Chicken pox lesion description
Reading File
Finding Sources
Searching Images
chickenpox varicella skin lesion rash
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Here is a comprehensive description of chickenpox (varicella) lesions:
Chickenpox (Varicella) — Lesion Description
Causative Agent
Varicella-zoster virus (VZV), a member of the herpesvirus family. The rash results from viremic spread to the skin during primary infection.
Distribution
- Begins on the face and scalp, then spreads rapidly to the trunk (centripetal distribution)
- Relative sparing of the extremities
- Denser on the back between the shoulder blades; more profuse on medial limb aspects
- Mucous membranes are also involved — mouth, nose, pharynx, vagina (vesicles rupture quickly, leaving shallow 2–3 mm ulcers)
- Lesions appear in successive crops over several days
Sequential Morphological Stages
Each lesion progresses rapidly — often within as little as 12 hours:
| Stage | Description |
|---|---|
| Macule | Rose-colored flat spot |
| Papule | Raised, erythematous bump |
| Vesicle | 2–3 mm, thin-walled, elliptical; long axis parallel to skin folds; surrounded by irregular erythema — classic "dewdrop on a rose petal" appearance |
| Pustule | Vesicle fills with inflammatory cells → becomes cloudy; center dries first → umbilicated pustule |
| Crust | Dries and crusts over; falls off in 1–3 weeks |
The hallmark diagnostic feature: all stages present simultaneously in any one area of skin ("pleomorphic" or "crops at different stages"). This distinguishes varicella from smallpox, where all lesions are at the same stage.
Key Vesicle Characteristics
- Size: 2–3 mm in diameter
- Shape: Elliptical, with long axis parallel to skin fold lines
- Wall: Superficial and thin-walled
- Surrounding halo: Irregular zone of erythema — gives the "dewdrop on a rose petal" appearance
- Evolution: Vesicle → cloudy pustule (influx of inflammatory cells) → umbilicated → crust
- Average count: 250–500 lesions in healthy children; more numerous in adults and immunocompromised
Healing & Scarring
- Crusts fall off spontaneously in 1–3 weeks, leaving shallow pink depressions that fade
- Scarring is rare unless lesions are scratched or superinfected
- May leave hypopigmented macules persisting weeks to months
- If scars occur, they are depressed and poxlike
In Immunocompromised Patients
- Lesions may lack surrounding erythema
- Vesicles may not progress to pustules
- Larger vesicles that may fuse (as seen in panel F below)
- Higher risk of disseminated/hemorrhagic varicella
Clinical Images
Fitzpatrick's Dermatology — Figure 165-2: Stages of varicella lesions
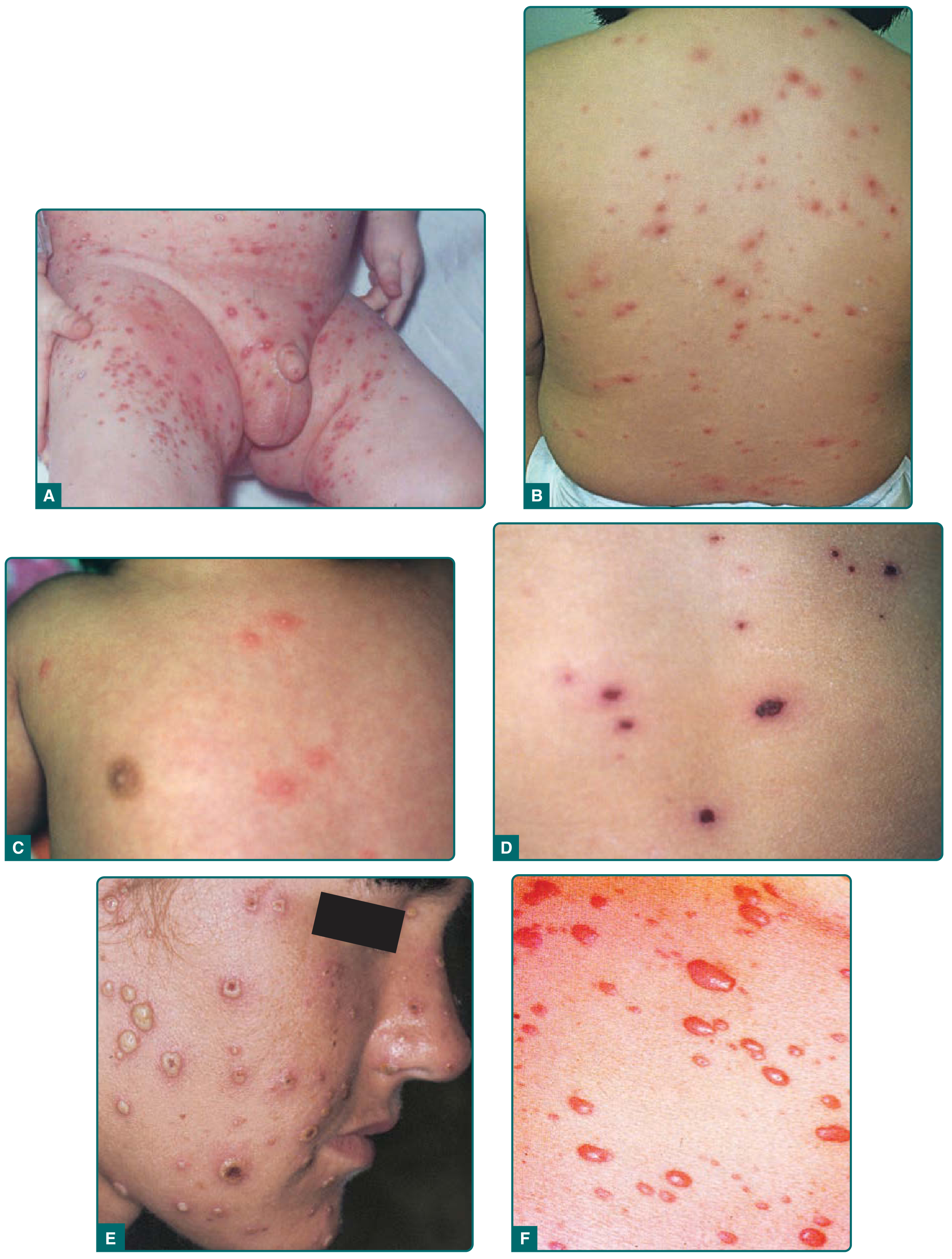
DermNet — Vesiculopapular eruption on the trunk:

Associated Symptoms
- Pruritus — the most distressing symptom, present until all lesions crust
- Fever — proportional to rash severity; persists while new lesions appear (up to 40.5°C in severe cases)
- Prodrome in older children/adults: 2–3 days of fever, malaise, headache, anorexia, backache
Sources: Fitzpatrick's Dermatology, 8th Ed., pp. 3069–3070; Goldman-Cecil Medicine, 26th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.