Neuropathic pain detail and mangement in ED and OPd basis as per NICE guidelines and also include standard textbooks
Reading File
Finding Sources
Searching the Web
NICE guidelines neuropathic pain management 2023 2024 NG173
Searching PubMed
"neuropathic pain" AND management
Reading File
Reading File
Reading File
Reading Web Page
neuropathic pain pharmacological management first line second line drugs dosing
Reading File
Finding Sources
Reading Web Page
NICE CG173 neuropathic pain first line second line drugs recommendations amitriptyline duloxetine gabapentin pregabalin
Reading File
Loading Image
Reading File
I now have all the essential information. Let me compose the comprehensive answer.
Neuropathic Pain: Definition, Pathophysiology, and Management
1. Definition and Diagnostic Criteria
Neuropathic pain is defined by the IASP as "pain caused by a lesion or disease of the somatosensory nervous system." It differs fundamentally from nociceptive pain: standard analgesics (paracetamol, NSAIDs) provide little to no benefit, and the underlying mechanism involves maladaptive changes in peripheral and central pain-processing pathways.
Harrison's Principles of Internal Medicine 22e, p. 937: "Damage to or dysfunction of nociceptive pathways can produce pain referred to the body region innervated by the damaged nerves... such pains are termed neuropathic and are often severe and resistant to standard treatments."
2. Pathophysiology
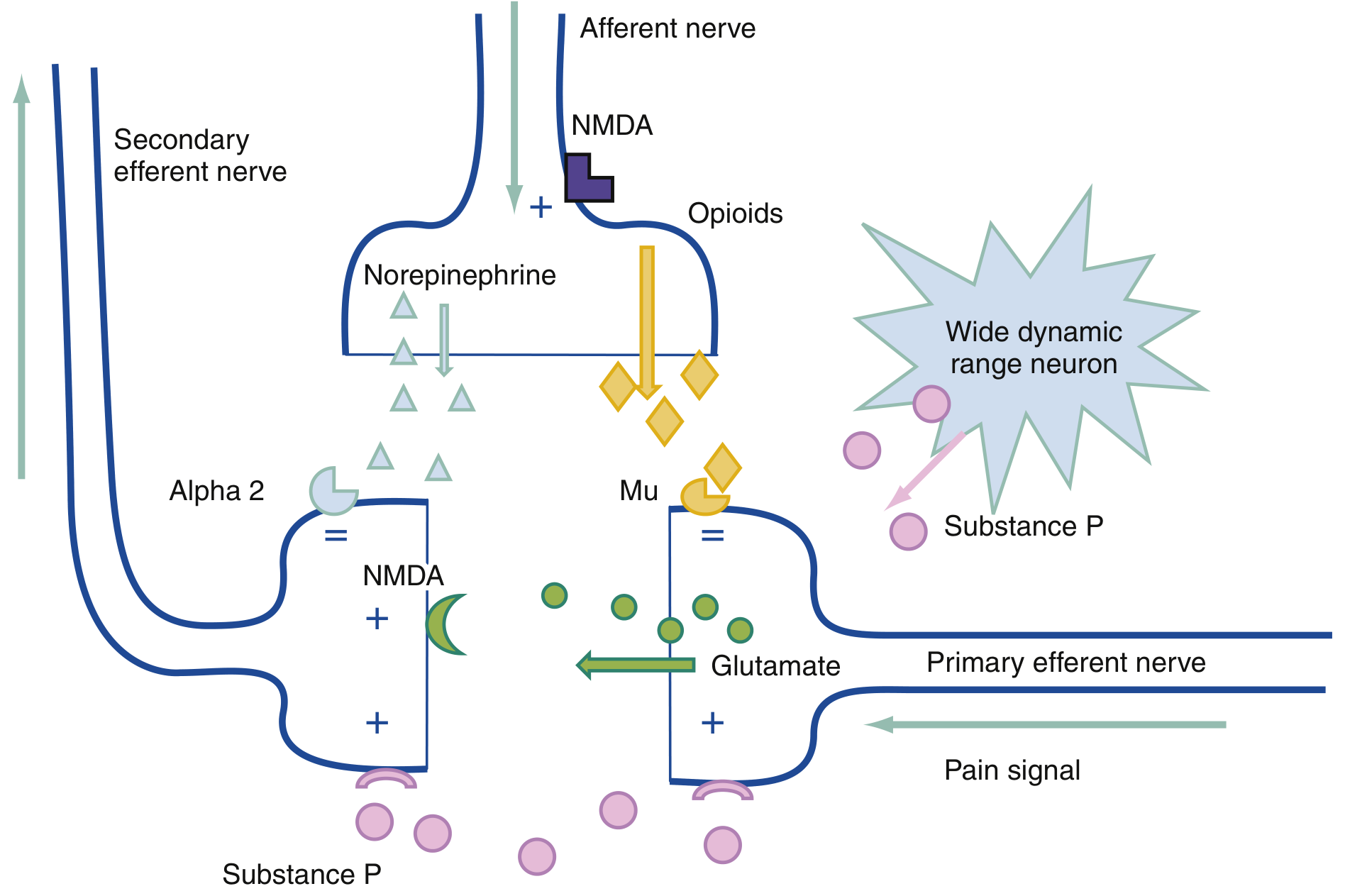
Key mechanisms include:
| Mechanism | Details |
|---|---|
| Peripheral sensitization | Damaged primary afferents become hyperexcitable; increased sodium channel density drives spontaneous firing |
| Central sensitization | Spinal cord neurons cut off from normal input become spontaneously active; wide dynamic range neuron hyperactivity |
| Ectopic discharge | Injured axons fire without a stimulus (spontaneous pain) |
| Sympathetically maintained pain | Damaged primary afferents acquire adrenergic sensitivity (basis of CRPS) |
| Glial activation | Increased prostaglandins, cytokines; structural remodeling of dorsal horn connections |
| Thalamocortical dysrhythmia | Brain-level plastic reorganization perpetuating chronic pain |
(Harrison's 22e, p. 942-943; Bradley and Daroff's Neurology in Clinical Practice, p. 729)
3. Clinical Features
Typical descriptors of neuropathic pain:
- Burning, tingling, electric-shock-like, stabbing, lancinating
- Spontaneous pain - occurs without any stimulus
- Allodynia - light touch evokes exquisite pain
- Hyperalgesia/Hyperpathia - exaggerated pain response to nociceptive stimuli
- Sensory deficit co-extensive with the pain area on examination
Common causes:
- Diabetic peripheral neuropathy
- Postherpetic neuralgia (PHN)
- Trigeminal neuralgia
- Post-stroke central pain
- Spinal cord injury pain
- HIV neuropathy
- Post-surgical/phantom limb pain
- CRPS (type I and II)
- Radiculopathy
4. Assessment Tools
- Numeric Rating Scale (NRS) or Visual Analogue Scale (VAS) for pain severity
- DN4 questionnaire (Douleur Neuropathique 4 questions) - validated screening tool, score ≥4/10 suggests neuropathic pain
- LANSS scale (Leeds Assessment of Neuropathic Symptoms and Signs)
- PainDETECT for screening
- Neurological examination: test for allodynia, hyperalgesia, and sensory deficits in the affected territory
5. NICE CG173 Recommendations (Non-specialist Settings, Adults)
Key Principles of Care (NICE 1.1.1)
When agreeing a treatment plan, discuss:
- Severity of pain and its impact on lifestyle, sleep, daily activities
- The underlying cause and whether it has deteriorated
- Why a particular pharmacological treatment is being offered
- The realistic expectation that treatment achieves partial (30-50%) not complete relief
Monitoring (NICE 1.1.6)
Regular clinical review with attention to:
- Pain severity, lifestyle impact
- Treatment effectiveness and tolerability
- Need for referral
Specialist Referral (NICE 1.1.2)
Refer to specialist pain service if:
- Severe pain
- Pain significantly limits lifestyle, daily activities, sleep
- Underlying condition has deteriorated
6. Pharmacological Management: Step-by-Step
First-Line Treatment (NICE CG173 Recommendation 1.1.8)
Offer a choice of 4 drugs as initial treatment (except trigeminal neuralgia):
| Drug | Typical Dose | Notes |
|---|---|---|
| Amitriptyline (TCA) | Start 10-25 mg nocte; titrate to 75-150 mg/day | Proven in PDN and PHN; fewer anticholinergic effects with nortriptyline/desipramine |
| Duloxetine (SNRI) | 30-60 mg/day; up to 120 mg/day | Dual reuptake inhibitor; first-line in diabetic neuropathy; fewer side effects than TCAs |
| Gabapentin (anticonvulsant) | Start 300 mg/day; titrate to 1800-3600 mg/day in 3 divided doses | Alpha-2-delta calcium channel ligand; effective for PHN and PDN |
| Pregabalin (anticonvulsant) | 75-150 mg/day in divided doses; up to 600 mg/day | Same mechanism as gabapentin; more predictable bioavailability |
NICE CG173 Rec. 1.1.8; Bradley and Daroff's Neurology, p. 1808-1816
Titration principle: Start at the lowest dose, increase every 3-7 days to balance efficacy and tolerability. Many failures are due to under-dosing or excessively rapid titration.
If First Agent Fails (NICE 1.1.9)
Switch to any of the other 3 first-line agents. If the second also fails, try the remaining agents before concluding pharmacotherapy is ineffective.
Second-Line / Adjunct Options
| Drug | Notes |
|---|---|
| Tramadol | NICE 1.1.10: Consider for acute rescue therapy only - NOT for long-term use |
| Capsaicin cream (0.075%) | NICE 1.1.11: For localised neuropathic pain; patients who cannot tolerate oral drugs; depletes Substance P at peripheral terminals |
| Lidocaine 5% patch | Particularly effective for PHN with prominent allodynia (Harrison's 22e, p. 941); specialist use in UK |
| Opioids | Not first-line; reserved for specialist settings; RCTs show opioids do help neuropathic pain with comparable benefit to gabapentin/nortriptyline (Harrison's 22e) |
| Ketamine IV | NMDA antagonist; reduces central excitability; used in refractory cases in ED/specialist settings - no long-term oral formulation |
Trigeminal Neuralgia (NICE 1.1.13)
Carbamazepine is the first-line treatment (200-1600 mg/day in divided doses). Follow MHRA safety advice on antiepileptics in pregnancy.
Drugs NOT to Start in Non-Specialist Settings (NICE 1.1.12)
Do NOT initiate the following unless advised by a specialist:
- Cannabis sativa extract
- Capsaicin high-concentration patch (8%)
- Lacosamide
- Lamotrigine
- Levetiracetam
- Morphine
- Oxcarbazepine
- Topiramate
- Tramadol (long-term)
- Venlafaxine
- Valproate
7. Emergency Department (ED) Management
The ED approach focuses on acute neuropathic flares, new presentations, and pain crises rather than initiating long-term pharmacotherapy.
ED Assessment Framework (Rosen's Emergency Medicine 10e, p. 96)
- Characterize the pain - type, severity, distribution, associated sensory symptoms
- Identify red flags - new neurological deficits, cauda equina, cord compression, malignancy
- Do not delay analgesia - administration of adequate analgesia does not impair diagnostic accuracy and may improve the physical examination
ED Treatment Priorities
Acute rescue analgesia:
- Tramadol - NICE-endorsed for acute rescue therapy (Rec. 1.1.10)
- IV Lidocaine - beneficial in neuropathic pain; not long-lasting but useful in acute settings (Bradley and Daroff's, p. 1808)
- IV/IM Ketamine (sub-anaesthetic dose, 0.1-0.5 mg/kg) - NMDA antagonism reduces central sensitization; effective for acute refractory neuropathic pain
- Opioids - use cautiously for acute rescue when other options fail; not to be initiated for long-term management in ED
For trigeminal neuralgia flares:
- IV Phenytoin or IV Lidocaine as acute bridge
- Initiate/continue carbamazepine (NICE 1.1.13)
Avoid in ED:
- Initiating long-term opioids
- Starting complex pharmacotherapy without follow-up plan
- NSAIDs/paracetamol as sole agents (rarely effective)
ED Discharge Planning:
- Ensure clear outpatient follow-up (GP or pain clinic)
- Initiate or refer for one of the NICE first-line drugs (amitriptyline, duloxetine, gabapentin, pregabalin) if appropriate
- Document pain severity, impact, and the management plan shared with the patient
8. OPD (Outpatient) Long-Term Management
Non-Pharmacological Approaches
These are important adjuncts (NICE CG173 and NG193 Chronic Pain guideline):
- Physiotherapy - activity pacing, graded exercise
- Transcutaneous Electrical Nerve Stimulation (TENS)
- Cognitive Behavioural Therapy (CBT) - especially for chronic pain with mood impact
- Pain management programs - multidisciplinary
- Spinal cord stimulation - for CRPS and refractory neuropathic pain (specialist)
- Acupuncture - limited evidence; may be tried where standard treatments fail
OPD Follow-Up Protocol (NICE 1.1.5-1.1.7)
- Review at 2-4 weeks after starting a new treatment
- If response is adequate, agree a review schedule
- If inadequate at 2-4 weeks, titrate dose or switch agent
- At each review, reassess: pain severity, quality of life, sleep, ADLs, side effects
Special Populations in OPD
| Population | Consideration |
|---|---|
| Elderly | Start amitriptyline at lower dose (10 mg); anticholinergic risk; prefer nortriptyline/desipramine; gabapentinoids with caution (fall/sedation risk) |
| Renal impairment | Gabapentin and pregabalin are renally cleared; dose-reduce per eGFR |
| Cardiac disease | TCAs - caution in ischaemic heart disease; ECG before starting |
| Pregnancy | Avoid valproate, topiramate (MHRA); discuss risk-benefit for all agents |
| Diabetic neuropathy | Duloxetine and pregabalin are specifically approved/recommended |
Long-Term Monitoring Checklist (OPD)
- NRS/VAS at each visit
- Side effect review (sedation, weight gain with pregabalin, anticholinergic effects with TCAs, liver enzymes with duloxetine)
- Function and mood assessment
- Medication adherence
- Referral to specialist pain service if not responding after adequate trials of ≥2 first-line agents
9. Interventional Options (Specialist/Tertiary)
| Procedure | Indication |
|---|---|
| Spinal cord stimulation | CRPS, refractory PDN, post-surgical neuropathic pain |
| Dorsal root ganglion stimulation | Focal neuropathic pain syndromes |
| Intrathecal drug delivery | Refractory severe neuropathic pain |
| Sympathetic nerve blocks | CRPS (early phase) |
| DREZ (Dorsal Root Entry Zone) lesion | SCI-related neuropathic pain; 50-85% achieve relief |
| Capsaicin 8% patch | PHN and HIV neuropathy; specialist application |
(Barash's Clinical Anesthesia 9e; Bradley and Daroff's Neurology, p. 730)
10. Summary Algorithm
NEUROPATHIC PAIN PRESENTATION
|
ED Setting OPD Setting
| |
Exclude red flags Confirm diagnosis (DN4, exam)
(cord compression, etc.) |
| Initiate NICE first-line:
Acute rescue: Amitriptyline / Duloxetine /
Tramadol / IV Ketamine / Gabapentin / Pregabalin
IV Lidocaine |
| Review 2-4 weeks
Discharge with OPD Titrate or switch
follow-up plan (NICE 1.1.9)
|
If 2 agents fail → Refer to
Specialist Pain Service
(NICE 1.1.2)
11. Recent Evidence (2023-2025)
A landmark 2025 Lancet Neurology meta-analysis (Soliman et al., PMID 40252663) evaluated pharmacotherapy and non-invasive neuromodulation for neuropathic pain, confirming the effectiveness hierarchy of current first-line agents. A 2024 network meta-analysis in Health Technology Assessment (Birkinshaw et al., PMID 39367772) found duloxetine and other SNRIs/TCAs have proven benefit for chronic pain including neuropathic pain. A 2024 systematic review (Nwankwo et al., PMID 38949515) highlighted that gabapentin side effects (sedation, dizziness, peripheral edema, misuse potential) require careful monitoring, particularly in elderly patients.
Key Textbook Sources
- Harrison's Principles of Internal Medicine 22e (2025), p. 937-947
- Bradley and Daroff's Neurology in Clinical Practice, p. 1806-1820
- Rosen's Emergency Medicine 10e, p. 96
- Barash's Clinical Anesthesia 9e, p. 2583-2588
- Morgan and Mikhail's Clinical Anesthesiology 7e
- Rheumatology 2e (Elsevier 2022)
- NICE CG173 - Neuropathic pain in adults: pharmacological management in non-specialist settings (last reviewed Sept 2020)
This is a shared conversation. Sign in to Orris to start your own chat.