Chest expansbilty koti normally? According to macloid?
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
Macleod's clinical examination chest expansibility normal value cm
Reading File
Finding Sources
Finding Sources
Macleod's is not in the textbook library, but the answer is well-established from multiple authoritative sources. Here is the answer:
Chest Expansibility - Normal Value (Macleod's)
According to Macleod's Clinical Examination, normal chest expansibility is > 5 cm (i.e., at least 5 cm).
How it is measured:
- The circumference of the chest is measured at the level of the 4th intercostal space (nipple level in men).
- Measured first at full expiration, then at full inspiration.
- The difference between the two readings = chest expansibility.
- Normal = 5 cm or more.
Clinical significance:
| Finding | Interpretation |
|---|---|
| > 5 cm | Normal |
| < 2.5 cm | Significant - suggests pathology (e.g., Ankylosing Spondylitis, COPD, pleural effusion) |
| Asymmetric expansion | Pathology on the side with reduced expansion |
Key causes of reduced chest expansion:
- Unilateral reduction: Pleural effusion, pneumothorax, consolidation, collapse, fibrosis
- Bilateral reduction: COPD (hyperinflation), Ankylosing Spondylitis (costovertebral fusion), bilateral pleural disease, obesity
Note: In Ankylosing Spondylitis, a chest expansion of < 2.5 cm has good specificity (though poor sensitivity) for the diagnosis, and it is one of the modified New York criteria for AS. - Washington Manual of Medical Therapeutics; Firestein & Kelley's Textbook of Rheumatology
What is ankylosing spindylitis
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of Ankylosing Spondylitis from the medical textbooks:
Ankylosing Spondylitis (AS)
Definition
Ankylosing spondylitis (AS) - now also called radiographic axial spondyloarthritis - is a chronic, multisystem inflammatory spondyloarthropathy primarily affecting the axial skeleton (spine and sacroiliac joints). Sacroiliitis and enthesitis of the axial skeleton are the hallmarks. - Goldman-Cecil Medicine; Grainger & Allison's Diagnostic Radiology
Epidemiology
- Prevalence: ~0.2% of the general population
- ~2% of HLA-B27 positive individuals develop AS
- ~20% of HLA-B27 positive individuals with an affected family member develop AS
- Male : Female = 3 : 1 (historically up to 5:1, but more recent studies show lower ratio)
- Onset: typically young adults, can begin in adolescence
Pathogenesis (Pathobiology)
- Strongly associated with HLA-B27 (90% of patients)
- HLA-B27 has a unique tendency to misfold in the endoplasmic reticulum, triggering a pro-inflammatory cascade called the unfolded protein response
- HLA-B27 also forms heavy-chain homodimers on the cell surface, contributing to inflammation
- Molecular mimicry with gram-negative enteric bacteria has been proposed
- Gut microbiome plays a role - germ-free HLA-B27 transgenic rats show markedly reduced joint disease
- Inflammation begins at entheses (sites where ligaments/tendons insert into bone), especially around the sacroiliac joints and spine
Clinical Features
Axial Symptoms (Primary)
- Chronic low back pain lasting > 3 months
- Inflammatory pattern: worse in the morning, improves with exercise, NOT relieved by rest
- Early-morning stiffness (often lasting hours)
- Pain around sacroiliac joints, may radiate to buttocks
- Back pain that wakes the patient from sleep is a red flag for inflammatory back pain
- Fatigue is common
As Disease Progresses
- Progressive loss of spinal mobility
- Reduced chest expansion (< 2.5 cm is specific for AS)
- Forward stoop / kyphosis
Peripheral Joint Involvement (~30%)
- Asymmetric oligoarthritis, predominantly lower limbs
- Hip joints - second most commonly affected (after sacroiliac joints)
- Enthesitis: Achilles tendinitis, plantar fasciitis (heel pain)
Extra-articular Manifestations
| System | Manifestation |
|---|---|
| Eyes | Acute anterior uveitis (iritis) - up to 40% of patients |
| Lungs | Upper lobe fibrosis/bullous disease (pulmonary manifestation) |
| Heart | Aortitis, aortic regurgitation, conduction defects |
| Gut | Association with IBD (Crohn's/UC) |
MRI of Sacroiliac Joints in AS
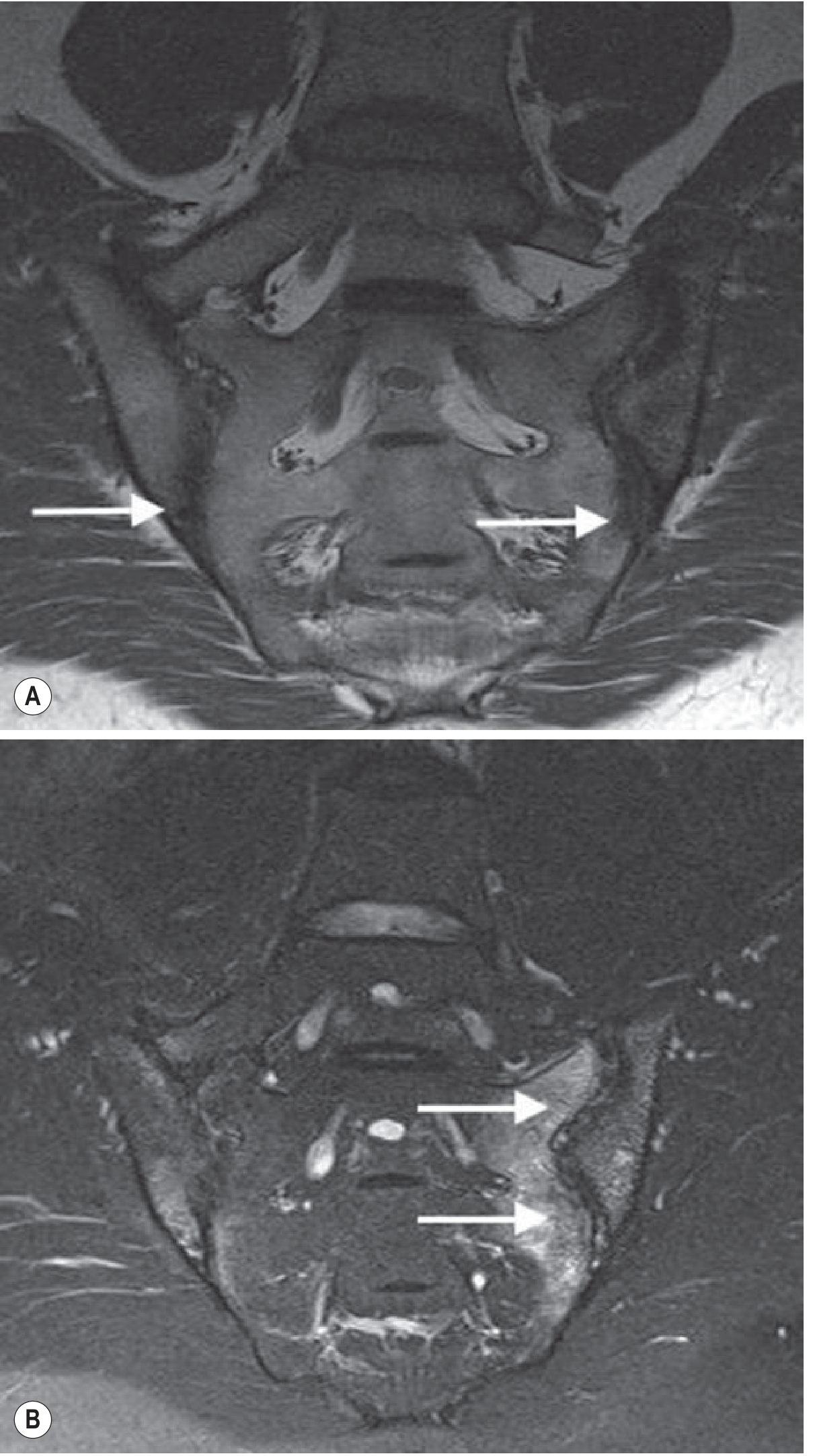
T1-weighted image (A) shows erosions in the sacroiliac joints with joint space loss. T2 fat-suppressed image (B) shows extensive subchondral oedema reflecting active disease.
MRI of Thoracic Spine in AS

STIR sagittal MRI of the thoracic spine showing oedema within the costovertebral joints at multiple levels, characteristic of AS.
Radiology
| Stage | Finding |
|---|---|
| Early | Subchondral bone marrow oedema on MRI (sacroiliac joints) |
| Early X-ray | Romanus lesions - sclerotic "shiny corners" of vertebral bodies |
| Intermediate | Squared vertebral bodies, thin marginal syndesmophytes |
| Late/Severe | Bamboo spine - complete fusion of vertebral bodies and sacroiliac joints |
Note: Spinal fractures are a serious complication - the fused, osteopenic spine is paradoxically brittle and transverse fractures can be catastrophic.
Diagnostic Criteria
Modified New York Criteria for AS
Clinical criteria:
- Low back pain and stiffness for > 3 months, improves with exercise but not rest
- Limitation of lumbar spine motion in both sagittal and frontal planes
- Limitation of chest expansion
Radiologic criterion:
- Sacroiliitis: grade ≥2 bilateral, or grade 3-4 unilateral
Definite AS = Radiologic criterion + at least 1 clinical criterion
Probable AS = All 3 clinical criteria present, OR radiologic criterion without clinical criteria
Differential Diagnosis
| Feature | Rheumatoid Arthritis | AS | Psoriatic Arthritis | Reactive Arthritis |
|---|---|---|---|---|
| M:F ratio | 1:3 | 3:1 | 1:1 | 10:1 |
| HLA | DR4 | B27 | B27 (axial) | B27 |
| Joint pattern | Symmetric peripheral | Axial | Axial + asymmetric peripheral | Axial + asymmetric peripheral |
| Sacroiliac | Absent | Bilateral, symmetric | Asymmetric | Asymmetric |
| Syndesmophytes | Absent | Smooth, marginal | Coarse, nonmarginal | Coarse, nonmarginal |
| Eye | Scleritis | Iritis | +/- | Iritis + conjunctivitis |
| RF | >80% | Rare | Rare | Rare |
Treatment
Step 1 - NSAIDs: Continuous NSAIDs are preferred over on-demand use for axial disease.
Step 2 - Biologics (if inadequate NSAID response):
- Anti-TNF agents (e.g., infliximab, adalimumab, etanercept) - first-line biologic
- IL-17 inhibitors (e.g., secukinumab, ixekizumab) - strongly recommended for active AS with inadequate NSAID response; preferred over TNF inhibitors in patients with demyelinating disease risk
Note: Sulfasalazine and methotrexate (DMARDs) are only recommended for peripheral arthritis, not axial disease.
Physical therapy and exercise are important throughout all stages. - Goldman-Cecil Medicine; Rheumatology 2-Volume Set (Elsevier 2022)
Deviation of trachia causes
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
I now have enough information from multiple authoritative textbook sources. Here is the complete answer:
Causes of Tracheal Deviation
The trachea is normally in the midline. Deviation is either due to something pushing it away or pulling it toward one side.
The Core Principle (Easy Memory Rule)
| Direction of Deviation | Mechanism | Side of Pathology |
|---|---|---|
| Away from the lesion | Pushed - space-occupying lesion | Ipsilateral (same side as the lesion) |
| Toward the lesion | Pulled - volume-losing lesion | Ipsilateral (same side as the lesion) |
Causes: Trachea Deviated AWAY from the Lesion (Pushed)
These are space-occupying / volume-increasing processes that push the mediastinum to the opposite side:
- Tension pneumothorax - most urgent/life-threatening cause; air under pressure pushes trachea away
- Massive pleural effusion - large fluid accumulation pushes trachea to opposite side
- Large haemothorax
- Diaphragmatic hernia - abdominal contents herniate into chest, pushing mediastinum
- Large mediastinal mass / tumour - e.g., lymphoma, thymoma
- Aortic aneurysm - displaces trachea
- Multinodular goiter / large thyroid mass - enlarged thyroid can deviate trachea to the contralateral side
On chest X-ray: tracheal deviation AWAY from an opacified (white) hemithorax = volume-occupying process (e.g., pleural effusion). - Frameworks for Internal Medicine
Causes: Trachea Deviated TOWARD the Lesion (Pulled)
These are volume-losing processes that pull the mediastinum toward the affected side:
- Pulmonary collapse / atelectasis - most common; lung collapses, pulling trachea toward it
- Pulmonary fibrosis - scarring contracts the lung, pulling trachea ipsilaterally
- Pleural fibrosis - fibrothorax/old empyema with fibrosis
- Post-pneumonectomy - removal of a lung pulls trachea to that side
- Post-lobectomy (if large enough)
- Phrenic nerve palsy with subsequent lung collapse
On chest X-ray: tracheal deviation TOWARD an opacified (white) hemithorax = volume-losing process (e.g., atelectasis, collapse, fibrosis). - Frameworks for Internal Medicine
Quick Summary Table
| Cause | Direction of Deviation | Mechanism |
|---|---|---|
| Tension pneumothorax | Away from lesion | Pushed (pressure) |
| Massive pleural effusion | Away from lesion | Pushed (fluid) |
| Large haemothorax | Away from lesion | Pushed (fluid) |
| Mediastinal mass / tumour | Away from lesion | Pushed (mass) |
| Large goiter / thyroid mass | Away from lesion | Pushed (mass) |
| Aortic aneurysm | Away from lesion | Pushed (mass) |
| Pulmonary collapse / atelectasis | Toward lesion | Pulled (volume loss) |
| Pulmonary fibrosis | Toward lesion | Pulled (fibrosis) |
| Pleural fibrosis | Toward lesion | Pulled (fibrosis) |
| Post-pneumonectomy | Toward lesion | Pulled (absent lung) |
Important Clinical Note
- In simple (non-tension) pneumothorax, tracheal deviation is usually absent - it only occurs with tension pneumothorax when pressure is sufficient to shift the mediastinum.
- Pemberton's sign: Raising both arms above the head can worsen tracheal compression/deviation from a large goiter, causing facial flushing and respiratory distress.
- Tracheal compression > 70% of the tracheal diameter is usually required before significant airway compromise occurs (e.g., from goiter). - Harrison's Principles of Internal Medicine, 22nd Ed.
Retristernal goitre hole ki hoi
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent - comprehensive information gathered. Here is the full answer:
Retrosternal Goiter (Intrathoracic Goiter)
Definition / "Kya hoti hai?"
Retrosternal goiter (also called substernal, intrathoracic, or cervicomediastinal goiter) is an enlarged thyroid gland that extends below the thoracic inlet into the chest (behind the sternum / retrosternally into the mediastinum).
Two most commonly used definitions:
- Any goiter that extends below the thoracic inlet (with patient in surgical position), OR
- Any goiter where more than 50% of the gland lies below the thoracic inlet
Incidence: Up to 20% of all goiters have intrathoracic extension. - Scott-Brown's Otorhinolaryngology
Types
| Type | Description |
|---|---|
| Secondary intrathoracic goiter (common) | Cervical thyroid that grows downward through the thoracic inlet - still gets blood from superior/inferior thyroid arteries |
| Primary intrathoracic goiter (rare, <1%) | Arises from ectopic thyroid tissue in the mediastinum - gets blood supply from intrathoracic vessels - seen as incidental mediastinal mass on X-ray |
Chest X-Ray - Primary Intrathoracic Goiter
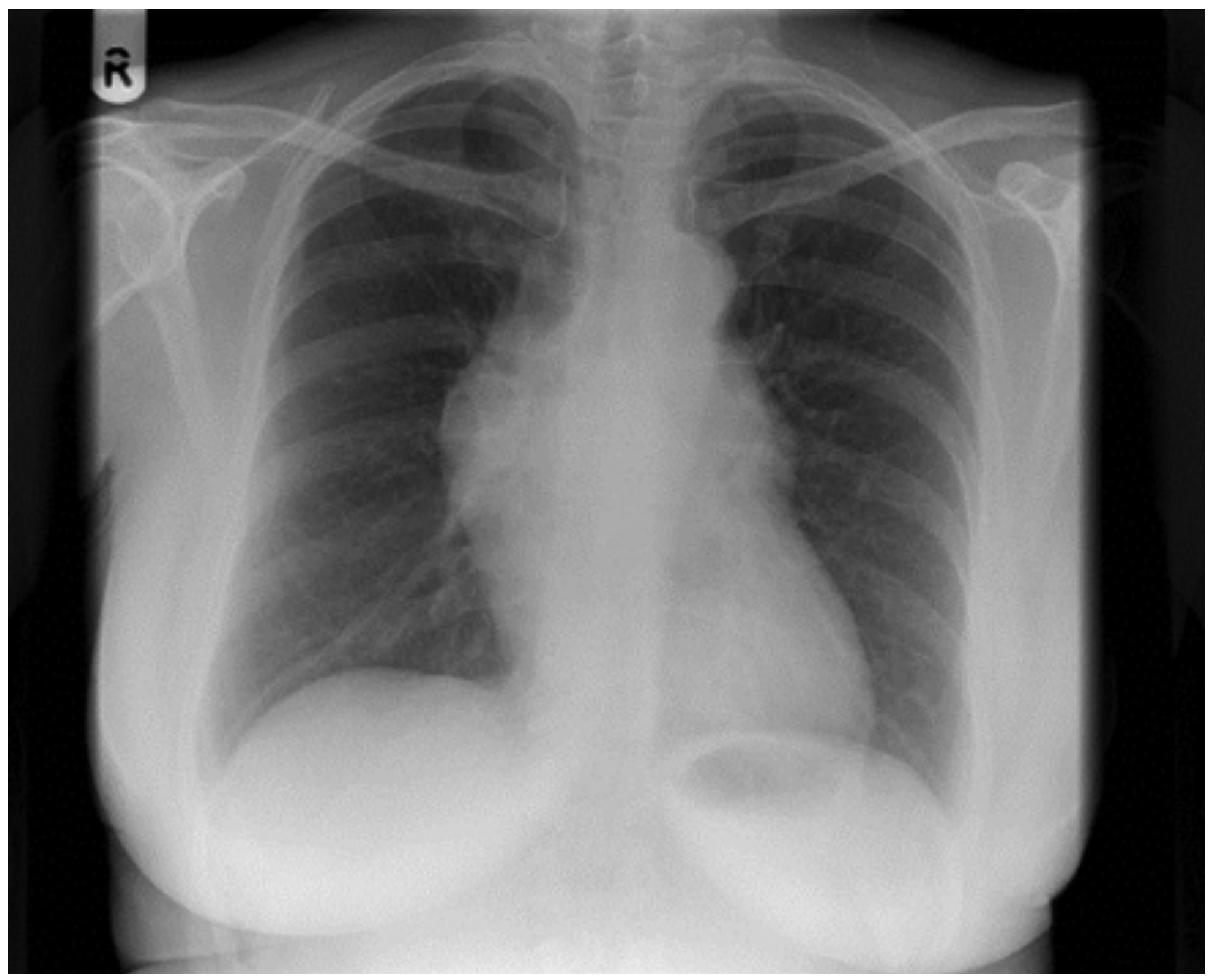
Chest X-ray showing incidental mediastinal mass (widened superior mediastinum) due to primary intrathoracic goiter
Why Does It Grow Downward? (Aetiology)
- Neck musculature obstructs extra-thoracic growth, directing the goiter downward
- Negative intrathoracic pressure and downward traction from swallowing pull it into the chest
- 90% grow into the anterior mediastinum; only 10-15% grow into the posterior mediastinum
- Majority are right-sided - because the great vessels (aorta) impede extension into the left thorax
Clinical Presentation
Asymptomatic
- Up to 40% are asymptomatic, discovered incidentally on chest X-ray
- May present as a barely palpable or impalpable neck mass (majority of thyroid is in the chest)
Symptomatic (due to compression)
| Structure Compressed | Symptom |
|---|---|
| Trachea (most common) | Dyspnea, cough, wheeze, stridor, acute airway distress (up to 20%) |
| Esophagus | Dysphagia |
| Recurrent laryngeal nerve | Hoarseness, voice change |
| Superior vena cava | SVC syndrome - facial oedema, upper limb oedema, plethora, cyanosis, papilloedema, dilated chest veins |
| Sympathetic chain | Horner's syndrome (ptosis, miosis, anhidrosis) |
| Thoracic duct | Chylothorax |
Pemberton's Sign (IMPORTANT)
When both arms are raised above the head, facial congestion, cyanosis, and respiratory distress appear - indicating increased thoracic inlet pressure from the retrosternal mass. This is pathognomonic of retrosternal goiter.
Investigations
- Thyroid function tests (TFTs/TSH) - most are euthyroid (80%); up to 30% have subclinical thyrotoxicosis
- Ultrasound - good for cervical thyroid; cannot assess intrathoracic component
- CT scan - best imaging modality for intrathoracic extension; shows extent, tracheal deviation/compression, mediastinal compartment involved
- Sternotomy more likely needed if goiter extends below the aortic arch
- MRI - useful for defining relationship with surrounding structures
- Radionuclide scan (¹²³I / ¹³¹I) - confirms thyroid origin; primary intrathoracic goiters often show reduced iodine avidity
- Flow-volume loop spirometry - to assess respiratory compromise (but correlates poorly with goiter weight)
Rule: If you cannot palpate the distal extent of a goiter, CT scan is mandatory.
Management
Non-Surgical Options
| Option | Details |
|---|---|
| Observation | For asymptomatic, euthyroid, benign goiters without intrathoracic extension |
| Radioiodine (¹³¹I) | Reduces non-toxic goiter size by 30-45% over 1-2 years in ~80% of patients; for those unfit or refusing surgery |
Surgery (Main Treatment)
- Surgery is indicated when trachea is compressed by ≥35% on axial CT (American Thyroid Association guideline)
- Route of surgery:
- Cervical approach (standard) - used in >95% of cases; retrosternal portion delivered into operative field by dividing isthmus and taking down superior pole
- Sternotomy - required if goiter extends below aortic arch or malignancy suspected; carries 25% risk of respiratory complications vs 2% for cervical approach
- Blood supply: Secondary intrathoracic goiter is ligated via neck vessels (superior/inferior thyroid arteries), NOT from thoracic vessels - this is why most can be removed via a cervical incision
Risks to Remember
- Recurrent laryngeal nerve injury
- Hypoparathyroidism
- Spontaneous intraglandular haemorrhage → acute respiratory distress (rare but real risk)
- Patients with retrosternal goiter tend to be older, frailer, with higher surgical risk
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery; Schwartz's Principles of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.