Indigestion, more burbs, left lower abdomen pain, what's the condition?
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a thorough breakdown based on your symptoms - indigestion, excessive burping (eructation), and left lower abdominal pain.
Most Likely Conditions
Your symptom combination points to several conditions across a spectrum from functional to structural. The key is whether alarm features (fever, weight loss, blood in stool) are present.
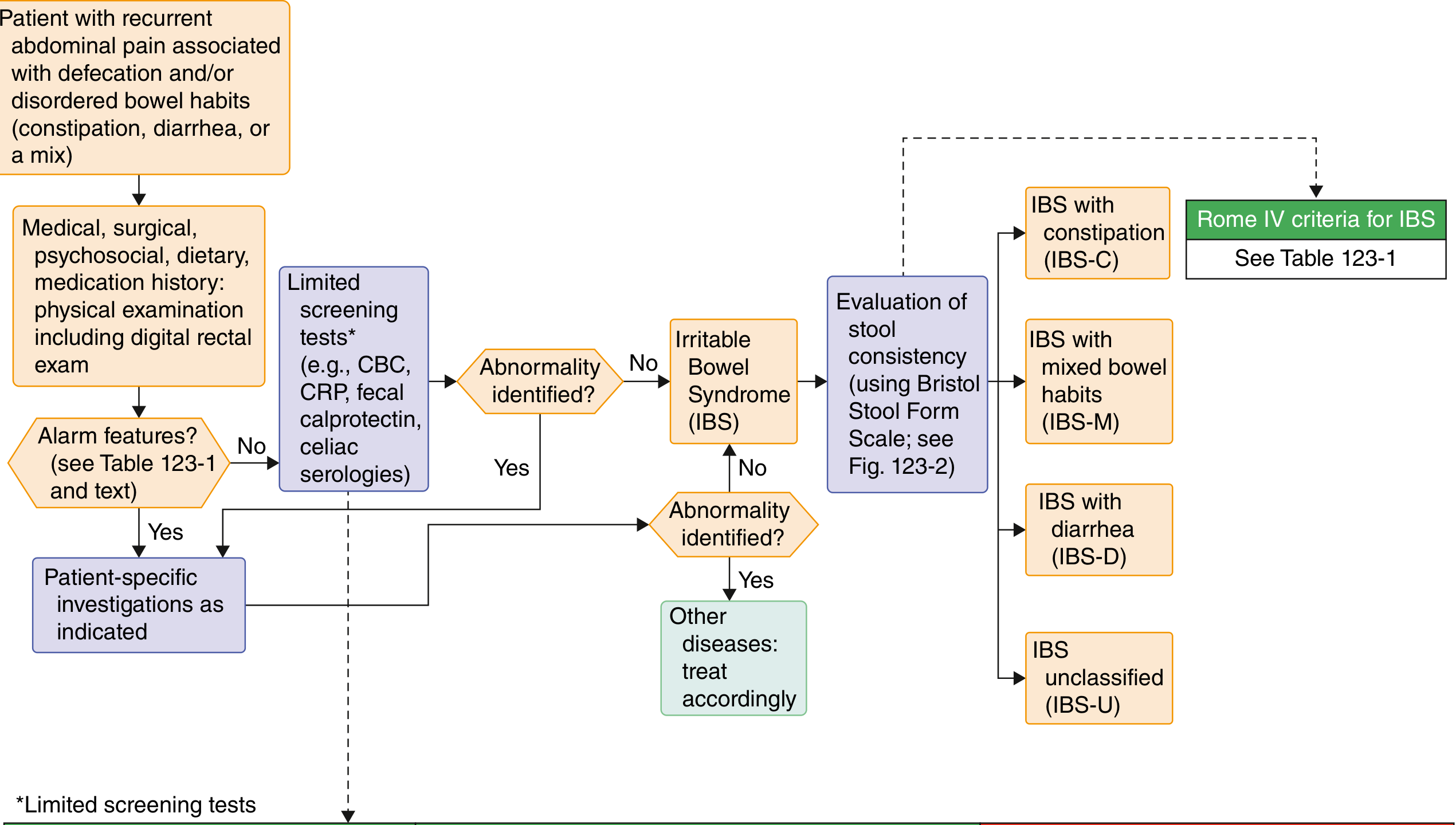
1. Irritable Bowel Syndrome (IBS) - Most Common Functional Cause
IBS is one of the most common GI disorders, affecting 10-15% of the population. It presents with recurrent abdominal pain (often lower abdomen) and altered bowel habits. Per the Rome III criteria, the diagnosis requires recurrent abdominal pain or discomfort for at least 3 days/month for 3 months, associated with two or more of:
- Improvement with defecation
- Onset associated with a change in stool frequency
- Onset associated with a change in stool appearance (constipation or diarrhea)
Belching and bloating are common co-symptoms in IBS, driven by gas accumulation and gut hypersensitivity. Triggers include stress, anxiety, antibiotics, certain foods (lactose, sorbitol, FODMAPs), and menstrual cycles.
2. Diverticulitis - Key Structural Cause (especially in adults over 40)
Diverticulitis classically causes left lower quadrant pain, fever, and altered bowel habits. From Yamada's Textbook of Gastroenterology:
"Acute sigmoid diverticulitis should be suspected in patients with the classic triad of left lower quadrant pain, fever, and leukocytosis."
Diverticulosis (pouches in the colon wall) can precede diverticulitis and may cause indigestion-like symptoms and bowel changes. The left lower quadrant location specifically points toward sigmoid colon involvement. CT scan is the diagnostic standard. Importantly, diverticulosis can follow a long history of IBS-like symptoms (bloating, constipation, diarrhea) before progressing.
3. Excessive Belching - The Gas Component
Per Goldman-Cecil Medicine:
"Belching (eructation)... is caused by swallowed air, which may be increased by eating quickly, drinking carbonated beverages, chewing gum, and smoking. Belching seldom reflects serious GI dysfunction but may be increased in patients with gastroesophageal reflux (GERD), functional dyspepsia, or gastroparesis."
Chronic, repetitive belching is also recognized as a functional disorder (supragastric belching) treated with behavioral modification.
4. Other Conditions to Consider
| Condition | Key Features |
|---|---|
| Functional dyspepsia | Indigestion + upper GI discomfort, often overlaps with IBS |
| Small intestinal bacterial overgrowth (SIBO) | Bloating, belching, abdominal discomfort, malabsorption |
| Lactose intolerance / FODMAP sensitivity | Gas, bloating, pain after certain foods |
| Inflammatory bowel disease (Crohn's/UC) | Lower abdominal pain + diarrhea, may have blood in stool |
| Colitis (infectious or ischemic) | Left lower quadrant pain, may have diarrhea/fever |
| Gynecological causes (if female) | Ovarian cyst, endometriosis - can mimic left lower quadrant pain |
Diagnostic Approach
The flowchart below (from Goldman-Cecil Medicine) guides workup for chronic abdominal pain:
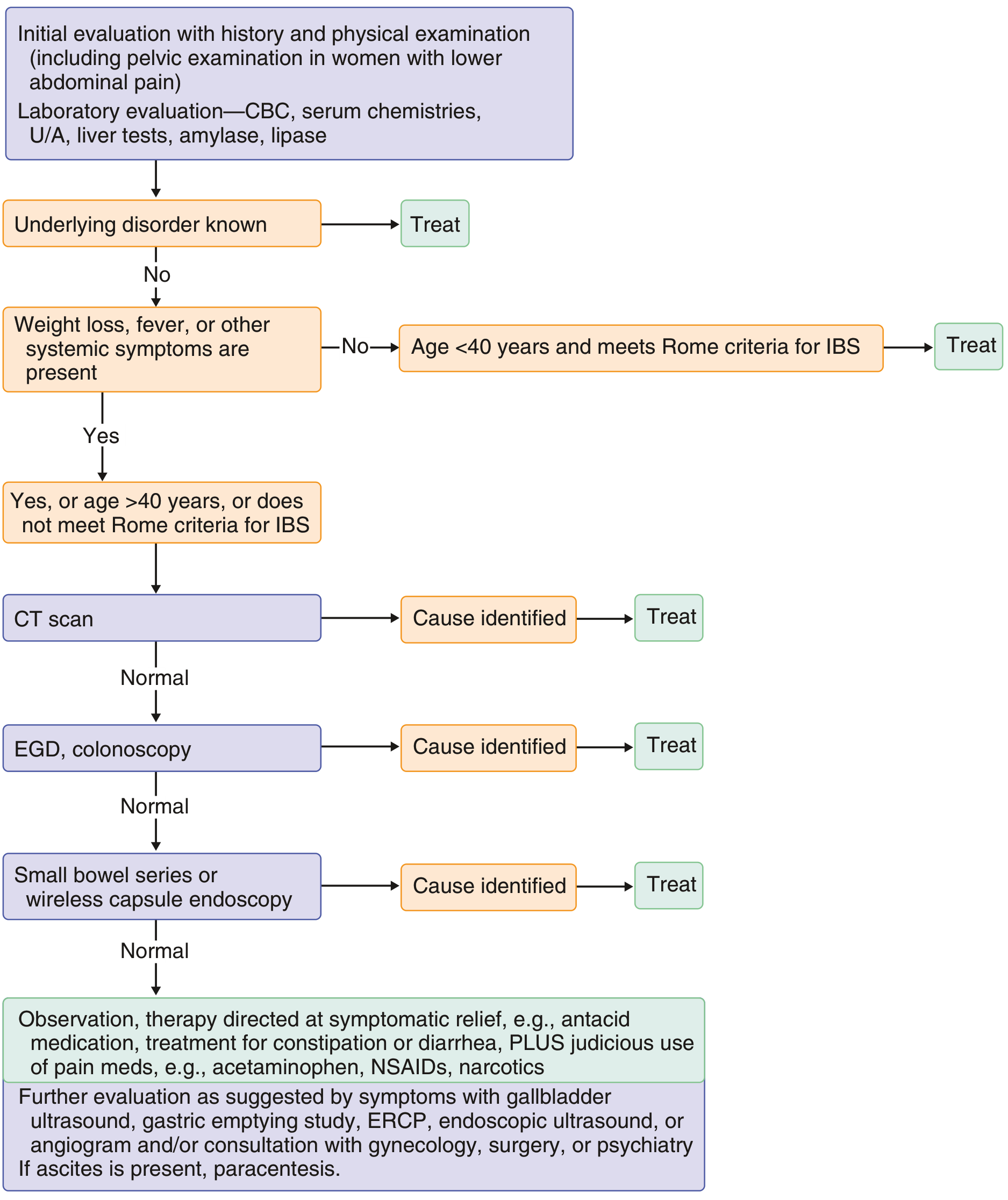
Key steps:
- Under 40, no alarm features - likely functional (IBS/dyspepsia), treat symptomatically
- Over 40, or alarm features present - CT scan first, then endoscopy (EGD/colonoscopy) if CT is normal
- Alarm features requiring urgent evaluation: fever, involuntary weight loss, rectal bleeding, nocturnal symptoms, progressive worsening
When to See a Doctor Urgently
Seek prompt medical attention if you have:
- Fever or chills alongside the abdominal pain (suggests diverticulitis or infection)
- Blood in stool
- Severe, worsening pain
- Vomiting with inability to keep food/fluids down
- Significant unintentional weight loss
Bottom line: The most likely diagnoses for your symptom triad are IBS (functional) or diverticulitis (structural, especially if you are over 40 and have fever). GERD/functional dyspepsia explains the burping. A doctor can differentiate these with a physical exam, blood work, and CT scan if needed.
Sources: Goldman-Cecil Medicine, p. 1368 | Washington Manual of Medical Therapeutics, p. 701 | Yamada's Textbook of Gastroenterology | Berek & Novak's Gynecology, p. 1084
Disclaimer: This is educational information only and not a substitute for professional medical advice. Please consult a healthcare provider for diagnosis and treatment.
Age 20
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
At age 20, the differential shifts substantially. Here is the refined picture:
Age-Adjusted Differential Diagnosis
What's MUCH less likely now
- Diverticulitis - rare under 40, not a realistic concern at 20
- Colon cancer - extremely uncommon at this age
- Colonoscopy is not routinely recommended under age 45 unless alarm features are present
Top Conditions at Age 20
#1 - Irritable Bowel Syndrome (IBS) - Most Likely Overall
IBS peaks in onset during the teens and 20s and is twice as common in women. At age 20 with no alarm features, this is the leading diagnosis. Key features:
- Recurrent lower abdominal pain, often left-sided (sigmoid colon)
- Altered bowel habits - constipation, diarrhea, or alternating
- Bloating, gas, and excessive belching as co-symptoms
- Symptoms relieved (or worsened) by defecation
- No fever, no weight loss, no blood in stool
Per Goldman-Cecil Medicine, new onset of symptoms before age 50 with no alarm features strongly favors a functional diagnosis like IBS. Routine colonoscopy is specifically not recommended under age 45 for IBS workup.
Alarm features that would push you away from IBS:
- Rectal bleeding
- Unintentional weight loss
- Nocturnal diarrhea (wakes you from sleep)
- Anemia
- Family history of IBD or colon cancer
#2 - Inflammatory Bowel Disease (IBD) - Crohn's Disease
Crohn's disease commonly first presents in the teens and 20s. It can involve any part of the GI tract, often causing:
- Left lower OR right lower abdominal pain (depending on segment involved)
- Chronic diarrhea
- Weight loss
- Fatigue and anemia
- Occasional fever
It can mimic IBS early on, which is why fecal calprotectin and CRP are recommended screening tests when IBD is suspected in a young person with IBS-like symptoms. A normal calprotectin strongly favors IBS over Crohn's.
#3 - Functional Dyspepsia + Gas Hypersensitivity
Indigestion and excessive burping at age 20 are very commonly due to:
- Functional dyspepsia - bloating, early fullness, indigestion with no structural cause
- Aerophagia / supragastric belching - swallowing air habitually, often stress-related
- FODMAP sensitivity - fermentable carbs (wheat, onions, legumes, dairy, apples) producing excess gas
- H. pylori infection - common in young adults, causes dyspepsia and can cause GI upset
#4 - Lactose Intolerance / Food Sensitivity
Very common at this age - causes bloating, gas, belching, and lower abdominal cramping after dairy or certain foods. Often confused with IBS.
Diagnostic Approach for a 20-Year-Old
Recommended basic workup:
| Test | Purpose |
|---|---|
| CBC + CRP | Screen for inflammation/anemia |
| Fecal calprotectin | Distinguish IBS from IBD |
| Celiac serologies (tTG-IgA) | Rule out celiac disease |
| H. pylori stool antigen | Rule out H. pylori (explains the indigestion/burping) |
| Dietary review | Identify FODMAP/lactose triggers |
Not recommended at this age (without alarm features):
- Routine colonoscopy
- CT scan as first step
- Food allergy panel
Practical Summary
At 20, IBS is by far the most likely diagnosis for your symptom triad. The burping points toward a functional upper GI component (dyspepsia or aerophagia) happening alongside the lower bowel symptoms - these often co-exist. Start by tracking which foods trigger symptoms, reduce FODMAPs, limit carbonated drinks and gum, and manage stress. If symptoms persist or worsen, a simple blood and stool panel (CRP, calprotectin, celiac screen, H. pylori) is the right next step - not a scope.
See a doctor if you develop fever, blood in stool, weight loss, or symptoms that wake you from sleep.
Sources: Goldman-Cecil Medicine, p. 1418 | Frameworks for Internal Medicine, p. 210 | Berek & Novak's Gynecology, p. 1084
Disclaimer: This is educational content only, not a substitute for professional medical evaluation.
Age 20 female - Indigestion, more burbs, left lower abdomen pain, what's the condition?
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Here is the complete, sex- and age-specific breakdown for a 20-year-old female with indigestion, excessive burping, and left lower abdominal pain:
Differential Diagnosis - 20-Year-Old Female
Being female adds a critical second category of causes: gynecological conditions that closely mimic GI disease. Left lower abdominal pain in a young woman must always be evaluated for both bowel and pelvic/reproductive origins.
Category 1: Gynecological Causes (Female-Specific)
1. Endometriosis - Very Important to Consider
Per Berek & Novak's Gynecology, endometriosis directly causes GI symptoms that can be mistaken for a purely digestive problem:
"Endometriosis can be associated with significant gastrointestinal symptoms - pain, nausea, vomiting, early satiety, bloating and distention, altered bowel habits."
This is a major "masquerader" - it can look exactly like IBS. Red flags suggesting endometriosis over IBS:
- Pain that is cyclical - worse around or during menstruation
- Dysmenorrhea (painful periods), especially severe
- Pain during intercourse (dyspareunia)
- Symptoms that began at or soon after first period
- Average diagnosis delay is 8-12 years due to frequent misdiagnosis as IBS or "normal period pain"
2. Pelvic Inflammatory Disease (PID)
PID is a spectrum of upper genital tract infection (endometritis, salpingitis, tubo-ovarian abscess). Per Red Book 2021:
"Clinicians need to maintain a high degree of suspicion for PID when a woman of reproductive age presents with mild or nonspecific findings, particularly in a young female who might provide an incomplete or inaccurate sexual history."
Key features:
- Lower abdominal/pelvic pain (can be left-sided)
- Abnormal vaginal discharge
- Fever or chills
- Pain with intercourse
- Caused by Chlamydia, Gonorrhoea, and other organisms
- Young women are biologically more susceptible due to cervical ectopy
- Subclinical PID is common - symptoms can be mild and easily missed
3. Ovarian Cyst
Functional ovarian cysts are extremely common in women of reproductive age. They cause:
- Unilateral lower abdominal aching or pressure (left or right)
- Bloating and a sense of fullness (mimics indigestion)
- Intermittent pain that may worsen mid-cycle (ovulation)
- Can rupture or undergo torsion, causing sudden severe pain
4. Primary Dysmenorrhea
The most common cause of pelvic pain in young women. Defined as menstrual pain without underlying pelvic pathology. Causes lower abdominal/pelvic cramping that can be accompanied by nausea, bloating, and GI upset due to prostaglandin release - which directly explains the indigestion and gas symptoms around the time of periods.
5. Ectopic Pregnancy
If sexually active and a period has been missed or is late - this must be ruled out immediately. A ruptured ectopic pregnancy is life-threatening. Symptoms: left or right lower pain, vaginal bleeding, shoulder tip pain, dizziness. A urine pregnancy test is the first step.
Category 2: GI Causes (Same as Before)
| Condition | Why it fits |
|---|---|
| IBS | #1 functional GI diagnosis in young women (2x more common in females); lower abdominal pain + bloating + altered bowel habits |
| Functional dyspepsia | Explains indigestion + burping; often coexists with IBS |
| Crohn's disease | Peaks in teens/20s; chronic lower abdominal pain + diarrhea + weight loss |
| FODMAP / lactose intolerance | Gas, bloating, lower cramping after food |
| H. pylori | Causes dyspepsia/indigestion and burping |
Critical Point: IBS vs. Endometriosis - Frequently Confused
These two conditions overlap heavily in young women:
| Feature | IBS | Endometriosis |
|---|---|---|
| Lower abdominal pain | Yes | Yes |
| Bloating | Yes | Yes |
| Altered bowel habits | Yes | Yes |
| Cyclical with periods | No | Yes |
| Pain improves with defecation | Often | Not typically |
| Painful periods | Not characteristic | Hallmark |
| Painful intercourse | Rare | Common |
If symptoms are worse around menstruation, endometriosis is the more likely diagnosis and needs gynaecological evaluation.
What to Do Next
See a doctor for:
- A pelvic examination
- Pregnancy test (urine hCG) - if sexually active
- Pelvic ultrasound - to check ovaries and uterus
- STI screen (Chlamydia, Gonorrhoea) - if sexually active, to rule out PID
- Blood tests: CBC, CRP, fecal calprotectin, celiac screen
- Dietary review for FODMAP/lactose triggers
Go to ER immediately if:
- Sudden severe pain (possible ovarian torsion or ectopic pregnancy rupture)
- Missed period + positive pregnancy test + abdominal pain
- High fever with pelvic pain
- Dizziness or fainting with abdominal pain
Most Likely Diagnosis by Scenario
| Situation | Most Likely Cause |
|---|---|
| Pain is cyclical, worse with periods | Endometriosis or dysmenorrhea |
| Pain after certain foods, relieved by stooling | IBS |
| Vaginal discharge + fever | PID |
| Mid-cycle pain, bloating, left side | Ovarian cyst |
| Indigestion + burping regardless of cycle | Functional dyspepsia / IBS |
| Sexually active + missed period | Ectopic pregnancy - rule out urgently |
Sources: Berek & Novak's Gynecology, pp. 628-629 | Red Book 2021, pp. 893-894 | Goldman-Cecil Medicine, p. 1418
Disclaimer: This is educational information only. A 20-year-old female with these symptoms should see a doctor for proper physical and pelvic examination to distinguish between these conditions.
This is a shared conversation. Sign in to Orris to start your own chat.