Multiple sclerosis for nurses
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive material. Let me compile the full nursing-oriented guide on Multiple Sclerosis.
Multiple Sclerosis — A Nursing Guide
Overview
Multiple sclerosis (MS) is a chronic, immune-mediated, demyelinating disease of the central nervous system (CNS) characterized by neurological deficits disseminated in time and space. It is a leading cause of disability in young adults in North America. Women are affected roughly twice as often as men (2:1 ratio), and onset typically occurs in the early 20s for relapsing disease and mid-30s for progressive disease.
Pathophysiology
MS involves autoimmune attack on myelin sheaths and oligodendrocytes. T lymphocytes cross the blood-brain barrier, triggering inflammation, demyelination, axonal injury, and eventually axonal loss. This disrupts nerve conduction velocity and synaptic transmission, producing the varied neurological deficits seen clinically.
Key genetic risk factor: HLA-DR2 (DR1501) haplotype. First-degree relatives carry a 2–5% lifetime risk versus <0.1% in the general population.
Environmental factors include: vitamin D deficiency, Epstein-Barr virus (EBV) exposure, smoking, and geographic latitude (higher prevalence in northern latitudes).
Disease Subtypes
| Type | Description |
|---|---|
| Relapsing-Remitting (RR) | Most common (~65%). Discrete attacks followed by full or partial recovery. |
| Secondary Progressive (SP) | Gradual neurological worsening after an initial RR course; most RR patients convert within 15–20 years. |
| Primary Progressive (PP) | Steady worsening from onset without relapses (~15%). More common in men, older onset. |
| Progressive-Relapsing (PR) | Progressive from onset with superimposed relapses. |
— Bradley and Daroff's Neurology in Clinical Practice
Clinical Presentation
MS can affect virtually any part of the CNS. Common presenting features include:
Visual Symptoms
- Optic neuritis: painful unilateral vision loss; retrobulbar inflammation means "the patient sees nothing and the doctor sees nothing" — but a relative afferent pupillary defect (Marcus-Gunn pupil) is detectable on swinging flashlight test.
- Internuclear ophthalmoplegia (INO): slowed adduction of one eye + contralateral abducting nystagmus — highly suggestive of MS.
- Diplopia, oscillopsia, blurred vision.
Motor Symptoms
- Weakness and impaired coordination, typically beginning in a leg, ascending from distal to proximal.
- Spasticity, hyperreflexia, extensor plantar responses.
Sensory Symptoms
- Paresthesias, numbness, tingling.
- Lhermitte sign: brief electric shock sensation down the spine on neck flexion — characteristic of cervical cord disease.
Cerebellar Symptoms
- Ataxia, intention tremor, dysmetria, dysarthria (Charcot's triad: nystagmus + intention tremor + scanning speech).
Uhthoff Phenomenon
- Transient worsening of symptoms with heat (e.g., hot shower, fever, exercise). Important: this is NOT a new relapse — reversible with cooling.
Cognitive & Psychiatric
- Depression affects the majority of MS patients.
- Cognitive impairment (especially attention, processing speed, memory).
- Pseudobulbar affect (pathological laughing/crying).
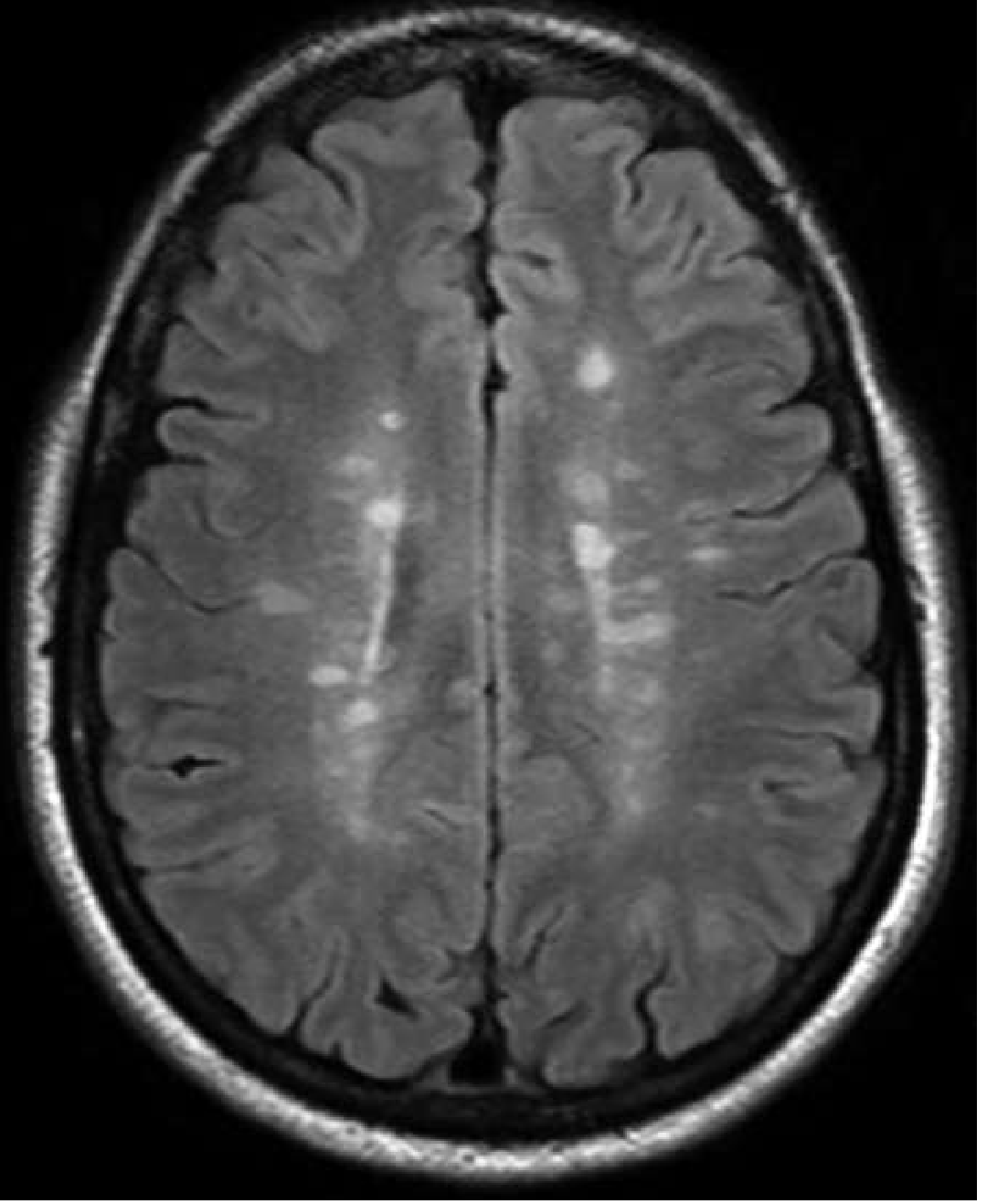
MRI Findings
MRI is the cornerstone of MS diagnosis. Classic findings:
Axial FLAIR MRI — periventricular and deep white matter hyperintense lesions:
Sagittal FLAIR MRI — "Dawson's fingers" radiating perpendicularly from ventricles:
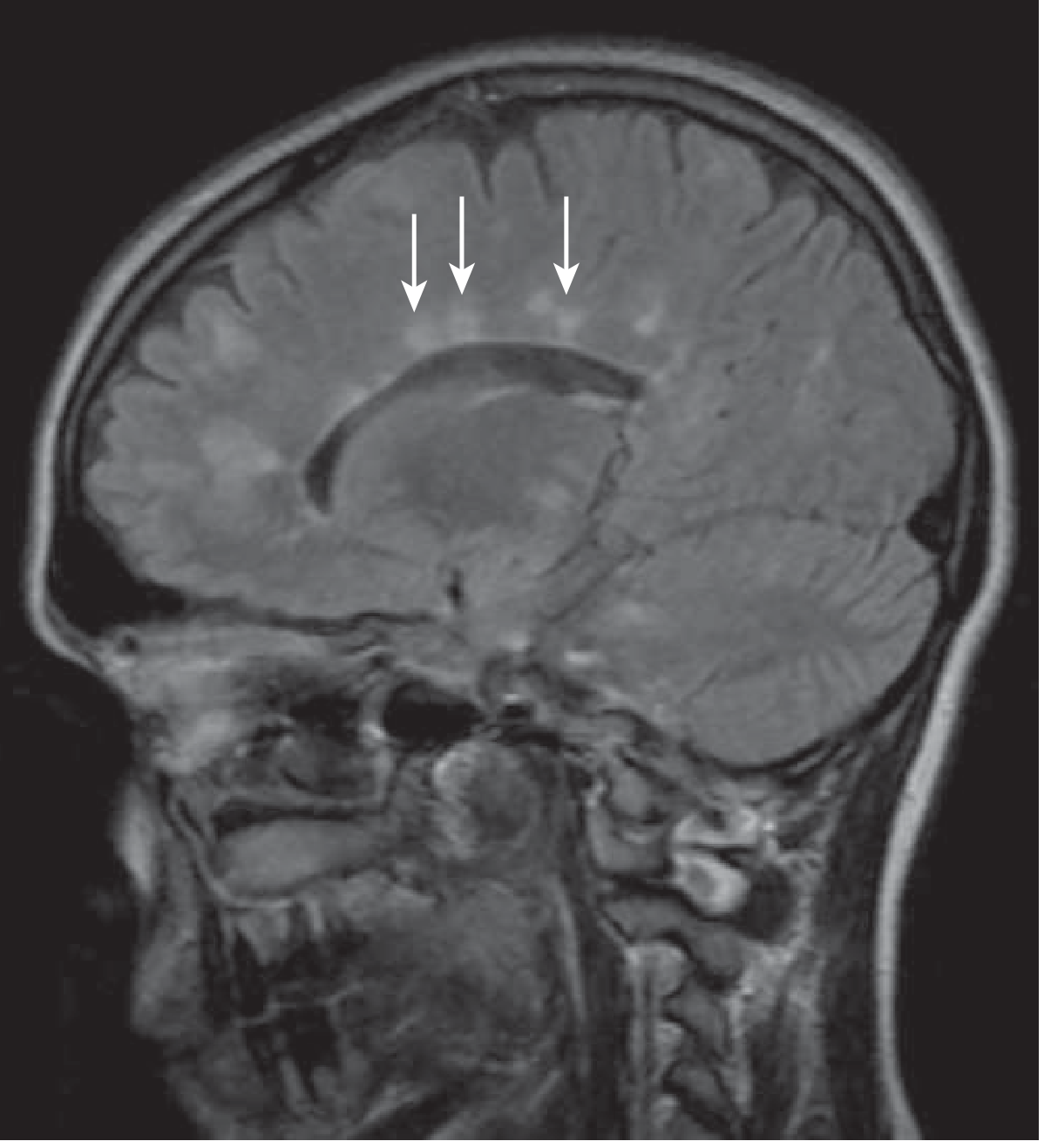
Lesion locations: periventricular, juxtacortical, infratentorial (brainstem/cerebellum), and dorsolateral spinal cord.
- Gadolinium enhancement = active inflammation (persists 2–8 weeks)
- T1 black holes = axonal loss and atrophy (poor prognosis)
— Goldman-Cecil Medicine, International Edition
Diagnosis: McDonald Criteria (2017)
Requires demonstration of dissemination in space (DIS) and dissemination in time (DIT):
- DIS: lesions in ≥2 characteristic locations (periventricular, juxtacortical, infratentorial, spinal cord)
- DIT: new T2/gadolinium lesions on follow-up MRI, or simultaneous presence of enhancing and non-enhancing lesions
For Primary Progressive MS: ≥1 year of disability progression + 2 of: ≥1 T2-hyperintense brain lesion, ≥2 spinal cord T2 lesions, CSF oligoclonal bands.
CSF findings: oligoclonal IgG bands (sensitivity ~85%), elevated IgG index — evidence of intrathecal immunoglobulin production. Note: not specific to MS.
Key Nursing Assessments
Nurses should perform and document:
- Neurological status: strength, coordination, gait, balance (fall risk)
- Visual: visual acuity, diplopia, pupillary responses
- Fatigue level: fatigue affects up to 78% of MS patients — use a validated fatigue scale
- Bladder function: voiding frequency, urgency, retention, incontinence, UTI history
- Bowel function: constipation or incontinence
- Mood: depression and anxiety screening (PHQ-9)
- Cognitive function: attention, memory, processing speed
- Pain: type (neuropathic vs. musculoskeletal vs. spastic), location, severity
- Temperature sensitivity: history of Uhthoff phenomenon
- Skin integrity: pressure injury risk in those with reduced mobility
- Medication adherence and injection-site reactions (for patients on self-injectable DMTs)
- Social support, caregiver burden
Symptom Management
Fatigue (up to 78% of patients)
- First-line: evaluate and treat contributing factors (insomnia, depression, nocturia, pain, spasticity).
- Pharmacological: amantadine 100 mg BID (40% efficacy, well tolerated), modafinil (evidence mixed), methylphenidate.
- Non-pharmacological: energy conservation strategies, occupational therapy, exercise pacing.
Spasticity
- Baclofen (5–160 mg/day in divided doses) — never stop abruptly (risk of severe withdrawal reaction including seizures and hyperthermia).
- Tizanidine (2–32 mg/day); start low at bedtime.
- Physical therapy, stretching, hydrotherapy.
- Intrathecal baclofen pump for severe refractory spasticity.
- Note: reducing tone can unmask underlying weakness.
Bladder Dysfunction (affects 50–80% of patients)
Two distinct types require different management:
| Type | Symptoms | Management |
|---|---|---|
| Hyperreflexic/overactive | Urgency, frequency, urge incontinence | Anticholinergics: oxybutynin (2.5–5 mg TID), tolterodine, darifenacin; β3 agonist mirabegron; botulinum toxin injection |
| Hypotonic/underactive | Hesitancy, retention, overflow incontinence | Bethanechol; intermittent self-catheterization; α-blocker (tamsulosin) for outlet obstruction |
Nursing key: Check post-void residual volume (>50 mL abnormal; >300 mL requires intervention). Recurrent UTIs are a red flag requiring urological referral.
Bladder/Bowel Nursing Interventions
- Timed voiding schedules
- Fluid management (adequate hydration — avoid restriction)
- Bowel program: fibre, adequate fluids, scheduled toileting, stool softeners
Gait and Mobility
- Dalfampridine (Ampyra) — potassium channel blocker; improves walking speed in ~35% of patients. Contraindicated if seizure history.
- Physiotherapy and occupational therapy for compensatory strategies, assistive devices, fall prevention.
Pain
- Neuropathic pain: gabapentin, pregabalin, TCAs (amitriptyline, nortriptyline).
- Trigeminal neuralgia: carbamazepine first-line.
- Lhermitte sign: usually self-limiting; cervical collar may help.
Depression
- Antidepressants: SSRIs/SNRIs — fluoxetine, sertraline, venlafaxine, bupropion (preferred for their "activating" properties in fatigued patients).
- Sedating agents (amitriptyline, nortriptyline, trazodone) useful when pain or insomnia coexists.
- Cognitive-behavioural therapy (CBT) and mindfulness have evidence in MS.
Cognitive Impairment
- Cognitive rehabilitation, compensatory strategies, memory aids.
- Treat underlying depression, fatigue, and sleep disorders.
Sexual Dysfunction (affects 45–74% of women, common in men)
- Erectile dysfunction: phosphodiesterase-5 inhibitors (sildenafil, tadalafil).
- Refer to urogynecology for pelvic floor therapy.
- Address psychological factors: counselling, sex therapy.
Relapse Management
A relapse (attack/exacerbation) is new or worsening neurological symptoms lasting >24 hours in the absence of fever or infection.
First, exclude pseudo-relapse (Uhthoff phenomenon from fever/infection — treat the underlying cause).
True relapses:
- High-dose IV methylprednisolone 1 g/day × 3–5 days shortens relapse duration.
- Does not alter long-term disability outcome.
- Nursing: monitor blood glucose (hyperglycaemia), blood pressure (hypertension), mood changes (steroid-induced psychiatric effects), GI upset, fluid retention.
- Administer with PPI/H2 blocker for GI protection.
- Plasmapheresis for steroid-refractory relapses.
Disease-Modifying Therapies (DMTs)
DMTs reduce relapse rate, new MRI lesions, and slow disability accumulation. Nurses play a central role in education, injection training, monitoring, and side effect management.
Injectable Agents (first-line)
| Drug | Route | Key Nursing Points |
|---|---|---|
| Interferon-β (Avonex, Rebif, Betaseron, Extavia) | IM or SC injection | Flu-like symptoms (manage with NSAIDs/paracetamol, take at bedtime); injection-site reactions; monitor LFTs and CBCs |
| Glatiramer acetate (Copaxone) | SC daily or 3×/week | Immediate post-injection reaction (flushing, chest tightness — transient, benign, <30 mins); lipodystrophy at injection sites; rotate sites |
Oral Agents
| Drug | Mechanism | Key Nursing Points |
|---|---|---|
| Fingolimod (Gilenya) | S1P receptor modulator | First dose monitoring for 6 hours (bradycardia, AV block); ophthalmology check (macular oedema); varicella titres before starting; PML risk |
| Dimethyl fumarate (Tecfidera) | Nrf2 pathway | Flushing, GI upset (reduce with food/aspirin); monitor lymphocyte count; PML risk with lymphopenia |
| Teriflunomide (Aubagio) | Pyrimidine synthesis inhibitor | Teratogenic — use contraception; hair thinning; LFT monitoring |
| Siponimod, Ozanimod | S1P modulators | Similar to fingolimod |
| Cladribine (Mavenclad) | Lymphocyte depletion | Annual courses; prolonged lymphopenia; infection risk; teratogenic |
High-Efficacy IV/SC Agents
| Drug | Mechanism | Key Nursing Points |
|---|---|---|
| Natalizumab (Tysabri) | Anti-α4-integrin | Monthly infusion; JC virus antibody testing (PML risk); infusion reactions; hepatotoxicity monitoring |
| Ocrelizumab (Ocrevus) | Anti-CD20 (B-cell depletion) | IV infusion 6-monthly; infusion reactions; hepatitis B screening; infection risk; approved for PPMS |
| Alemtuzumab (Lemtrada) | Anti-CD52 | Annual courses; serious autoimmune side effects (thyroid disease, ITP, nephropathy) — prolonged monitoring programme |
Strategy tip from Goldman-Cecil: Start with an oral agent for typical newly diagnosed RR-MS. Switch to a high-efficacy monoclonal antibody if the patient has a severe relapse, multiple relapses, or new MRI lesions. — Goldman-Cecil Medicine
Nursing Care Priorities Summary
| Priority | Key Actions |
|---|---|
| Safety | Fall prevention: bed rails, non-slip footwear, mobility aids; Uhthoff education; seizure precautions (if on dalfampridine) |
| Infection prevention | UTI surveillance; vaccination (avoid live vaccines in patients on immunosuppressants); respiratory hygiene |
| Medication management | DMT injection technique training; side effect monitoring; never abruptly stop baclofen |
| Patient education | Disease course, relapse recognition, heat avoidance, medication adherence, MS Society resources |
| Psychosocial support | Depression/anxiety screening, social work referral, support groups, caregiver support |
| Rehabilitation | Physiotherapy, occupational therapy, speech therapy (dysarthria/dysphagia), dietitian |
| Bone health | Vitamin D + calcium supplementation; bisphosphonates if osteoporosis present |
| Bowel/bladder program | Individualised voiding schedules, catheter technique if self-catheterising |
| Skin integrity | Pressure area care for patients with reduced mobility or sensation |
Prognosis
- Annual mortality risk ~2× general population; average lifespan reduced by ~8 years.
- ~85% start with RRMS; ~15% are PPMS.
- 1/3 will eventually require a wheelchair; ~50% need assistive devices; ~2/3 have disability preventing employment.
- African Americans and men tend to have more aggressive disease.
- Early immunomodulating therapy appears to slow disability progression.
— Goldman-Cecil Medicine, International Edition | Bradley and Daroff's Neurology in Clinical Practice
Key Points for NCLEX / Exams
- MS is disseminated in time AND space — the diagnostic hallmark.
- Uhthoff phenomenon = heat worsens symptoms — NOT a relapse; cool the patient.
- Lhermitte sign = electric shock down spine on neck flexion — cervical cord involvement.
- Never stop baclofen abruptly — risk of life-threatening withdrawal (seizures, hyperthermia).
- Post-void residual >300 mL requires intervention.
- Steroid treatment for relapses speeds recovery but does NOT improve long-term outcome.
- Optic neuritis — retrobulbar, so the disc looks normal; look for a RAPD (Marcus-Gunn pupil).
- Gadolinium enhancement on MRI = active inflammation.
- For fatigue: rule out treatable causes (depression, insomnia, anaemia, thyroid disease) first.
- Patients on high-efficacy DMTs need JC virus antibody monitoring (PML risk).
This is a shared conversation. Sign in to Orris to start your own chat.