Sequestrum mbbs university style
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
I now have all the content and images needed for a comprehensive MBBS-style answer. Here it is:
SEQUESTRUM - MBBS University Notes
Definition
A sequestrum is a fragment of dead (necrotic) bone that has become separated from the surrounding viable bone and lies free within a cavity or a bed of granulation tissue, typically as a complication of chronic osteomyelitis.
The term comes from the Latin sequestrare - to separate or set apart.
Context: Chronic Osteomyelitis
Sequestrum formation is the hallmark of chronic osteomyelitis, which is the aftermath of inadequately treated acute osteomyelitis.
"A piece of bone becomes dead (Sequestrum) and remains within the cavity which is formed by destruction of the bone due to the infection. This cavity is generally connected outside through a sinus."
- S Das, A Manual on Clinical Surgery
Pathogenesis / How a Sequestrum Forms
The sequence of events (important for exam):
- Bacterial infection reaches bone (most commonly via haematogenous spread - Staphylococcus aureus is the #1 organism)
- Bacteria proliferate → neutrophilic inflammatory reaction → bone cell necrosis within 48 hours
- Inflammation spreads through Haversian systems to the periosteum
- Periosteum lifts (especially in children, where it is loosely attached) → subperiosteal abscess forms
- Lifting of periosteum further compromises blood supply → extends necrosis
- After 1 week: chronic inflammatory cells release cytokines → osteoclastic bone resorption + fibrous tissue ingrowth
- The dead avascular fragment = Sequestrum
- Surrounding reactive new bone deposition = Involucrum (shell of living bone encasing the dead fragment)
- Apertures in the involucrum = Cloaca (plural: cloacae) - channels through which pus and sequestrum fragments may discharge to the surface via a sinus tract
(Robbins & Kumar Basic Pathology)
The Classic Triad of Chronic Osteomyelitis
| Structure | What it is | Appearance |
|---|---|---|
| Sequestrum | Dead necrotic bone fragment | Dense, ivory-white; avascular; no osteocytes on histology |
| Involucrum | Periosteal shell of new reactive bone surrounding sequestrum | Thickened, sclerotic new bone |
| Cloaca | Aperture/opening in the involucrum | Drainage channel; visible on CT/MRI |
Gross Pathology Image (Robbins)
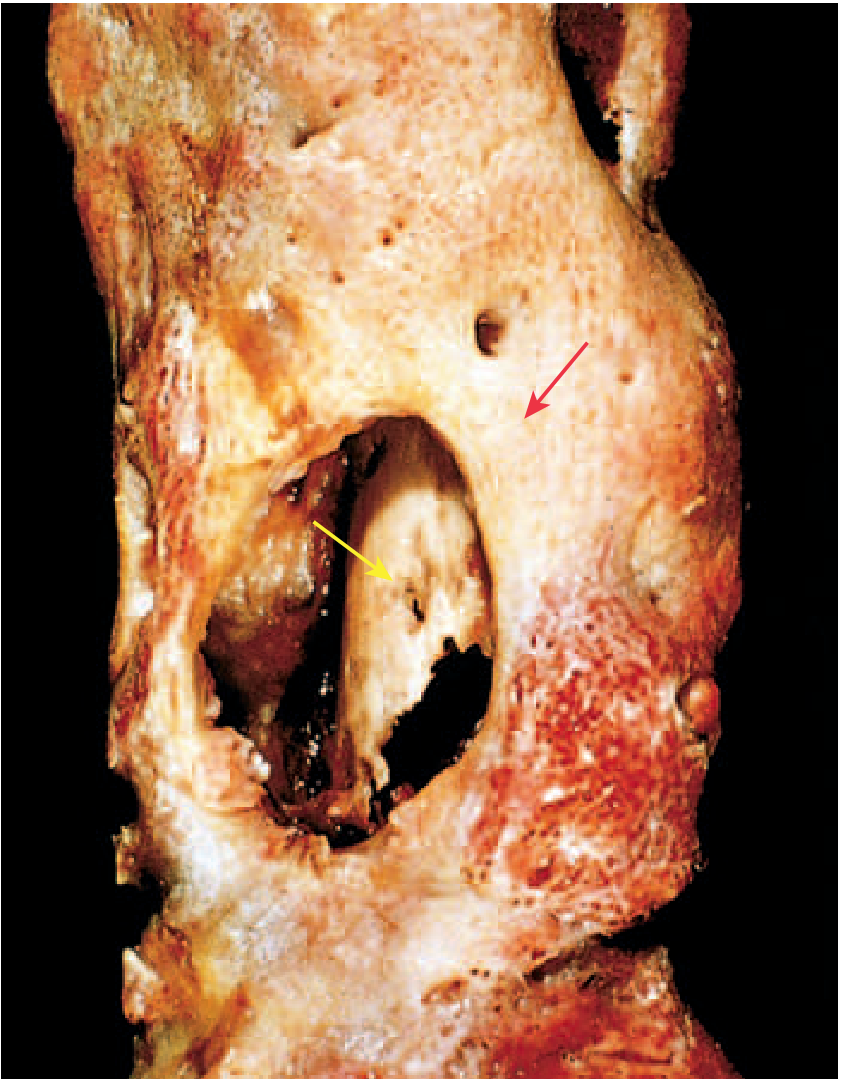
FIG. 19.13 Resected femur in a patient with draining osteomyelitis. The drainage tract is within the subperiosteal shell of viable new bone (involucrum, yellow arrow). The original cortex (sequestrum, red arrow) is necrotic.
- Robbins & Kumar Basic Pathology
Histology of Sequestrum
- Empty lacunae (dead osteocytes - the most reliable microscopic marker)
- No viable osteocytes
- Surrounded by purulent exudate and granulation tissue
- No vascular channels within the fragment
- Background: marrow fibrosis, lymphocytes, plasma cells (chronic inflammatory infiltrate)
Clinical Features of Chronic Osteomyelitis (with Sequestrum)
- Long history of discharging sinus from a previous acute osteomyelitis episode
- Sinus opening shows sprouting granulation tissue (key clinical sign - indicates sequestrum in depth)
- Thickened, irregular bone on palpation
- Low-grade fever, malaise
- Serous/purulent discharge from sinus
- Sinus may temporarily close then re-open (characteristic recurrent pattern)
Radiological Features
X-ray (Plain Radiograph)
- Areas of bony rarefaction (destruction) surrounded by dense sclerosis
- The sequestrum appears as a dense, isolated fragment of bone (denser than surrounding bone because it has no blood supply and does not undergo osteoporosis)
- Involucrum seen as periosteal new bone formation
- Useful only in chronic cases - practically valueless in early acute osteomyelitis
CT Scan
CT is the investigation of choice for chronic osteomyelitis:
- Best demonstrates intraosseous cavities containing the sequestrum
- Shows cloaca (apertures) in the involucrum
- Guides surgical planning

Fig. 46.10 Chronic Osteomyelitis with Sequestrum. Axial CT of the tibia: cloaca in the posterior cortex (black arrows), small sequestrum within it (white arrow).
- Grainger & Allison's Diagnostic Radiology
MRI
- Sequestrum has similar signal to the bone it came from (low T1 and T2 if cortical; higher signal if from cancellous bone)
- The involucrum shows enhancement with gadolinium but the sequestrum itself does NOT enhance (avascular - no contrast uptake - this is pathognomonic)
- Cloaca = high signal defect in cortical bone on fluid-sensitive sequences
Types / Special Forms
| Type | Key Features |
|---|---|
| Acute Osteomyelitis | No sequestrum yet; haematogenous; children; metaphysis of long bones; S. aureus |
| Chronic Osteomyelitis | Sequestrum + involucrum + cloaca + sinus; gram-negative organisms may be involved |
| Brodie's Abscess | Subacute localized form; metaphysis; sclerotic rim on X-ray; low-virulence Staph; no obvious sequestrum; "penumbra sign" on MRI |
| Tuberculous | Rarefaction predominates; minimal sclerosis; cold abscess; sinus with undermined edges; sequestrum less common |
Treatment
Conservative:
- Prolonged antibiotics (targeted to culture - S. aureus most common)
- In chronic osteomyelitis with gram-negative organisms, surgical removal of sequestrum is recommended in addition to antibiotics
Surgical (Sequestrectomy + Saucerization):
- Sequestrectomy = surgical removal of the sequestrum
- Saucerization (Saucerisation) = conversion of the infected cavity into a shallow saucer by removing overhanging bone edges - allows drainage and healing
- Timing: wait until the involucrum is fully formed before removing sequestrum (otherwise structural support is lost)
- Combined with wound debridement, dead space management, and appropriate antibiotics
Complications of Chronic Osteomyelitis
- Pathological fracture (bone weakened by cavity)
- Secondary (reactive) amyloidosis - due to prolonged suppuration (amyloid in kidneys → albuminuria)
- Septic arthritis - if metaphysis is intra-articular
- Squamous cell carcinoma in a long-standing sinus tract (Marjolin's ulcer equivalent)
- Sarcoma in the infected bone
- Endocarditis and sepsis
- Deformity - limb shortening or lengthening (epiphyseal growth plate involvement)
High-Yield One-Liners for MCQs
- Sequestrum = dead bone | Involucrum = new bone | Cloaca = opening in involucrum
- Sequestrum does not enhance on gadolinium MRI (avascular)
- CT is best for demonstrating sequestrum in chronic osteomyelitis
- MRI is best for early acute osteomyelitis (positive at 3-5 days)
- Most common organism = S. aureus (except sickle cell = Salmonella)
- Granulation tissue at sinus opening = sequestrum in depth
- Sequestrum appears denser than surrounding bone on X-ray (no hyperaemia/osteoporosis)
- Treat by sequestrectomy - but only after involucrum is fully formed
Sources: Robbins & Kumar Basic Pathology | S Das: A Manual on Clinical Surgery, 13th Ed | Grainger & Allison's Diagnostic Radiology | Campbell's Operative Orthopaedics 15th Ed (2026) | Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.