laser is a solid-state laser widely used in otolaryngology - head and neck surgery. It produces a visible green beam at 532 nm wavelength by a process called frequency doubling of an Nd:YAG laser. Its versatility, fiber-optic delivery, and selective absorption by hemoglobin make it one of the most useful lasers across all subspecialties of ENT.
2. LASER PHYSICS - BASIC PRINCIPLES
2.1 What is LASER?
LASER = Light Amplification by Stimulated Emission of Radiation.
Three fundamental photon-atom interactions (Figure 1):
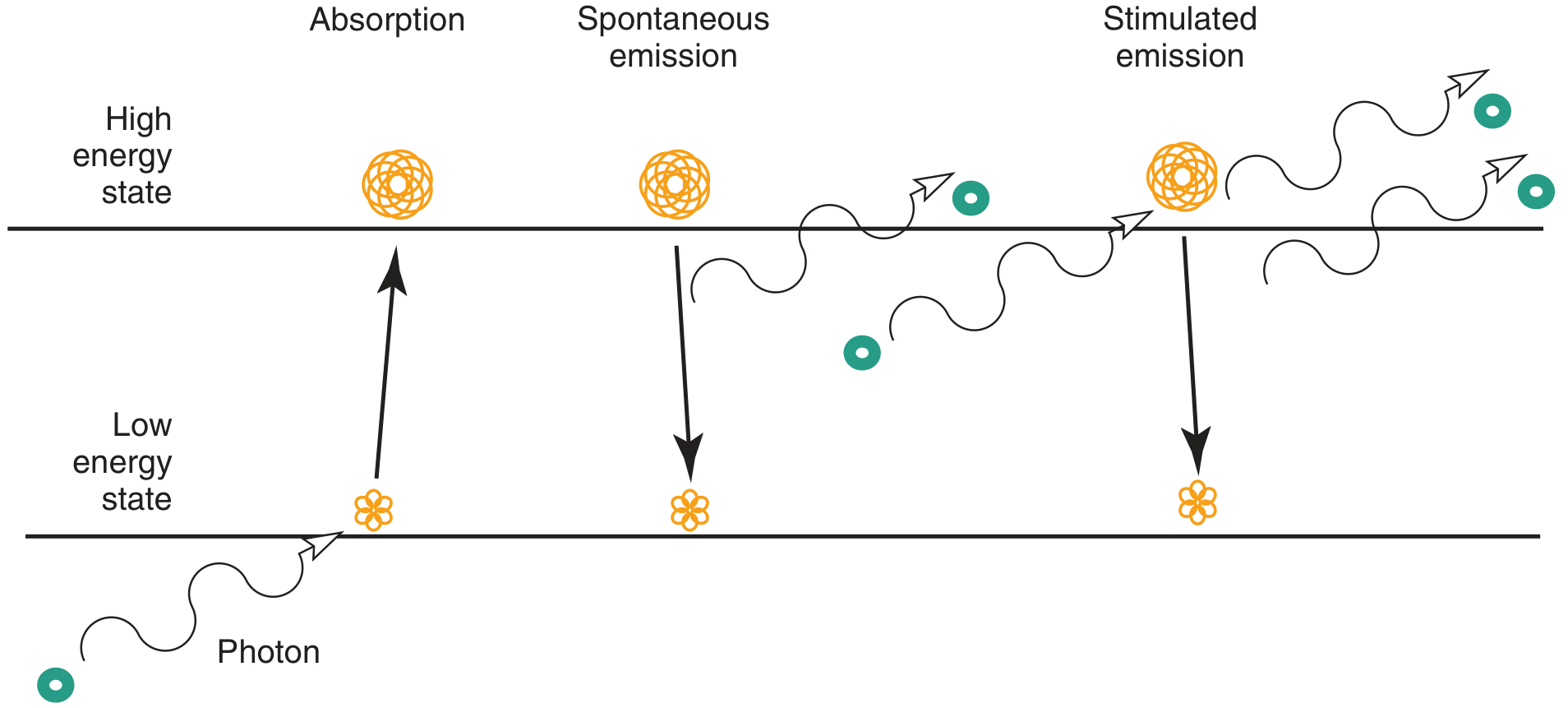
Fig. 1 - The three interactions of light with atoms: Absorption, Spontaneous Emission, and Stimulated Emission. Stimulated emission is the basis of laser action. (Cummings Otolaryngology, Fig 59.1)
2.2 Laser Generation - Flow Chart
EXTERNAL ENERGY SOURCE (electricity / flashlamp)
|
▼
ACTIVE MEDIUM (atoms raised to higher energy state)
|
▼
POPULATION INVERSION (>50% atoms in excited state)
|
▼
SPONTANEOUS EMISSION → Photons reflect off mirrors
|
▼
STIMULATED EMISSION → Pairs of identical photons produced
|
▼
OPTICAL RESONATING CAVITY (2 mirrors - 1 fully reflective,
| 1 partially transmissive)
▼
AMPLIFICATION (photons multiply with each pass)
|
▼
LASER BEAM OUTPUT (through partially transmissive mirror)
|
▼
Properties: MONOCHROMATIC + COLLIMATED + COHERENT + INTENSE
(Cummings Otolaryngology Head and Neck Surgery, Chapter 59)
2.3 Properties of Laser Light
| Property | Description |
|---|---|
| Monochromaticity | Single wavelength (pure color) |
| Coherence | Waves in spatial and temporal phase |
| Collimation | Parallel beam, minimal divergence |
| Intensity | Extremely high power density |
3. KTP LASER - SPECIFIC PHYSICS
3.1 Generation
Nd:YAG Laser (1064 nm, infrared, invisible)
|
▼
KTP Crystal (Potassium Titanyl Phosphate)
[Frequency doubling = wavelength halved]
|
▼
KTP Laser Output: 532 nm (visible GREEN light)
- The KTP crystal doubles the frequency and halves the wavelength of the parent Nd:YAG beam
- Wavelength: 532 nm (visible green spectrum)
- Because the output can be switched, one device can deliver BOTH 532 nm (KTP) and 1064 nm (Nd:YAG) light
(Cummings Otolaryngology, p. 1099)
3.2 Chromophores and Tissue Absorption
| Chromophore | Absorption at 532 nm |
|---|---|
| Oxyhemoglobin | Very high (absorption peak 542 nm - very close) |
| Melanin | High (similar to argon laser) |
| Water | Minimal |
| Collagen/connective tissue | Low |
- The KTP laser's chromophore is primarily oxyhemoglobin - this gives it excellent selective vascular photothermolysis
- Absorption by oxyhemoglobin is stronger than with the argon laser
- Scattering and absorption by skin pigments is nearly the same as with the argon laser
- Because water absorption is low, tissue penetration is deeper than the CO2 laser
(Cummings Otolaryngology, p. 1099)
3.3 Modes of Delivery
KTP Laser Delivery Systems
├── Continuous Wave (CW) Mode
│ - Standard delivery
│ - Most common clinical use
│ - Sustained thermal effect
│
└── Pulsed Mode
- Takes advantage of thermal relaxation time
- Minimizes collateral thermal damage
- Used for selective vascular effects
- Ideal for laryngeal papilloma, dysplasia
- Allows office-based procedures
- Fiber-optic delivery: light travels through a flexible optical glass fiber
- Can pass through rigid pediatric bronchoscopes as small as 3 mm
- Handheld probes available for sinus surgery, middle ear, microlaryngoscopy
(Cummings Otolaryngology, p. 1099-1100)
4. COMPARISON OF KTP WITH OTHER ENT LASERS
| Feature | CO2 | KTP (532 nm) | Nd:YAG (1064 nm) | Argon |
|---|---|---|---|---|
| Wavelength | 10,600 nm | 532 nm | 1064 nm | 488-514 nm |
| Color | Invisible (IR) | Green (visible) | Invisible (IR) | Blue-green |
| Chromophore | Water | Oxyhemoglobin | Water/pigment | Hemoglobin/melanin |
| Delivery | Mirror/arm only | Optical fiber | Optical fiber | Optical fiber |
| Penetration | Superficial | Intermediate | Deep | Intermediate |
| Hemostasis | Moderate | Excellent | Excellent | Good |
| Precision | Very high | High | Lower | High |
| Office use | Limited | Yes (pulsed) | Limited | Limited |
5. LASER-TISSUE INTERACTIONS
Temperature-Tissue Effect Flowchart
Rising Tissue Temperature → Sequential Changes:
37-60°C → DENATURATION (protein uncoiling, reversible)
↓
60-65°C → COAGULATION (protein coagulates, hemostasis)
↓
100°C → VAPORIZATION (water boils → tissue ablation/cutting)
↓
>200°C → CARBONIZATION (black eschar formation)
↓
>300°C → INCANDESCENCE (tissue glows)
- Cutting with a laser = narrow, controlled vaporization
- Lateral thermal spread → coagulation of small vessels → hemostasis
- The lateral thermal effect varies with wavelength, rate of energy application, fluence, and tissue type
(Scott-Brown's Otorhinolaryngology Vol 1, p. 631)
Controllable Parameters
- Power (Watts) - least useful variable in isolation
- Spot size (mm²) - critical; irradiance = Power/Spot Area (W/cm²)
- Exposure time (seconds)
- Irradiance (W/cm²) - the most important operating parameter at a given wavelength
6. ENT APPLICATIONS OF KTP LASER
Flow Chart of KTP Applications in ENT
KTP LASER APPLICATIONS IN ENT
│
├── OTOLOGY
│ ├── Stapedotomy (primary and revision)
│ ├── Chronic ear surgery
│ │ ├── Remove hyperplastic infected mucosa
│ │ ├── Disarticulate mobile stapes superstructure
│ │ └── Remove middle ear implants
│ └── Tympanomastoid surgery
│
├── RHINOLOGY
│ ├── FESS (functional endoscopic sinus surgery)
│ ├── Endonasal DCR (dacryocystorhinostomy)
│ ├── Turbinate reduction
│ ├── Telangiectasia destruction
│ ├── Antrostomy creation
│ ├── Nasal/sinus tumor surgery
│ └── Epistaxis control (hereditary hemorrhagic telangiectasia)
│
├── LARYNGOLOGY
│ ├── Recurrent Respiratory Papillomatosis (RRP)
│ ├── Vocal fold dysplasia / leukoplakia
│ ├── Early glottic carcinoma (T1, T2)
│ ├── Vascular polyps
│ ├── Vocal fold ectasias and varices
│ ├── Reinke's edema
│ └── Office-based laryngeal procedures (via channeled flexible scope)
│
├── TRACHEO-BRONCHIAL
│ ├── Subglottic/tracheal papilloma
│ ├── Bronchial papilloma
│ └── Endobronchial lesions (through pediatric bronchoscope ≥ 3mm)
│
└── OROPHARYNX / HEAD AND NECK
├── Tonsillectomy
└── Pigmented dermal lesions
(Cummings, p. 1099; Scott-Brown Vol 1, p. 631; Scott-Brown Vol 2, p. 3107)
7. OTOLOGICAL APPLICATIONS IN DETAIL
7.1 KTP Laser Stapedotomy
Indications: Otosclerosis (primary and revision stapedectomy)
Advantages of Laser Stapedotomy over Mechanical Methods:
- Stabilization of the prosthesis in the center of the oval window
- Reduced trauma to the inner ear (less postoperative sensorineural loss and dizziness)
- Less mechanical trauma to the middle ear (reduced adhesions, less risk to facial nerve)
- No footplate mobilization or fracture (unlike trocar or microdrill)
KTP Technique:
- The 200-μm EndoOtoprobe is the most popular delivery system
- Rosette technique: A series of tiny rosettes (0.05-0.2 mm) are vaporized in the center of the stapes footplate
- Result is an irregular, scalloped stapedotomy - precise diameter control is difficult
- Surgeons usually seal the visible laser stapedotomy with a vein or perichondrium graft
Limitations (Shambaugh):
- A KTP 200-μ fiber did not deliver adequate energy for some applications
- Visible lasers (KTP, argon) produce irregular scalloped stapedotomies - harder to achieve the precise 0.6 mm round hole preferred by many surgeons
- CO2 laser is preferred by some experts (Shambaugh) for a precisely round, sized stapedotomy that minimizes collagen contracture and prosthesis migration
Safe Energy Parameters: Established by laboratory thermocouple experiments for argon, KTP, CO2, and erbium:YAG lasers.
(Shambaugh Surgery of the Ear; Cummings, p. 1099)
7.2 Chronic Ear Surgery (Thedinger)
Thedinger specifically promoted KTP laser for:
- Removing hyperplastic infected mucosa in cholesteatoma surgery
- Disarticulating mobile stapes superstructure for complete cholesteatoma removal
- Removing previously inserted middle ear implants
8. LARYNGOLOGICAL APPLICATIONS IN DETAIL
8.1 Recurrent Respiratory Papillomatosis (RRP)
KTP vs. CO2 Laser in RRP (Scott-Brown Vol 2):
CO2 Laser (Traditional) KTP / Nd:YAG Laser
───────────────────────────── ──────────────────────────────────
- Easy with microscope & - Equally effective for ablation
micromanipulator and haemostasis
- Minimal bleeding - FIBER DELIVERY → can treat
- Treatment of choice for many TRACHEAL and BRONCHIAL papillomas
- Late soft-tissue complications:- Can be delivered through flexible
fibrosis, webbing, stenosis bronchoscope for adult patients
(13-45% rate) - Fiber guidance system with bendable
distal tip: 50° directional range
- Plume extractor mandatory (infectious viral load in laser plume)
- KTP plays a key role in subglottic and infraglottic disease inaccessible to CO2
8.2 Office-Based KTP Laser Laryngology (Pulsed Mode)
IN-OFFICE KTP PROCEDURE FLOW:
Patient awake (topical anesthesia)
↓
Flexible channeled laryngoscope introduced transnasally
↓
KTP laser fiber passed through working channel
↓
Pulsed KTP delivered to target (papilloma, polyp, dysplasia, varix)
↓
Selective vascular photothermolysis → lesion ablation
↓
No general anesthesia required
Advantages:
- Office-based (no GA required)
- Selective for vascular lesions
- Minimal thermal spread in pulsed mode
- Avoids microlaryngoscopy risks in frail patients
- Ideal for performers/professional voice users
Indications for Office KTP:
- RRP (adult, accessible lesions)
- Vocal fold dysplasia/leukoplakia
- Vascular polyps, ectasias, varices
- Reinke's edema debulking
- Early glottic lesions
(Cummings, p. 1099-1100)
8.3 KTP Laser for Glottic Neoplasms
Recent Evidence (Suppah et al., 2023 - Meta-Analysis, Laryngoscope):
- 8 studies included; mean follow-up 3.3 years
- Overall survival: 90.7% (95% CI 85%-96.5%)
- Disease-free survival: 98.5% (95% CI 97.3%-99.8%)
- Pooled recurrence: 7.7% (95% CI 3.4%-12%)
- Voice Handicap Index (VHI) at 6 months: 6.76; at 1 year: 5.21
- Conclusion: KTP laser ablation is safe and effective for early glottic neoplasms with excellent oncological and voice outcomes [PMID: 36606671]
9. RHINOLOGICAL APPLICATIONS
9.1 Endonasal DCR (Dacryocystorhinostomy)
- KTP laser creates the rhinostomy through a fiber passed endonasally
- Comparable to Holmium:YAG for this application
- Avoids external scar
9.2 Turbinate Reduction and FESS
- Handheld fiber probes used intranasally
- Reduces inferior turbinate bulk with good hemostasis
- Can treat nasal telangiectasias in Hereditary Hemorrhagic Telangiectasia (HHT/Osler-Weber-Rendu)
10. LASER SAFETY
Safety Protocol Flowchart
LASER SAFETY MEASURES
│
├── PATIENT SAFETY
│ ├── Wet gauze/fire-proof material shield
│ ├── Laser-safe endotracheal tube (airway fire prevention)
│ └── Wet cottonoids around target area
│
├── STAFF SAFETY
│ ├── Appropriate wavelength-specific eye protection
│ │ (KTP 532 nm → optical density ≥ 4 green-filter goggles)
│ ├── Plume extractor / smoke evacuator
│ └── Mandatory training + signed documentation
│
├── ENVIRONMENTAL SAFETY
│ ├── Warning sign + locked operating room doors
│ ├── Laser-protected windows/walls
│ └── Blackened endoscopic instruments (reduce reflections)
│
└── EQUIPMENT SAFETY
├── Key to laser held by senior surgeon only
├── Laser in STANDBY mode when not actively firing
└── Regular equipment checks per Medical Devices Agency guidelines
(Scott-Brown Vol 1, p. 631-632)
Eye Protection for KTP (532 nm):
- All personnel must wear green-wavelength-blocking goggles
- The patient's cornea and retina are at high risk as 532 nm is a visible wavelength that can be focused by the lens onto the retina
11. COMPLICATIONS OF KTP LASER
General Complications
KTP LASER COMPLICATIONS
│
├── THERMAL INJURY
│ ├── Even pulsed mode can cause deeper damage
│ │ (computer modeling shows inadequate cooling between pulses)
│ └── Adjacent tissue necrosis
│
├── OTOLOGICAL
│ ├── Postoperative sensorineural hearing loss
│ ├── Vestibular disturbance / dizziness (high fluence)
│ └── Facial nerve injury (rare)
│
├── LARYNGOLOGICAL
│ ├── Airway fire (with unprotected tube)
│ ├── Posterior glottic/subglottic stenosis
│ ├── Scarring / fibrosis
│ └── Incomplete ablation → recurrence
│
├── RHINOLOGICAL
│ ├── Crusting and adhesions
│ └── Septal perforation (rare)
│
└── SYSTEMIC / OCCUPATIONAL
├── Laser plume inhalation (viral load in RRP)
└── Retinal injury (eye protection breach)
Recent evidence (Mizoguchi et al., 2024) showed that high fluence in laser stapedotomy aggravates transient subjective dizziness - emphasizing the importance of using established safe energy parameters [PMID: 38546378].
12. ADVANTAGES AND DISADVANTAGES
Advantages of KTP Laser
- Fiber-optic delivery - flexible fiber enables access to difficult anatomical sites (trachea, bronchi, pediatric airways, office laryngoscopy)
- Selective vascular absorption - ideal for vascular lesions (papilloma, polyps, ectasias, varices, telangiectasias)
- Excellent hemostasis - stronger oxyhemoglobin absorption than argon
- Dual-mode operation - CW for ablation; pulsed for selective photothermolysis
- Switchable with Nd:YAG - same device can deliver both wavelengths
- Office use possible - pulsed KTP through channeled flexible scope avoids general anesthesia
- Visible beam - no separate aiming beam needed (unlike CO2 or Nd:YAG)
- Versatility - applicable in otology, rhinology, laryngology, head and neck
Disadvantages
- Irregular stapedotomy - rosette technique gives scalloped edges, less precise than CO2 for exact fenestration sizing
- Deeper penetration than CO2 - greater risk of thermal damage to inner ear structures
- Pulsed mode inadequate cooling - computer modeling shows potential for deeper damage between pulses
- Less precise than CO2 for microlaryngeal cutting
- Eye hazard - visible green beam at 532 nm is particularly dangerous (direct retinal absorption)
- Cost - expensive equipment
13. RECENT ADVANCES (RGUHS Perspective)
13.1 Office-Based KTP Laser Surgery
The major advance in the past decade is the shift toward awake, office-based procedures using pulsed KTP through channeled flexible laryngoscopes. This has transformed the management of:
- Benign vocal fold lesions (ectasias, varices, polyps)
- RRP in adult patients
- Vocal fold dysplasia/leukoplakia
A 2024 systematic review (Bhat et al.) demonstrated that photoangiolytic lasers (KTP and PDL) are effective for benign laryngeal lesions with good voice outcomes [PMID: 39119758].
13.2 KTP in Professional Voice Users
O'Connor et al. (2025) assessed KTP laser ablation of benign vocal fold lesions specifically in performers, showing favorable outcomes with voice preservation - relevant for professional voice users and singers [PMID: 40204606].
13.3 KTP for Vocal Fold Dysplasia and Leukoplakia
The 2026 review by Miri et al. on office-based surgery for dysplasia and leukoplakia confirmed KTP as an effective modality in this setting [PMID: 40835561].
13.4 KTP in RRP - Office Setting
The 2026 systematic review by Miri et al. (Otolaryngol Head Neck Surg, 2026) supports office-based RRP surgery as effective and safe, with KTP being the primary modality [PMID: 41848235].
13.5 Technological Advances
- Pulsed KTP systems with computer-controlled pulse parameters
- Distal-tip articulating fiber delivery systems
- Integration with office-based laryngoscopy platforms
- 532 nm diode laser systems that mimic KTP without requiring Nd:YAG source
14. SUMMARY TABLE - KTP LASER AT A GLANCE
| Parameter | Details |
|---|---|
| Full name | Potassium Titanyl Phosphate laser |
| Wavelength | 532 nm |
| Color | Visible green |
| Parent laser | Nd:YAG (1064 nm) |
| Generation mechanism | Frequency doubling through KTP crystal |
| Primary chromophore | Oxyhemoglobin (peak 542 nm) |
| Secondary chromophore | Melanin |
| Delivery | Fiber-optic (flexible) |
| Modes | Continuous wave + Pulsed |
| Key ENT applications | Stapedotomy, RRP, glottic tumors, turbinates, DCR |
| Distinguishing feature | Office-based pulsed delivery; vascular selectivity |
| Eye protection | Green-blocking goggles (OD ≥ 4) |
15. MNEMONICS FOR RGUHS EXAMS
KTP = Kills Tumors Photoangiolytically (vascular selectivity)
LASER properties = MICC - Monochromatic, Intense, Collimated, Coherent
KTP Applications = SLOT - Stapedotomy, Larynx (RRP, dysplasia), Optics (DCR), Turbinate/sinus
16. REFERENCES / SOURCE TEXTBOOKS
- Cummings Otolaryngology Head and Neck Surgery (7th Ed.) - Chapter 59: Lasers in Otolaryngology - detailed laser physics, KTP specific section p. 1099-1100
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 1 - Laser applications chapter, p. 631-632
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 2 - KTP in RRP management, p. 3107-3114
- Shambaugh Surgery of the Ear - Laser stapedotomy, thermocouple experiments, safety parameters, p. 5878-6141
- Dhingra - Diseases of ENT (for laser classification and basic applications)
- Hazarika - Textbook of ENT and Head-Neck Surgery (for Indian standard of ENT laser practice)
- Zakir Hussain - Synopsis of Diseases of ENT (for exam-oriented laser summary)
- Stell and Maran's Head and Neck Surgery (for head and neck laser oncology context)
Recent Literature:
- Suppah M et al. "Outcomes of KTP Laser Ablation in Glottic Neoplasms: A Systematic Review and Meta-Analysis." Laryngoscope 2023;133:1806-1814 [PMID: 36606671] - View on PubMed
- Bhat AM et al. "Photoangiolytic Lasers for Treatment of Benign Laryngeal Lesions: A Systematic Review and Meta-Analysis." Laryngoscope 2024 Dec [PMID: 39119758] - View on PubMed
- Miri M et al. "Surgical and Voice Outcomes of Office-Based RRP Surgery: A Systematic Review." Otolaryngol Head Neck Surg 2026 Jun [PMID: 41848235]
- Mizoguchi Y et al. "High fluence in laser stapedotomy aggravates transient subjective dizziness." Acta Otolaryngol 2024 [PMID: 38546378]
APPENDIX: KEY DIAGRAMS SUMMARY
Diagram 1 (already shown above) - Laser physics: Absorption, Spontaneous Emission, Stimulated Emission (Cummings Fig. 59.1)
Diagram 2 - KTP Crystal frequency-doubling:
[Nd:YAG source] → 1064 nm ──→ [KTP Crystal] ──→ 532 nm output
infrared visible green
Diagram 3 - Absorption spectrum showing KTP (532 nm) sits near the oxyhemoglobin absorption peak at 542 nm, explaining its excellent vascular selectivity.
Diagram 4 - Temperature-Tissue Effect curve (described in Section 5 above).
Diagram 5 - Stapedotomy rosette technique: series of overlapping 0.05-0.2 mm spots in stapes footplate center creating the fenestration.
Examiner's Note for RGUHS 50-mark answer: A complete answer should cover physics (10 marks), generation/properties of KTP specifically (8 marks), laser-tissue interactions (7 marks), ENT applications with details (15 marks), safety (5 marks), complications (3 marks), and recent advances (2 marks). This answer addresses all these domains comprehensively.
This is a shared conversation. Sign in to Orris to start your own chat.