Stretch reflex regulation and applied
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Now I have comprehensive information. Let me compile the full answer.
Stretch Reflex: Regulation and Applied Aspects
1. Definition and Basic Circuit
The stretch reflex (myotatic reflex) is the simplest monosynaptic spinal reflex. When a skeletal muscle with an intact nerve supply is suddenly stretched, it reflexly contracts. The receptor is the muscle spindle, located within the fleshy belly of the muscle.
Pathway (monosynaptic loop):
- Muscle stretch → activates muscle spindle (Ia afferents)
- Ia afferent enters dorsal root → synapses directly on alpha (α) motor neurons in anterior horn
- α motor neuron fires → contracts the same (homonymous) muscle
- Muscle shortens → spindle unloads → Ia firing returns to baseline
The neurotransmitter at the central synapse is glutamate. The central delay for the knee jerk reflex is only 0.6-0.9 ms, confirming a single synapse.
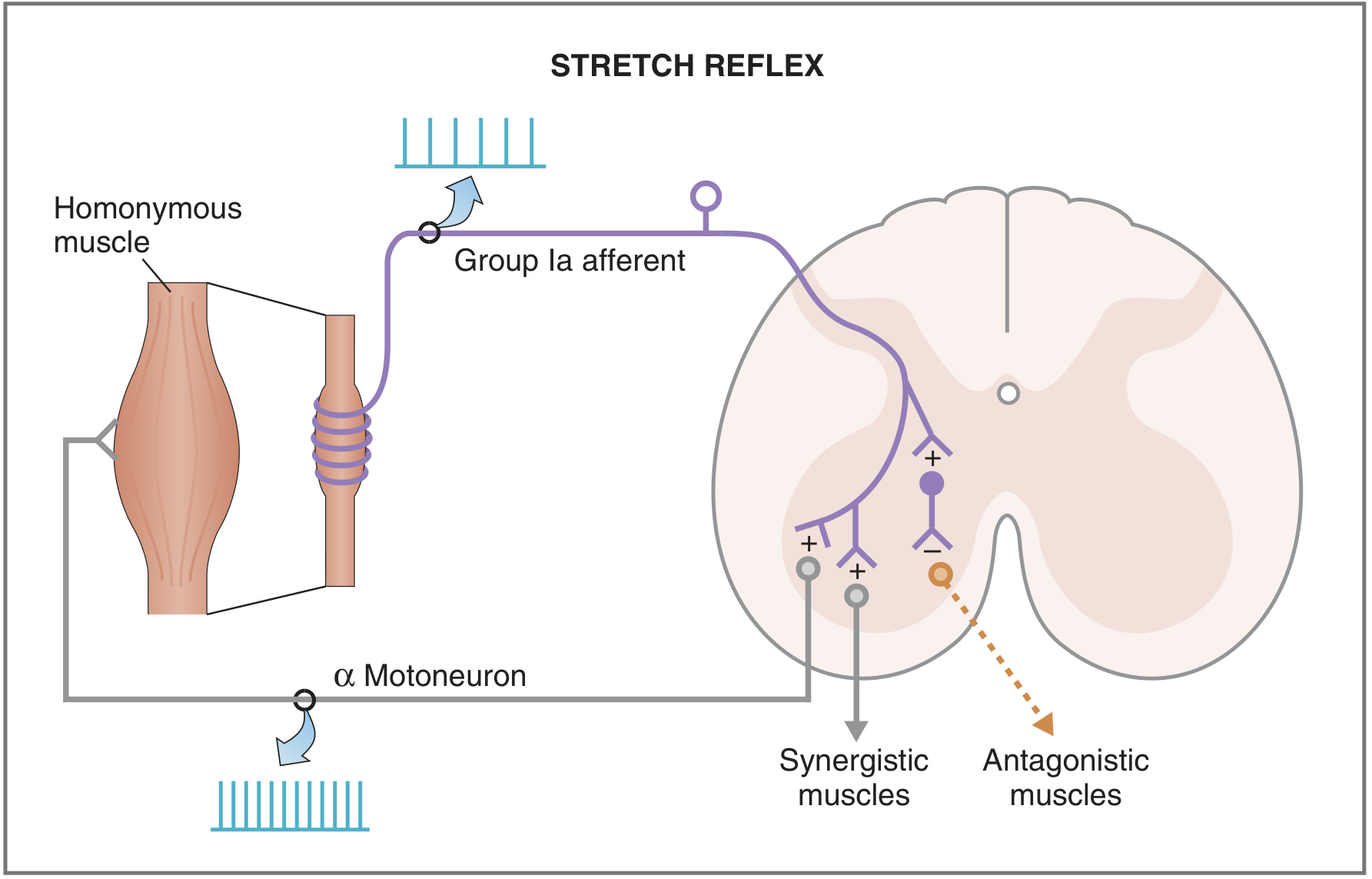
Stretch reflex circuit: Ia afferents from the muscle spindle excite (+) the homonymous muscle's α motor neurons and synergistic muscles, while inhibiting (-) antagonistic muscles via interneurons (Costanzo Physiology)
Simultaneously, collateral branches cause:
- Contraction of synergistic muscles
- Relaxation of antagonistic muscles (reciprocal inhibition via inhibitory interneurons)
2. Structure of the Muscle Spindle
The spindle is the key sensory element. It has three essential components:
| Component | Details |
|---|---|
| Intrafusal fibers | Specialized fibers in parallel with extrafusal fibers; do not contribute to contractile force |
| Sensory endings (afferents) | Group Ia (primary) wraps the center of all fibers; Group II (secondary) at adjacent regions |
| Motor supply (gamma efferents) | γ-motor neurons (3-6 µm, ~30% of ventral root fibers) supply intrafusal fibers |
Two types of intrafusal fibers:
- Nuclear bag fibers (dynamic and static subtypes) - contain many nuclei in a dilated central area
- Nuclear chain fibers - thinner, shorter, no bag
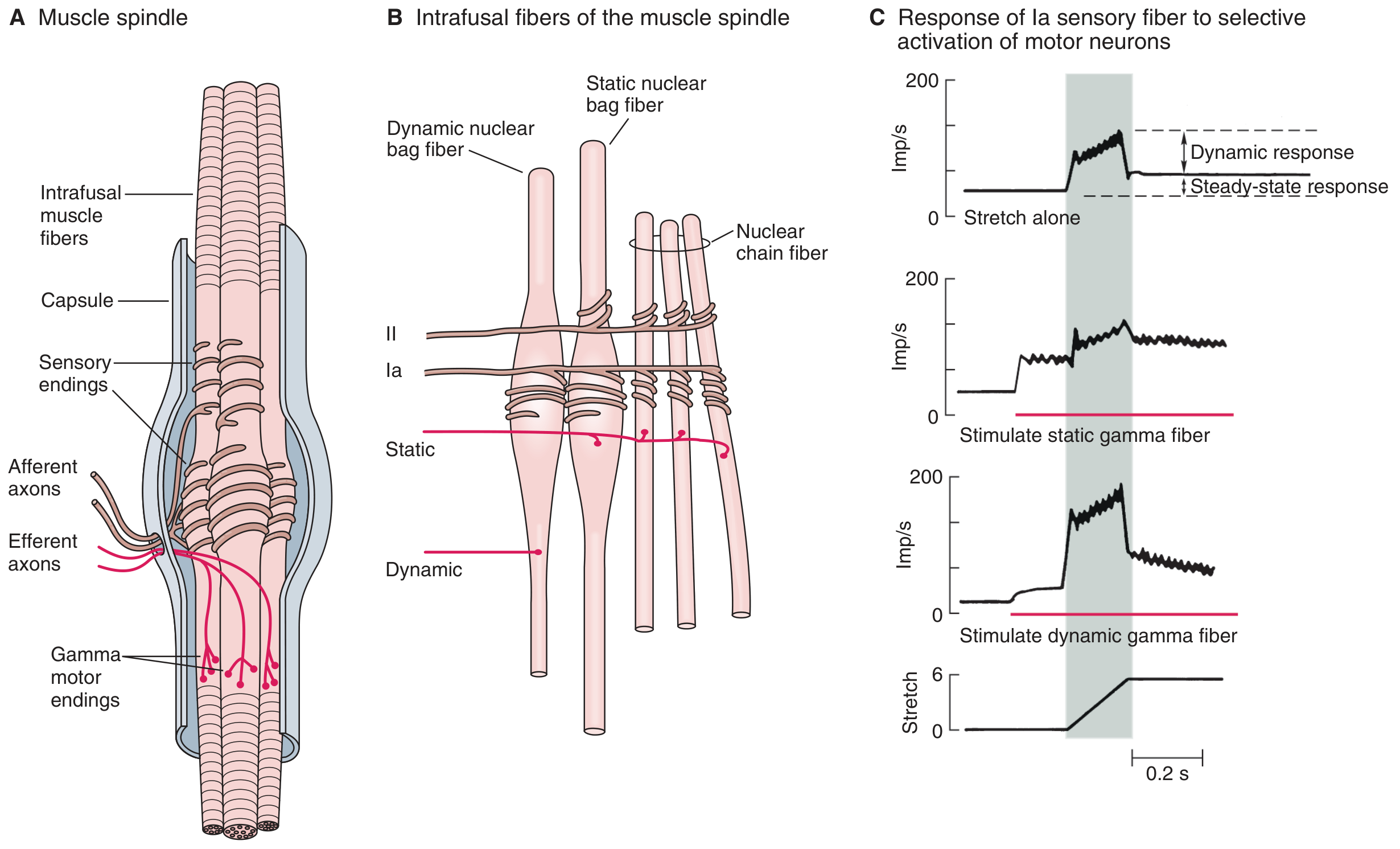
Mammalian muscle spindle (A) structure, (B) intrafusal fiber types and their innervation, (C) effect of static vs. dynamic gamma motor neuron stimulation on Ia firing (Ganong's Review)
3. Dynamic vs. Static Stretch Reflex
| Feature | Dynamic Stretch Reflex | Static Stretch Reflex |
|---|---|---|
| Stimulus | Rapid change in muscle length (phasic) | Sustained/maintained stretch (tonic) |
| Afferent | Primarily Ia (primary ending) | Both Ia and Group II (secondary) |
| Duration | Brief - over within a fraction of a second | Prolonged - continues as long as stretch maintained |
| Function | Opposes sudden changes in muscle length | Maintains constant muscle contraction/length |
4. Regulation: The Gamma Motor (Fusimotor) System
The γ-motor neurons are the primary regulators of stretch reflex sensitivity. They set the "gain" of the spindle.
Two types of gamma motor neurons:
Dynamic γ-motor neurons:
- Supply dynamic nuclear bag fibers
- Increase the phasic/dynamic sensitivity of Ia endings
- Enhance the response to rate of stretch (velocity)
Static γ-motor neurons:
- Supply static nuclear bag fibers + nuclear chain fibers
- Increase tonic/steady-state firing of both Ia and Group II afferents
- Decrease dynamic sensitivity of Ia afferents
- Prevent silencing of Ia afferents during maintained stretch
Alpha-Gamma Coactivation:
When the CNS sends signals to contract a muscle (via α motor neurons), it simultaneously activates γ motor neurons - called coactivation. This serves two purposes:
- Keeps the spindle taut (prevents "unloading") during whole-muscle contraction - maintains reflex sensitivity
- Maintains the damping/smoothing function of the spindle regardless of muscle length changes
Brain Areas Controlling the Gamma System:
The gamma efferent system is controlled hierarchically:
- Bulboreticular facilitatory area (brain stem) - primary driver; concerned with antigravity contractions
- Cerebellum - modulates via bulboreticular area
- Basal ganglia - modulates via bulboreticular area
- Cerebral cortex - transmits impulses into bulboreticular area
5. Damping and Stabilization Functions
Damping/Smoothing: The stretch reflex smooths jerky motor commands. Even when the spinal cord sends uneven bursts to a muscle, the spindle feedback averages out the oscillations, producing a smooth contraction. If spindle afferents are sectioned, muscle contractions become jerky.
Stabilization of Joint Position: When the bulboreticular area activates spindles on both sides of a joint simultaneously, both opposing muscle groups tighten, strongly stabilizing the joint. This is critical during fine motor tasks - proximal joint stabilization allows distal fine movements (e.g., steadying the elbow to allow finger work).
6. Inverse Stretch Reflex (Golgi Tendon Organ)
| Feature | Stretch Reflex | Inverse Stretch Reflex |
|---|---|---|
| Receptor | Muscle spindle (parallel to fibers) | Golgi tendon organ (in series with fibers) |
| Afferent | Group Ia | Group Ib |
| Stimulus | Muscle stretch (lengthening) | Muscle contraction (force/tension) |
| Synapses | Monosynaptic | Disynaptic (via inhibitory interneuron - glycine) |
| Response | Muscle contraction | Muscle relaxation |
| Function | Resists excessive stretch | Protects against excessive tension |
With very strong stretch, Ib activation hyperpolarizes the motor neuron so strongly it stops firing - producing the "clasp knife" response seen in spasticity.
7. Clinical Applications
Deep Tendon Reflexes (DTRs)
Clinicians use stretch reflexes to assess the "tone" (degree of facilitation) being sent from the brain to the spinal cord.
DTR Grading Scale:
| Grade | Interpretation |
|---|---|
| 0 | Absent |
| 1+ | Hypoactive |
| 2+ | Brisk/normal |
| 3+ | Hyperactive, no clonus |
| 4+ | Hyperactive, mild clonus |
| 5+ | Hyperactive, sustained clonus |
Common DTRs and their spinal levels:
- Biceps: C5, C6
- Triceps: C7
- Patellar (knee jerk): L4
- Achilles (ankle jerk): S1
- Masseter: trigeminal nerve
Hyporeflexia / Absent Reflexes
Absence of a reflex can indicate a lesion anywhere along the reflex arc:
- Muscle spindle damage
- Ia afferent neuropathy (most common cause: peripheral neuropathy from diabetes, alcoholism, toxins)
- Alpha motor neuron lesion (lower motor neuron lesion)
Hyperreflexia and Spasticity
Hyperactive reflexes result from interruption of corticospinal and other descending pathways that normally suppress reflex arc activity (disinhibition). Causes include:
- Cerebral cortex lesions (strokes, brain tumors) - affects contralateral muscles
- Upper motor neuron lesions at any level
- Increased excitation of the bulboreticular facilitatory area
Clonus
Clonus is rhythmic oscillation of the stretch reflex, seen when reflex sensitivity is markedly increased:
- Example (ankle clonus): sudden plantarflexion stretch → gastrocnemius reflex contracts → body rises → spindle unloads → relaxes → body drops → cycle repeats
- Clonus indicates high facilitation of the spinal cord (upper motor neuron pathology)
- Clinicians test by applying sudden, maintained stretch and observing for sustained oscillation
Physiologic Tremor
The phasic Ia response to dynamic stretch helps dampen normal feedback loop oscillations. Minor oscillations (~10 Hz, barely visible) constitute physiologic tremor, a normal phenomenon. The dynamic spindle response is a key damping mechanism against this tremor.
Summary Table
| Aspect | Detail |
|---|---|
| Reflex type | Monosynaptic (Ia→α motor neuron) |
| Receptor | Muscle spindle (intrafusal fibers) |
| Afferents | Ia (dynamic + static); Group II (static) |
| Motor regulator | γ-motor neurons (dynamic & static) |
| CNS control | Bulboreticular area, cerebellum, basal ganglia, cortex |
| Key mechanism | Alpha-gamma coactivation; damping; joint stabilization |
| Clinical uses | DTR assessment, spasticity evaluation, clonus testing |
| Hyporeflexia | Peripheral neuropathy, LMN lesion |
| Hyperreflexia/clonus | UMN lesion, loss of descending inhibition |
Sources:
- Guyton and Hall Textbook of Medical Physiology, Ch. 55
- Ganong's Review of Medical Physiology, 26th Edition, Ch. 12
- Costanzo Physiology, 7th Edition, Ch. 3
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have all the material needed for a complete answer to all three parts. Let me compile the full response.
Q1. Cerebellar Haemorrhage - Model Answer
Case Summary: 18-year-old male, cerebellar haemorrhage, presenting with:
- Jerky eye movements (nystagmus)
- Sways when standing (disequilibrium/truncal ataxia)
- Drunken gait (wide-based ataxic gait)
(a) Which Part of the Cerebellum is Most Likely Affected? (2 marks)
The clinical triad of nystagmus + disequilibrium (swaying on standing) + ataxic/drunken gait points to the Vestibulocerebellum (Flocculonodular lobe / Archicerebellum).
| Functional Division | Anatomic Region | Key Functions |
|---|---|---|
| Vestibulocerebellum | Flocculonodular lobe (flocculus + nodulus) | Balance, equilibrium, eye movements, head position coordination |
| Spinocerebellum | Vermis + intermediate hemispheres | Posture, axial/limb coordination |
| Cerebrocerebellum | Lateral hemispheres | Motor planning, fine voluntary movements |
The vestibulocerebellum receives input from the vestibular nuclei and sends output back to vestibular nuclei - this is why lesions here produce nystagmus (abnormal eye movement control) and loss of balance/equilibrium (drunken gait, swaying). The deep nucleus involved is the lateral vestibular nucleus of Deiters.
"The major dysfunction seen after damage to the vestibulocerebellum is ataxia, disequilibrium, and nystagmus." - Ganong's Review of Medical Physiology, 26th Ed.
(b) Features Seen in Cerebellar Lesion (5 marks)
Cerebellar lesions produce a characteristic constellation of signs. The mnemonic DANISH is helpful:
1. Dysdiadochokinesia
- Inability to perform rapidly alternating opposite movements (e.g., repeated pronation/supination of the hands)
- Due to inability to stop one movement and start the opposite rapidly
2. Ataxia
- Wide-based, unsteady, "drunken" gait
- Incoordination due to errors in rate, range, force, and direction of movement
- Manifest also as scanning/staccato speech (slurred, slow, dysarthric)
3. Nystagmus
- Jerky oscillatory eye movements
- Particularly associated with vestibulocerebellar lesions
- Due to loss of smooth coordination of eye movements
4. Intention Tremor (+ Dysmetria)
- Tremor that worsens on approaching a target (unlike resting tremor of Parkinsonism)
- Dysmetria: overshooting or undershooting a target (e.g., finger-nose test)
- The correction itself overshoots, causing the finger to oscillate (intention tremor)
5. Slurred (Scanning) Speech
- Dysarthria due to incoordination of speech muscles
- Speech is broken into syllables with inappropriate pauses
6. Hypotonia
- Decreased resistance to passive movement of joints
- Due to loss of cerebellar facilitatory drive on alpha motor neurons
Additional Signs:
- Rebound phenomenon: inability to check movement suddenly (forearm flies back when resistance is removed)
- Decomposition of movement: multi-joint tasks are broken down and performed one joint at a time
- Delay in initiating movement (especially with cerebrocerebellum damage)
- Pendular knee jerk: reflex oscillates instead of a single jerk, due to hypotonia
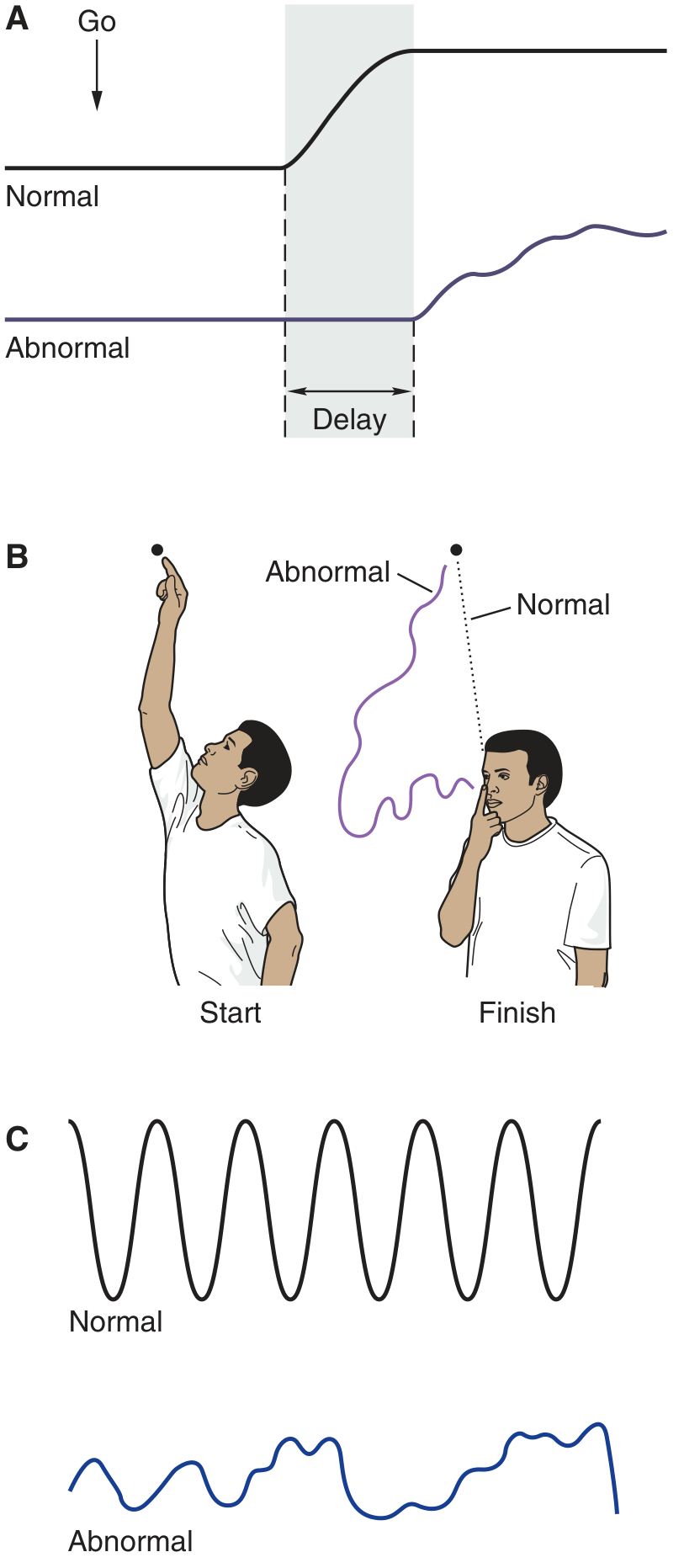
Typical defects of cerebellar disease: (A) delayed initiation, (B) dysmetria and intention tremor, (C) dysdiadochokinesia - Ganong's Review
Regional localization of signs:
| Region Damaged | Dominant Features |
|---|---|
| Vestibulocerebellum (flocculonodular lobe) | Nystagmus, disequilibrium, ataxia |
| Spinocerebellum (vermis + fastigial nucleus) | Scanning speech, truncal/axial ataxia, posture disturbance |
| Cerebrocerebellum (lateral hemispheres + dentate) | Delayed movement initiation, decomposition of movement, intention tremor |
Note: Cerebellar signs are ipsilateral to the lesion (because cerebellar output crosses twice - once in the cerebellum and once in the brainstem - ending up ipsilateral).
(c) Comparator Servo Mechanism of the Cerebellum (3 marks)
The cerebellum acts as a biological comparator - it continuously compares the intended movement (efference copy/motor plan) with the actual movement (sensory feedback) and sends error-correcting signals to adjust the movement in real time.
The Mechanism - Step by Step:
Motor Cortex
|
|---- Motor Command (efference copy/"reference signal")
| ↓
| CEREBELLUM ← Actual movement feedback (from proprioceptors,
| | vestibular system, visual system)
| |
| Compares intended vs. actual
| |
| Generates ERROR SIGNAL
| |
←-----------+--- Corrective output (via thalamus → motor cortex,
or brainstem → spinal cord)
Three Inputs to the Comparator:
- Motor plan (intended movement) - from motor cortex via corticopontine-pontocerebellar fibers (mossy fibers) → what movement is desired
- Peripheral sensory feedback (actual movement) - from proprioceptors, vestibular apparatus, visual system (via spinocerebellar tracts, vestibular inputs)
- Ongoing motor commands - collateral copies of signals going to muscles
How the Cerebellum Corrects Errors:
- If actual movement deviates from intended: cerebellum detects the discrepancy
- Purkinje cell outputs (inhibitory, via GABA) modulate the deep cerebellar nuclei
- Deep nuclei send excitatory corrections via:
- Dentate nucleus → VL thalamus → motor cortex (for voluntary movement)
- Fastigial nucleus → vestibulospinal/reticulospinal tracts (for posture/balance)
- Interposed nucleus → red nucleus → rubrospinal tract (for limb coordination)
Why is this called a "Servo" mechanism?
A servo-mechanism is a control system that uses negative feedback to self-correct toward a desired output. The cerebellum functions identically:
- Set point = intended movement (motor plan)
- Actual output = real limb movement (sensory feedback)
- Error signal = difference between the two
- Correction = cerebellar output adjusting ongoing motor commands
When the Comparator Fails (Cerebellar Lesion):
- The error cannot be detected and corrected in real time
- Result: dysmetria (overshooting), intention tremor (repeated failed corrections oscillate), ataxia
- The patient cannot execute smooth goal-directed movements
"The spinocerebellum receives proprioceptive input from the body as well as a copy of the motor plan from the motor cortex" - allowing it to compare intended vs. actual movement (Ganong's Review, 26th Ed.)
Sources: Ganong's Review of Medical Physiology 26th Ed., Ch. 12 | Adams and Victor's Principles of Neurology 12th Ed., Ch. 5 | Costanzo Physiology 7th Ed., Ch. 3
This is a shared conversation. Sign in to Orris to start your own chat.