Write down pathophysiology and management of ARDS / Patient with fever, breathlessness, hypoxia - causes and management of ARDS ⭐⭐⭐
Reading File
Finding Sources
Searching PubMed
"acute respiratory distress syndrome" AND management
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information from Harrison's, Fishman's, and Murray & Nadel's. Let me compile the complete, detailed answer.
Acute Respiratory Distress Syndrome (ARDS)
Pathophysiology and Management
DEFINITION AND DIAGNOSIS (Berlin Criteria 2012)
ARDS is a clinical syndrome of acute, severe hypoxemia with bilateral pulmonary infiltrates, not fully explained by cardiac failure or fluid overload. It is classified by PaO₂/FiO₂ (P/F ratio) measured on at least 5 cmH₂O PEEP:
| Severity | P/F Ratio | Mortality |
|---|---|---|
| Mild | 200-300 mmHg | ~27% |
| Moderate | 100-200 mmHg | ~32% |
| Severe | <100 mmHg | ~45% |
Additional criteria:
- Onset: Within 1 week of a known clinical insult or new/worsening respiratory symptoms
- Chest imaging: Bilateral opacities not fully explained by effusions, lobar collapse, or nodules
- Origin of edema: Not primarily from cardiac failure or fluid overload
2024 Global Definition Update: The new global definition (Matthay MA et al., AJRCCM 2024) allows SpO₂/FiO₂ ≤315 mmHg as a substitute for P/F ratio, and permits diagnosis in non-intubated patients on high-flow nasal oxygen (≥30 L/min) or NIV/CPAP. This broadens ARDS recognition to resource-limited settings.
CAUSES (ARDS Risk Factors)
Patient with Fever + Breathlessness + Hypoxia → Think ARDS
Direct Lung Injury (Pulmonary)
- Pneumonia (bacterial, viral, fungal) - most common
- Aspiration of gastric contents
- Pulmonary contusion / trauma
- Inhalation injury (smoke, toxic gases)
- Near-drowning
- Reperfusion injury post lung transplant
Indirect Lung Injury (Extrapulmonary)
- Sepsis (most common overall cause - 40%)
- Severe trauma / non-thoracic
- Multiple blood transfusions (TRALI)
- Pancreatitis
- Burns
- Drug overdose
- Cardiopulmonary bypass
Clinical pearl: In a patient with fever + breathlessness + hypoxia, the triad points to either sepsis-induced ARDS or infectious pneumonia-induced ARDS as the most likely cause.
PATHOPHYSIOLOGY
ARDS evolves in three overlapping phases:
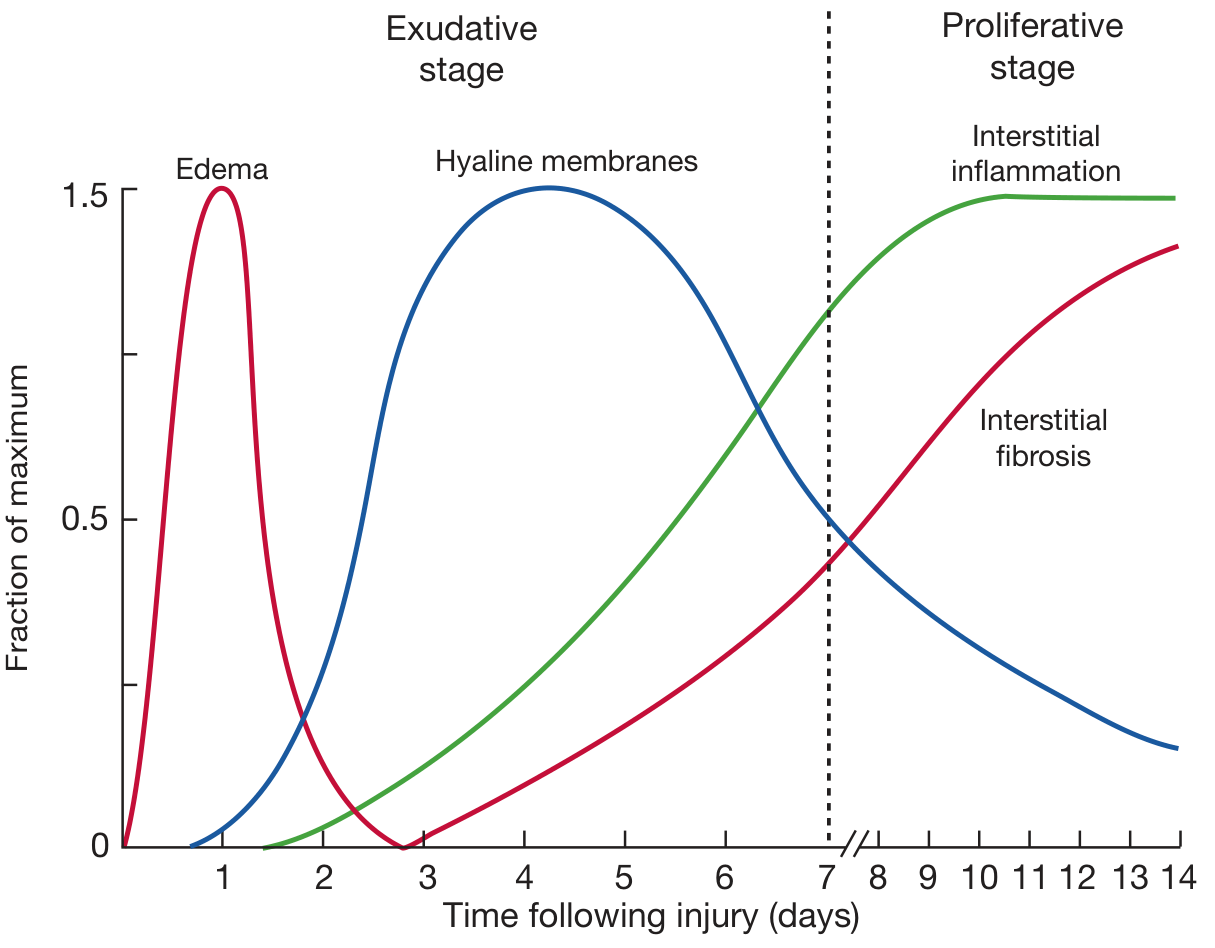
Phase 1: Exudative Phase (Days 1-7)
Initiating trigger (sepsis, pneumonia, aspiration, etc.)
↓
Alveolar-capillary barrier disruption
The core mechanism is increased permeability of the alveolar-capillary membrane, not hydrostatic pressure (unlike cardiogenic pulmonary edema):
-
Endothelial injury: Activated neutrophils release proteases, reactive oxygen species (ROS), and pro-inflammatory cytokines (IL-1, IL-6, IL-8, TNF-α) that damage capillary endothelial cells and widen intercellular junctions.
-
Epithelial injury: Type I pneumocytes (which cover ~95% of alveolar surface) are destroyed. This denudes the alveolar basement membrane.
-
Protein-rich edema floods alveoli: Loss of the tight epithelial barrier allows protein-rich fluid to pour into alveolar spaces. Condensed plasma proteins + cellular debris + dysfunctional surfactant = hyaline membrane formation.
-
Surfactant dysfunction: Surfactant is washed out and inactivated. Loss of surfactant causes alveolar collapse (atelectasis). This raises surface tension and further worsens compliance.
-
Neutrophil influx: Massive neutrophil recruitment into the interstitium and alveoli. Neutrophils release elastase, collagenase, and more ROS, amplifying injury.
-
Pulmonary vascular injury: Microthrombi form in pulmonary vasculature; vascular obliteration causes pulmonary hypertension.
Physiologic consequences:
- V/Q mismatch and intrapulmonary shunting → refractory hypoxemia (fails to correct with supplemental O₂ alone)
- Reduced lung compliance (stiff lungs = increased work of breathing)
- Increased dead space → hypercapnia in severe cases
- Right-to-left shunting dominates
Phase 2: Proliferative Phase (Days 7-14)
- Type II pneumocytes proliferate along denuded alveolar basement membranes - they synthesize new surfactant and differentiate into Type I cells
- Hyaline membranes begin to be reorganized
- Shift from neutrophil-predominant to lymphocyte-predominant infiltrate
- Fibroblast and myofibroblast proliferation begins
- Collagen deposition starts (elevated BAL N-terminal procollagen peptide III detectable as early as 24h)
- Many patients begin improving in this phase
Phase 3: Fibrotic Phase (>14-21 days, some patients)
- Alveolar and interstitial fibrosis replaces the inflammatory exudate
- Emphysema-like changes with large bullae form
- Intimal fibroproliferation in microcirculation → progressive pulmonary hypertension
- Increased pneumothorax risk (poor compliance + bullae)
- Associated with significantly increased mortality
Diffuse Alveolar Damage (DAD) is the pathologic hallmark - but found on autopsy in only ~45-50% of clinical ARDS cases, confirming pathologic heterogeneity.
MANAGEMENT
A. Treat the Underlying Cause
This is the most important first step - ARDS is a syndrome, not a diagnosis:
- Cultures + broad-spectrum antibiotics for suspected sepsis/pneumonia
- Source control (drain abscess, manage peritonitis)
- Treat aspiration, pancreatitis, etc.
B. Lung-Protective Ventilation (ARDSNet Protocol) - Grade A evidence
The cornerstone of ARDS management. Prevents ventilator-induced lung injury (VILI):
| VILI Mechanism | Problem | Solution |
|---|---|---|
| Volutrauma | Alveolar overdistension from large tidal volumes | Low TV |
| Barotrauma | Excess plateau pressure | Keep Pplat <30 cmH₂O |
| Atelectrauma | Repeated alveolar collapse/re-opening | Adequate PEEP |
| Biotrauma | Cytokine release from injured lung | Low TV strategy reduces cytokines |
ARDSNet parameters:
- Tidal volume (TV): 6 mL/kg of predicted body weight (not actual)
- Plateau pressure: ≤30 cmH₂O
- Driving pressure (Pplat - PEEP): Target <15 cmH₂O - associated with improved survival
- PEEP: Titrated to maintain alveolar recruitment - use the ARDSNet high-PEEP/FiO₂ table
- FiO₂: Minimum needed to achieve SpO₂ 92-96% (avoid hyperoxia)
- Rate: Can increase up to 35 breaths/min to allow permissive hypercapnia
Permissive hypercapnia: Allow PaCO₂ to rise (pH ≥7.20) to keep TV low - acceptable trade-off.
C. Prone Positioning - Grade B evidence (mortality benefit in severe ARDS)
- Indicated when P/F ratio <150 mmHg despite lung-protective ventilation
- Recommendation: ≥16 hours/day prone sessions (PROSEVA trial: Guerin et al., NEJM 2013)
- Mechanism: Redistributes alveolar edema, recruits dorsal lung segments, reduces V/Q mismatch, decreases atelectrauma
- Mortality benefit: ~50% reduction in 28-day mortality in severe ARDS
D. Fluid Management - Conservative strategy (Grade B)
- ARDS patients: Use a conservative fluid strategy to minimize further pulmonary edema
- Target: Lowest left atrial filling pressure compatible with adequate organ perfusion
- FACTT trial: Conservative fluids = more ventilator-free days (no survival difference, but improved lung function)
- Use vasopressors for shock rather than fluid loading once euvolemia is achieved
E. PEEP Optimization
- Adequate PEEP keeps alveoli open at end-expiration (prevents atelectrauma)
- Higher PEEP may worsen hemodynamics (reduces venous return)
- No single optimal PEEP strategy proven; ARDSNet PEEP/FiO₂ tables are widely used
- "Open lung" approach: Recruit with higher PEEP, but LOCO2/ART trials showed high-PEEP recruitment maneuvers may increase mortality - so routine aggressive recruitment is no longer recommended
F. Neuromuscular Blockade (NMB) - Grade C (selective use)
- Cisatracurium infusion (48h) in severe ARDS (P/F <150) was shown to reduce mortality in the ACURASYS trial
- However, the larger ROSE trial (NEJM 2019) showed NO mortality benefit from routine early NMB
- Current recommendation: Use NMB for patient-ventilator dyssynchrony or severe refractory hypoxemia - not routinely
G. Extracorporeal Membrane Oxygenation (ECMO) - Grade B (select patients)
- Indicated for severe refractory ARDS (P/F <80 despite optimized ventilation + prone)
- Veno-venous (VV) ECMO: Provides gas exchange while resting injured lungs
- CESAR trial and EOLIA trial showed potential benefit in severe ARDS at expert centers
- Allows "ultra-protective" ventilation (TV 3-4 mL/kg)
H. Glucocorticoids - Grade D (not routinely recommended)
- Multiple trials failed to show consistent mortality benefit
- Current evidence does NOT support routine glucocorticoids in ARDS
- Exception: Low-dose hydrocortisone 200 mg/24h may be considered in:
- Septic shock refractory to vasopressors
- Severe CAP with ARDS
- 2024 meta-analysis (Soumare et al., Ann Intern Med 2026, PMID 41325621): Confirms corticosteroids in pneumonia + ARDS may reduce mortality but increase infection risk - careful patient selection required
I. Other Therapies (NOT proven to improve survival)
| Therapy | Evidence |
|---|---|
| Inhaled nitric oxide | Improves oxygenation transiently, no mortality benefit |
| Inhaled prostacyclin (epoprostenol) | Same - transient oxygenation improvement only |
| Surfactant replacement | Disappointing in adults (unlike neonates) |
| High-frequency oscillatory ventilation (HFOV) | NOT recommended (OSCAR/OSCILLATE trials showed harm) |
| Ketoconazole, PGE₂, NSAIDs | Not recommended |
J. Supportive ICU Care (General Principles)
- VTE prophylaxis: LMWH + sequential compression devices
- GI prophylaxis: PPI or H2-blocker
- Enteral nutrition: Early (within 24-48h) via nasogastric tube - preferred over parenteral
- Glucose control: Target 140-180 mg/dL (avoid tight control)
- Sedation: Minimize (daily sedation interruption); avoid prolonged deep sedation
- Head-of-bed elevation: 30-45° to reduce aspiration
- Infection surveillance: Regular cultures, early de-escalation of antibiotics
- Delirium prevention: Minimize benzodiazepines, early mobilization
SUMMARY TABLE: Evidence-Based ARDS Therapies
| Treatment | Evidence Grade | Key Point |
|---|---|---|
| Low tidal volume (6 mL/kg PBW) | A | Reduces mortality - core therapy |
| Conservative fluid management | B | More ventilator-free days |
| Prone positioning (>16h/day) | B | Mortality benefit in P/F <150 |
| High PEEP/open lung | B | Benefit depends on recruitability |
| ECMO (severe refractory) | B | Expert centers only |
| Neuromuscular blockade | C | Selective use only (dyssynchrony) |
| Inhaled vasodilators | C | Temporary oxygenation bridge only |
| Glucocorticoids | D | Not routine; limited specific indications |
| HFOV | D | Avoid - shown to be harmful |
| Surfactant | D | Not recommended in adults |
OUTCOMES
- Mortality has fallen from >60% (1980s) to <40% currently
- Most survivors recover near-normal lung function by 6-12 months
- However, significant long-term morbidity remains:
- ICU-acquired weakness (myopathy/axonopathy from proteolysis)
- Cognitive impairment (attention, memory, processing speed)
- PTSD and mood disorders
- Reduced 6-minute walk distance for years post-discharge
Sources: Harrison's Principles of Internal Medicine 22E (2025); Murray & Nadel's Textbook of Respiratory Medicine; Fishman's Pulmonary Diseases and Disorders; PMID 41325621 (Soumare et al., Ann Intern Med 2026 - corticosteroids in ARDS)
This is a shared conversation. Sign in to Orris to start your own chat.