Management of CIN and critically evaluate various treatment options for CIN. Give detail answer for gynecological oncologist. Give answer in table, flowcharts and images and use recent advance guidelines
Reading File
Finding Sources
Searching PubMed
"cervical intraepithelial neoplasia" AND management
Searching the Web
ASCCP 2023 2024 CIN management guidelines treatment colposcopy
Finding Sources
Finding Sources
Searching PubMed
"CIN2" OR "CIN3" AND treatment excision ablation outcomes
Reading File
Finding Sources
Searching PubMed
"cervical intraepithelial neoplasia" AND LEEP cryotherapy cold knife cone
Reading File
Finding Sources
Searching PubMed
cervical precancer treatment loop excision ablation comparison
Finding Sources
Reading Article
Reading Web Page
CIN management treatment guidelines 2024 2025
Finding Sources
Searching PubMed
"CIN2" regression surveillance observation versus treatment
Reading File
Reading File
Reading File
Loading Image
Searching PubMed
adjuvant HPV vaccination after CIN treatment recurrence prevention
Reading File
Loading Image
Reading File
Reading File
Loading Image
Management of Cervical Intraepithelial Neoplasia (CIN)
A Comprehensive Reference for Gynecological Oncologists
Updated to ASCCP 2019/2023/2025 Risk-Based Guidelines, USPSTF 2024 Draft, and Latest Evidence
1. PATHOLOGICAL CLASSIFICATION & NATURAL HISTORY
Colposcopic appearance of CIN 2 (HPV/CIN 2 white lesion with surface spicules):
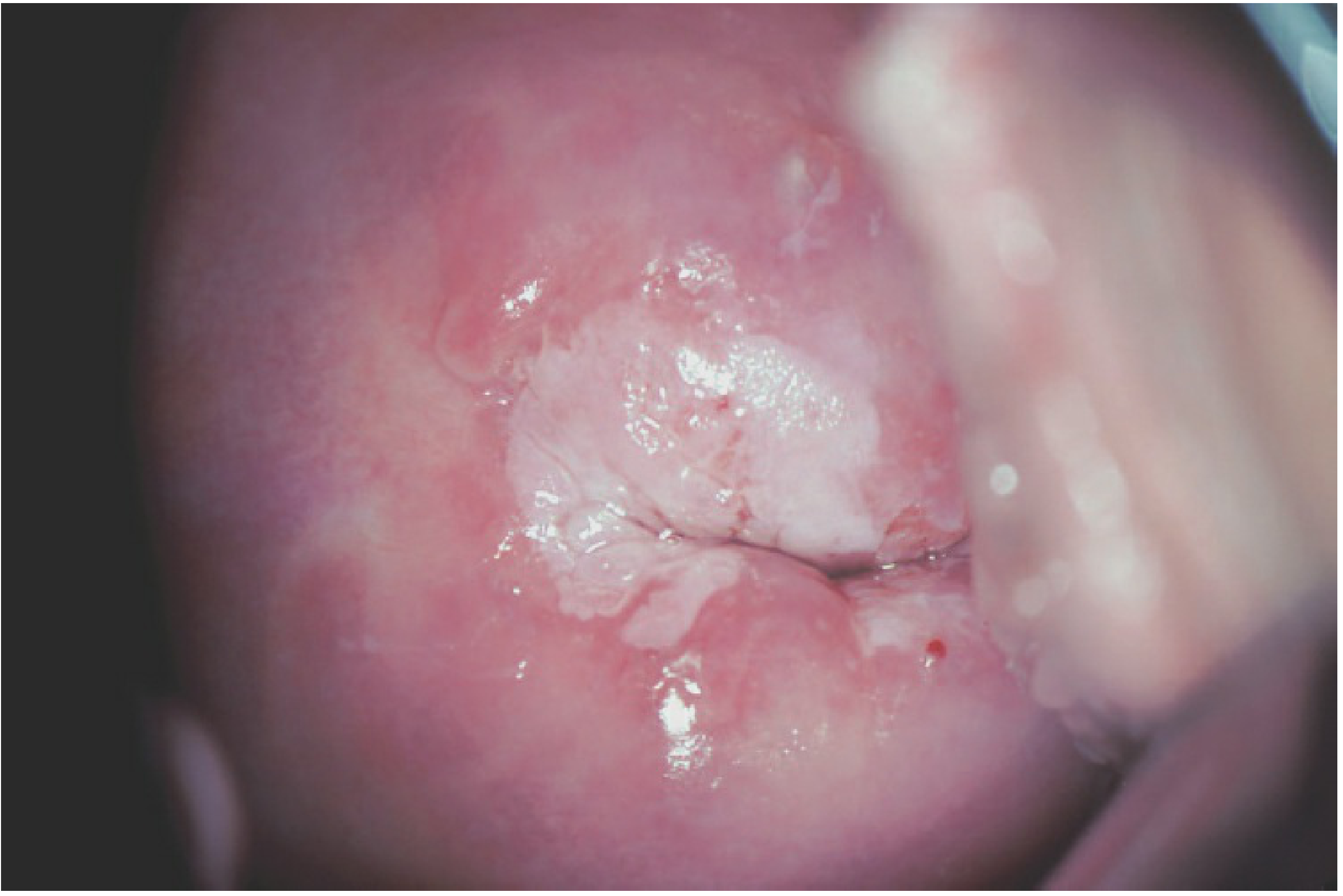
Table 1: CIN Classification, Histology & Natural History
| Grade | Bethesda (Cytology) | Histologic Features | Regression | Persistence | Progression to CIS | Progression to Invasion |
|---|---|---|---|---|---|---|
| CIN 1 (LSIL) | LSIL | Koilocytes, mild dysplasia lower 1/3 of epithelium; mitoses limited to lower 1/3 | 60-85% within 2 yr | 20% | 11% | 1% |
| CIN 2 (hHSIL) | HSIL | Dysplastic cells lower 2/3; increased mitotic activity | 40-60% | 20-30% | 20% | 5% |
| CIN 3 (HSIL/CIS) | HSIL | Full-thickness or near full-thickness dysplasia; high N:C ratio | 32% | 40% | - | 12-22% |
Key Biology: CIN originates at the squamocolumnar junction (SCJ) in the transformation zone. HPV-16 is the most common type in both CIN 2-3 and invasive cancer. Oncogenic transformation requires E6/E7 oncoprotein expression. - Berek & Novak's Gynecology, p. 834
2. OVERVIEW: ASCCP 2019/2025 RISK-BASED MANAGEMENT FRAMEWORK
The foundational shift from the 2012 to 2019 guidelines is risk-based management using the CIN 3+ risk threshold:
| Risk Threshold | Recommended Action |
|---|---|
| Immediate CIN 3+ risk ≥ 60% | Treatment preferred; colposcopy acceptable |
| Immediate CIN 3+ risk ≥ 25% | Colposcopy or treatment |
| Immediate CIN 3+ risk ≥ 4% | Colposcopy recommended |
| 5-year CIN 3+ risk ≥ 0.55% but < 4% | 1-year surveillance |
| 5-year CIN 3+ risk < 0.55% | 3-5 year surveillance / return to routine screening |
2025 Additions (ASCCP Enduring Guidelines):
- Extended HPV genotyping now integrated into management (HPV 16/18 vs. other HR types vs. HPV 45/33/58/31, etc.)
- p16/Ki-67 Dual Stain (DS) incorporated as triage tool (April 2024 guideline)
- Self-collected vaginal HPV specimens now acceptable (April 2025 guideline)
- Adjuvant HPV vaccination at time of treatment now formally recommended by ASCCP (December 2025)
3. COLPOSCOPY: THE GATEWAY TO MANAGEMENT
Indications for Colposcopy (ASCCP 2019/2025)
| Clinical Scenario | Action |
|---|---|
| HPV 16 positive (any cytology) | Colposcopy |
| HPV 18 positive (any cytology) | Colposcopy |
| HPV 16/18 + HSIL | Treatment preferred; colposcopy acceptable |
| Other HR HPV + HSIL or ASC-H | Colposcopy |
| ASC-US + HPV positive | Colposcopy |
| LSIL (age ≥ 25) | Colposcopy |
| HSIL (any age ≥ 25) | Colposcopy or expedited treatment |
| AGC any subtype | Colposcopy + ECC + endometrial sampling (if age ≥ 35 or AUB) |
| DS positive (p16/Ki-67) | Colposcopy |
| 2nd consecutive HPV positive (non-16/18) | Colposcopy |
Colposcopy Quality Criteria (IFCPC 2011 Terminology)
| Term | Definition | Clinical Implication |
|---|---|---|
| Satisfactory | Entire SCJ and all lesion margins visible | Ablation permissible if appropriate |
| Unsatisfactory | SCJ not fully visible | Excision required |
| TZ Type 1 | Ectocervical, fully visible | Ablation appropriate |
| TZ Type 2 | Endocervical component, visible | Ablation may be used |
| TZ Type 3 | Endocervical, not fully visible | Excision mandatory |
4. MANAGEMENT FLOWCHARTS
Flowchart 1: CIN 1 Management
CIN 1 preceded by ASC-US, ASC-H, or LSIL cytology:
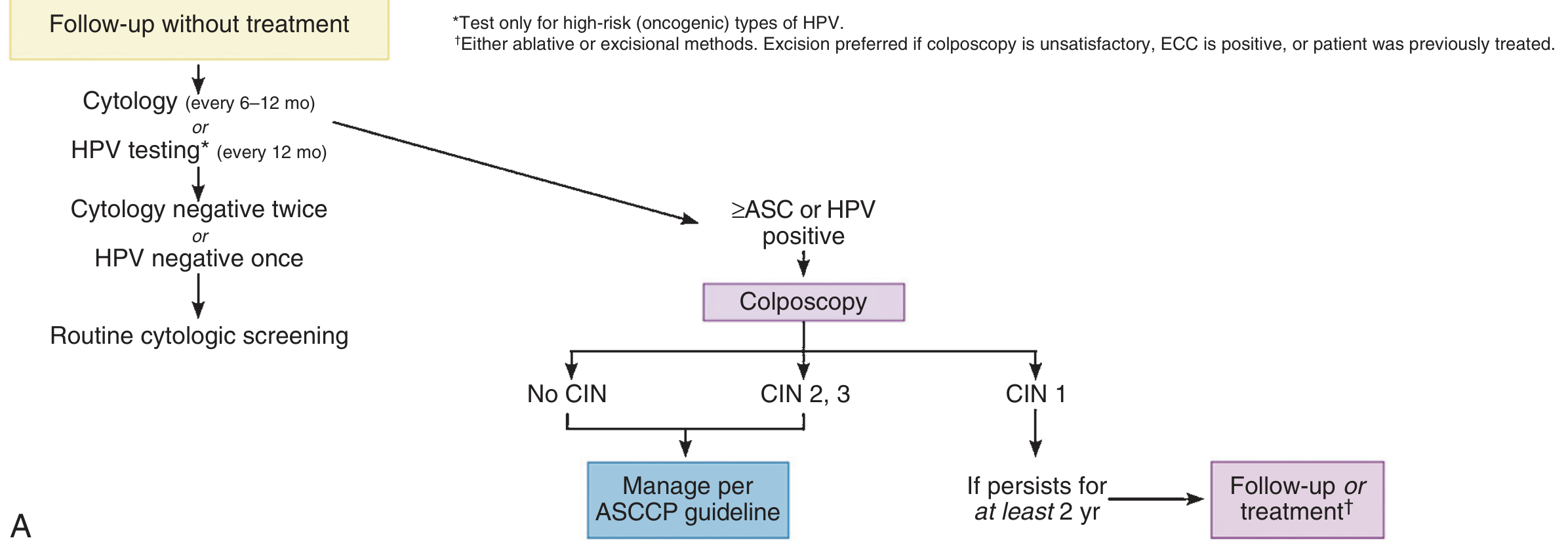
Summary of CIN 1 Management:
CIN 1 (LSIL)
├── Observation PREFERRED (regression 60-85%)
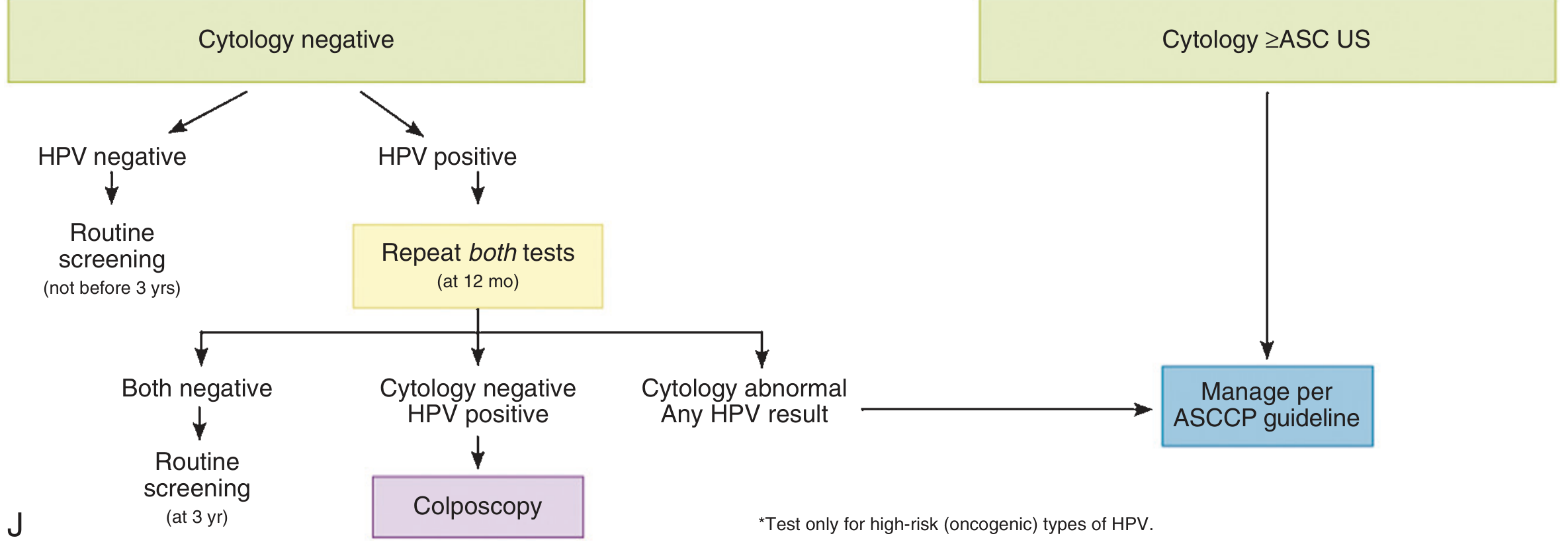
│ ├── Co-test (cytology + HPV) at 12 months
│ │ ├── Both negative → Co-test in 3 years → Routine screening
│ │ ├── HPV positive, cytology negative → Colposcopy
│ │ └── Cytology ≥ ASC (any HPV) → Manage per ASCCP guideline
│ └── If CIN 1 persists ≥ 2 years
│ ├── Continue surveillance (acceptable), OR
│ └── Treatment (ablation or excision if TZ visible)
└── NEVER treat CIN 1 as initial management
Flowchart 2: CIN 1 Post-HSIL/AGC-NOS Cytology
CIN 1 preceded by HSIL or AGC-NOS
├── Review of all material (cytology + colposcopy + biopsy)
├── If unsatisfactory colposcopy → Diagnostic excisional procedure
├── Repeat cytology + colposcopy at 6 months
│ ├── Negative x2 → Routine screening
│ ├── HSIL at any repeat → Diagnostic excision
│ └── No change on biopsy → Either observation OR diagnostic excision
Flowchart 3: CIN 1 Post-Treatment Surveillance (co-testing)
Flowchart 4: CIN 2 & CIN 3 Management
CIN 2 / CIN 3 Confirmed on Biopsy
│
├── SPECIAL POPULATIONS (manage differently):
│ ├── Age 21-24 years → Observation acceptable for CIN 2 (not CIN 3)
│ ├── PREGNANCY → Defer treatment; repeat colposcopy q12 weeks; treat postpartum
│ └── Immunocompromised → Treatment recommended regardless of grade
│
├── Satisfactory Colposcopy (TZ fully visible)?
│ ├── YES → Excision OR Ablation of transformation zone (either acceptable)
│ │ [See Section 5 for choice]
│ └── NO → Diagnostic excisional procedure ONLY (ablation contraindicated)
│
├── Recurrent CIN 2,3 → Diagnostic excisional procedure
│
└── POST-TREATMENT FOLLOW-UP:
├── Co-test (cytology + HPV) at 6 months AND 12 months
├── Negative x2 → Annual co-test for 3 years → Return to 3-year co-testing for ≥20 years
├── ≥ ASC on cytology → Colposcopy
└── HPV positive → Colposcopy
5. CRITICAL EVALUATION OF TREATMENT OPTIONS
Table 2: Comprehensive Comparison of Treatment Modalities
| Parameter | Cryotherapy | CO₂ Laser Ablation | Cold Coagulation | LEEP/LLETZ | Laser Conization | Cold Knife Conization (CKC) | Hysterectomy |
|---|---|---|---|---|---|---|---|
| Mechanism | Freeze-thaw (-20°C), ice crystal cell death | Laser vaporization of tissue | Thermal destruction at 100°C | Electrosurgical loop excision | Laser excision with CO₂ | Scalpel excision | Uterus removal |
| Tissue specimen | None | None | None | Yes (margins assessable) | Yes (margins assessable) | Yes (best margins) | Yes |
| Cure rate - CIN 2/3 | 77-87% | 90-95% | 87-90% | 92-98% | 94-98% | 93-97% | ~99% |
| Treatment failure risk vs. LLETZ | OR 1.84 (CI 1.27-2.24) | OR 1.69 (CI 1.27-2.24) | OR 1.09 (CI 0.68-1.74) | Reference | OR 0.59 (CI 0.44-0.79) | OR 0.63 (CI 0.50-0.81) | - |
| Preterm birth risk (vs. untreated) | No increase | No increase | No increase | OR 1.37 (CI 1.16-1.62) | OR 1.77 (CI 1.29-2.43) | OR 2.27 (CI 1.70-3.02) | N/A |
| Requires colposcopy | Yes | Yes | Yes | Yes (best alone) | Yes | Yes | Yes |
| Anesthesia | None / local | Local | None / local | Local (GA in RCT: similar outcomes) | Local/General | General/Spinal | General/Spinal |
| Endocervical assessment | Not possible | Not possible | Not possible | ECC can accompany | ECC can accompany | Full endocervical specimen | Full specimen |
| Setting | Outpatient/clinic | Outpatient | Outpatient | Outpatient | Outpatient/Theatre | Theatre | Theatre |
| Cost | Lowest | Moderate | Low | Low-Moderate | Moderate-High | High | Highest |
| Contraindications | Unsatisfactory colposcopy, TZ3, ECC+, endocervical extension, recurrence, microinvasion suspected | Unsatisfactory colposcopy, microinvasion suspected | Same as cryotherapy | None (preferred in most cases) | None | None | Desire for fertility |
| Key advantage | Simple, no equipment | Precise, no thermal artifact | Simple, cheap, comparable to LEEP | Gold standard outpatient; specimen for histology | Best precision; lowest recurrence among ablative | Best margins; gold standard for glandular | Definitive cure |
| Key disadvantage | No specimen; low cure rate for large/endocervical lesions | Equipment cost; skill required | Limited availability; less data | Thermal artifact at margins; preterm birth risk | Cost; skill; laser access | Operative morbidity; preterm birth risk highest | Major surgery; fertility loss |
Evidence for cure rates and preterm birth from: Lancet Oncology network meta-analysis, Athanasiou et al. 2022 (PMID 35835138) - 19,240 patients, 71 studies.
6. ABLATIVE vs. EXCISIONAL TREATMENT: DECISION FRAMEWORK
Table 3: When to Choose Ablation vs. Excision
| Criterion | Ablation Acceptable | Excision REQUIRED |
|---|---|---|
| Colposcopy adequacy | Satisfactory (TZ 1 or 2) | Unsatisfactory (TZ 3) |
| Endocervical curettage | Negative | Positive |
| Lesion extent | Limited to ectocervix | Extends into endocervical canal |
| Prior treatment | First treatment | Recurrent lesion |
| Cytology-histology correlation | CIN grade matches cytology | Discordant (higher cytology grade) |
| Cancer excluded | Clearly excluded | Cannot exclude microinvasion |
| AIS (adenocarcinoma in situ) | Never | Always (CKC preferred) |
| Patient preference (reproducibility) | Acceptable | Preferred for oncologic documentation |
Ablation: Absolute Contraindications (all require excision)
- Unsatisfactory colposcopy
- ECC positive for dysplasia or glandular abnormality
- Histology-cytology discordance (higher cytologic grade)
- Microinvasion suspected
- AIS present
- Previously treated, recurrent CIN 2/3
7. SPECIFIC TREATMENT PROCEDURES - DETAILED EVALUATION
7a. LEEP/LLETZ (Large Loop Excision of the Transformation Zone)
Status: Current Gold Standard for outpatient management of CIN 2/3
Advantages:
- Histologic specimen with assessable margins
- Outpatient under local anesthesia
- Cure rate 92-98%
- Simultaneous diagnostic + therapeutic ("see and treat" approach acceptable in high-risk patients)
- ECC can be performed simultaneously
Complications (from pooled data - Berek & Novak):
| Complication | Rate |
|---|---|
| Operative hemorrhage | 0.001% |
| Post-operative hemorrhage | 1.8% |
| Cervical stenosis | 0.6% |
| Infection | Rare |
| Preterm birth in future pregnancies | OR 1.37 |
Margin Involvement: Positive margins predict recurrence (23.6% with gland involvement vs. 11.3% without). Margin positivity does not mandate immediate re-treatment - co-testing at 4-6 months is acceptable.
RCT evidence 2025 (PMID 40673798): General vs. local anesthesia in LEEP shows equivalent oncologic outcomes; local anesthesia remains standard for outpatient settings.
7b. Cold Knife Conization (CKC)
Best margins; preferred for AIS, suspected microinvasion, and recurrent CIN
Indications:
- AIS (adenocarcinoma in situ)
- Suspected stage IA1 microinvasion
- Recurrent CIN after LEEP
- TZ 3 with high-grade pathology
- Discordant cytology-histology (very high cytologic grade)
- Positive ECC with high-grade histology
Key data: Treatment failure OR 0.63 vs. LEEP, but preterm birth OR 2.27 - highest reproductive morbidity of all excisional techniques. (Lancet Oncol, Athanasiou 2022)
7c. Laser Conization
- Failure rate lower than LEEP (OR 0.59 vs. LEEP)
- Preterm birth OR 1.77 vs. untreated
- Limited availability; best for large lesions where precise depth control matters
- Can combine with laser ablation of edges for broader TZ coverage
7d. Cryotherapy
- WHO recommends for LMIC settings (screen-and-treat programs)
- Effective for small ectocervical lesions covering <75% of ectocervix
- Requires 2 freeze-thaw cycles (3 min / 5 min / 3 min)
- Failure rate significantly higher than LEEP (OR 1.84)
- Not recommended for CIN 3, large lesions, or TZ extending into canal
7e. CO₂ Laser Ablation
- Cure rate 90-95% for CIN 2/3
- Higher failure rate than LEEP (OR 1.69) and both conization techniques
- Maintains fertility potential (no preterm birth increase)
- Best reserved for selected small CIN 2 in women desiring future pregnancy who meet all ablation criteria
7f. Cold Coagulation (Semm)
- Thermal probe at 100-120°C for 20-30 seconds
- Network meta-analysis shows no significant difference vs. LEEP (OR 1.09, CI 0.68-1.74)
- No preterm birth increase
- Limited RCT data (only 2 small studies)
- Widely used in UK; cheap; outpatient
7g. Hysterectomy
Role is limited and should be last resort:
Appropriate indications only:
- Histologically confirmed recurrent high-grade CIN after multiple excisions
- AIS with positive cone margins and completed childbearing
- Microinvasion (FIGO stage IA1 without LVSI - simple hysterectomy)
- Co-occurring gynecologic pathology requiring hysterectomy (fibroids, prolapse, endometriosis)
"Hysterectomy is the treatment of last resort for recurrent high-grade CIN." - Berek & Novak's Gynecology, p. 865
8. SPECIAL POPULATIONS
Table 4: Modified Management in Special Populations
| Population | CIN 1 | CIN 2 | CIN 3 | Key Principle |
|---|---|---|---|---|
| Age 21-24 | Cytology at 12 mo (no HPV testing) | Observation x24 months acceptable | Treat | High spontaneous regression; avoid overtreatment |
| Age ≥ 25 | Observe; treat if persists ≥ 2 yr | Treat OR observe if concerns | Treat | Standard management |
| Pregnancy | Observe | Defer to postpartum (repeat q12 wks in pregnancy) | Defer to postpartum (unless invasion suspected) | 70% CIN 2 regresses postpartum |
| Immunocompromised (HIV, transplant) | Lower threshold to treat | Treat | Treat aggressively; margin-free excision | Higher progression risk; lower regression rate |
| Postmenopausal | HPV co-test preferred; intravaginal estrogen before colposcopy aids visualization | Treat | Treat; ECC mandatory | Endocervical assessment critical |
| Desire for future pregnancy | Observe | Prefer ablation or minimal LEEP if treatment needed | Smallest excision adequate; prefer laser/ablation if criteria met | Balance oncologic control vs. obstetric risk |
9. POST-TREATMENT SURVEILLANCE
Table 5: Post-Treatment Follow-Up Protocol
| Time Point | Test | Action if Abnormal |
|---|---|---|
| 4-6 months post-treatment | HPV co-test (cytology + HR-HPV) | ≥ ASC or HPV+ → Colposcopy |
| 12 months post-treatment | HPV co-test | ≥ ASC or HPV+ → Colposcopy |
| If both negative | Annual HPV co-test | Continue for 3 consecutive years then step down |
| After 3 negative co-tests | Co-test every 3 years for ≥ 20 years | Continue regardless of age at time of treatment |
| Persistent HPV positivity | Colposcopy + ECC | Re-excision vs. intensive surveillance |
Predictors of Post-Treatment Failure (Systematic Review, Bomans et al. 2025, PMID 40638922):
- Positive surgical margins (most significant)
- Persistent HR-HPV post-treatment (especially HPV 16/18)
- Endocervical gland involvement
- CIN 3 (vs. CIN 2)
- Immunosuppression
Risk-stratified surveillance after LEEP (Nomogram 2026, PMID 41853302): Integrates HPV persistence, margin status, and clinical factors to individualize CIN 2+ recurrence prediction - moving toward personalized follow-up.
10. EMERGING AND ADJUNCTIVE THERAPIES
Table 6: Emerging Treatment Options
| Modality | Evidence Level | Status | Notes |
|---|---|---|---|
| Adjuvant HPV vaccination | Meta-analysis (PMID 40919695; 41821885) | Recommended (ASCCP Dec 2025) | 9-valent vaccine post-excision reduces recurrence; offer to unvaccinated patients at time of treatment. Most benefit in HPV 16/18-negative residual infection |
| Imiquimod 5% (topical) | Phase II RCT (PMID 38592381) | Investigational | Imiquimod ± HPV vaccine: complete histologic regression in subset of CIN 2/3; not standard care |
| Photodynamic Therapy (PDT) | RCT 2026 (PMID 41453715) | Investigational | 5-ALA PDT vs. Hiporfin PDT for HPV+ CIN 2: comparable efficacy; used in some Asian centers |
| Topical 5-Fluorouracil | Pilot trial (PMID 38168442) | Investigational in PLHIV | Post-LEEP intravaginal 5-FU in HIV+ women in Kenya; phase II ongoing |
| DNA methylation triage | Systematic review (PMID 37533074) | Emerging triage biomarker | Methylation markers (FAM19A4, miR124-2) may replace cytology in HPV+ triage |
11. 2024-2025 BIOMARKER ADVANCES: TRIAGE & RISK STRATIFICATION
Table 7: Molecular Markers in CIN Management
| Marker | Test | Role | Evidence |
|---|---|---|---|
| HR-HPV genotyping | Extended genotyping (HPV 16/18 vs. 31/33/45/52/58) | Risk stratification for immediate action vs. surveillance | ASCCP 2025 guideline (PMID 39791481) |
| p16/Ki-67 Dual Stain | Dual stain (DS) on liquid cytology | Triage HPV+ women; DS+ → colposcopy; DS- → 1-year repeat | ASCCP April 2024 guideline; higher specificity than cytology |
| HPV E6/E7 oncoprotein | Protein-based test | Higher specificity for high-grade CIN vs. DNA; meta-analysis accuracy (PMID 37973957) | Emerging, not yet in routine guidelines |
| DNA methylation | FAM19A4/miR124-2 | Triage hr-HPV+ women to reduce unnecessary colposcopy | Systematic review (PMID 37533074) - sensitivity 70-80%; specificity 60-75% |
| p16 IHC (histology) | Immunohistochemistry on biopsy | Resolves CIN 2 vs. reactive changes; positive in true CIN 2/3 | Standard pathology adjunct; helps distinguish CIN 2 mimics |
12. ADENOCARCINOMA IN SITU (AIS) - SPECIAL CONSIDERATION
AIS management differs fundamentally from squamous CIN:
| Principle | Recommendation |
|---|---|
| Primary treatment | CKC with clear margins (LEEP insufficient - skip lesions) |
| Margin positive | Re-excision to achieve clear margins |
| Fertility desired + clear margins | Conservative management with close surveillance acceptable |
| Fertility completed or margins unachievable | Hysterectomy recommended |
| HPV type | HPV 18 predominant in AIS (unlike HPV 16 in squamous) |
| ECC | Mandatory in all cases |
13. SUMMARY MANAGEMENT TABLE
Table 8: At-a-Glance Management by Grade, Setting, and Special Circumstance
| Clinical Scenario | First-Line Management | Acceptable Alternative | When to Escalate |
|---|---|---|---|
| CIN 1, colposcopy satisfactory | Surveillance (HPV co-test at 12 mo) | Ablation if persistent ≥ 2 yr | CIN 2+ on re-biopsy |
| CIN 1, post-HSIL cytology | Review all material; consider excision | Observation with repeat in 6 mo | Any HSIL recurrence |
| CIN 2, age ≥ 25, completed childbearing | LEEP/LLETZ | CKC if ECC+ | Recurrence → re-excision |
| CIN 2, age 21-24 | Observation x24 mo (cytology q6 mo) | LEEP if persistent >24 mo | CIN 3 found on biopsy |
| CIN 2, pregnancy | Observation to postpartum | - | If invasion suspected |
| CIN 3, any age ≥ 25 | LEEP/LLETZ | CKC (for endocervical/large lesion) | Microinvasion on LEEP → CKC/radical |
| CIN 3, satisfactory colposcopy | LEEP preferred; ablation acceptable | Laser conization | Recurrence after two excisions → hysterectomy |
| CIN 3, unsatisfactory colposcopy | CKC | Laser conization | Microinvasion → FIGO staging |
| Recurrent CIN 2/3 after LEEP | CKC | Laser conization | Second recurrence → hysterectomy |
| AIS, fertility desired | CKC with clear margins | - | Positive margins → re-CKC |
| AIS, completed fertility | Hysterectomy (simple) | CKC + close surveillance if margins clear | Invasive adenocarcinoma → radical |
| Microinvasion IA1, no LVSI | Simple/extrafascial hysterectomy | Fertility-sparing: CKC with margins | IA1 with LVSI → modified radical |
14. KEY CLINICAL PEARLS FOR THE GYNECOLOGIC ONCOLOGIST
-
"See and treat" is acceptable for HSIL cytology with colposcopic impression of CIN 2/3 in non-pregnant women - reduces loss to follow-up but risks overtreatment.
-
Margin status alone should not mandate immediate re-treatment after LEEP. HPV co-testing at 4-6 months is the preferred first step; colposcopy if co-test positive.
-
CIN 2 is a heterogeneous category: p16 IHC helps distinguish true high-grade lesion (CIN 3-equivalent) from CIN 1 with sampling artifact. p16-negative CIN 2 has much higher regression rate.
-
Adjuvant HPV vaccination reduces recurrence after excisional treatment: meta-analysis 2026 (PMID 41821885) confirms benefit regardless of timing (pre- or post-surgery) and vaccine valency, particularly for 9-valent vaccine. ASCCP formally recommends it (December 2025).
-
Extended genotyping changes management: HPV 16 + HSIL cytology now warrants "treatment preferred" without waiting for colposcopy biopsy confirmation (ASCCP 2025).
-
HPV persistence after treatment is the strongest recurrence predictor: HR-HPV positive at 6 months post-LEEP predicts CIN 2+ recurrence better than margin status.
-
Cryotherapy is NOT appropriate for: TZ 3, lesion >75% ectocervix, ECC positive, prior treatment failure, any CIN 3 extending to os, or AIS.
-
Long-term follow-up is mandatory: Women treated for CIN 2/3 have elevated cervical cancer risk for ≥20 years compared to the general population - co-testing for at least 20 years post-treatment is recommended.
-
LEEP in a future pregnancy: Preterm birth risk is dose-dependent on cone depth. Depth <10 mm has minimal risk; depth >20 mm significantly increases preterm birth rate.
-
Dual Stain (p16/Ki-67): HPV+ / DS- women can safely return to 1-year repeat HPV testing instead of immediate colposcopy, reducing unnecessary procedures by up to 40%.
Sources & Evidence Base
- Berek & Novak's Gynecology (p. 832-870) - Comprehensive CIN chapter
- Creasy & Resnik's Maternal-Fetal Medicine (p. 1351) - CIN in pregnancy
- Pfenninger & Fowler's Procedures for Primary Care - Histologic management algorithms
- Athanasiou et al., Lancet Oncol 2022 (PMID 35835138) - Network meta-analysis, 19,240 patients: comparative treatment failure and preterm birth rates
- Massad et al., J Low Genit Tract Dis 2025 (PMID 39791481) - ASCCP Extended Genotyping Enduring Guidelines
- Maiorano et al., Front Oncol 2026 (PMID 41821885) - HPV vaccine post-conization, meta-analysis
- Kapp et al., Cochrane 2025 (PMID 40919695) - Cochrane review: HPV vaccination post-conization
- Bomans et al., Obstet Gynecol 2025 (PMID 40638922) - Predictors of treatment failure post-excision, meta-analysis
- Reuschenbach et al., Eur J Obstet Gynecol 2024 (PMID 39002399) - Treatment characteristics and subsequent disease in high-grade CIN, European systematic review
- Sheth et al., Clin Cancer Res 2024 (PMID 38592381) - Phase II RCT: Imiquimod ± HPV vaccine for CIN 2/3
- ASCCP 2019 Risk-Based Management Consensus Guidelines (updated through 2025)
- USPSTF 2024 Draft Recommendation: Primary HPV screening preferred age 30-65
This is a shared conversation. Sign in to Orris to start your own chat.