tell me about Ecmo
Reading File
Searching the Web
ECMO extracorporeal membrane oxygenation overview indications 2024
Finding Sources
Searching PubMed
extracorporeal membrane oxygenation ECMO outcomes
Reading File
Reading File
Reading File
Loading Image
I now have excellent content from two authoritative textbooks plus the circuit diagram. Let me compile a comprehensive answer.
Extracorporeal Membrane Oxygenation (ECMO)
What Is ECMO?
ECMO is a form of prolonged extracorporeal life support for patients with life-threatening cardiac and/or pulmonary failure that is refractory to conventional therapy, including CPR. It traces its roots to the cardiopulmonary bypass circuit invented by Gibbon, first used in 1953 during open-heart surgery. The modern ECMO era began in 1975 when Bartlett successfully applied it in neonates with severe respiratory distress.
The ECMO Circuit
The basic circuit has four components:
| Component | Role |
|---|---|
| Inflow (drainage) cannula | Drains venous blood from the patient into the circuit |
| Centrifugal pump | Maintains blood flow through the circuit |
| Membrane oxygenator | Adds O₂, removes CO₂; also has a heat exchanger to warm blood |
| Outflow (return) cannula | Returns oxygenated blood to the patient |
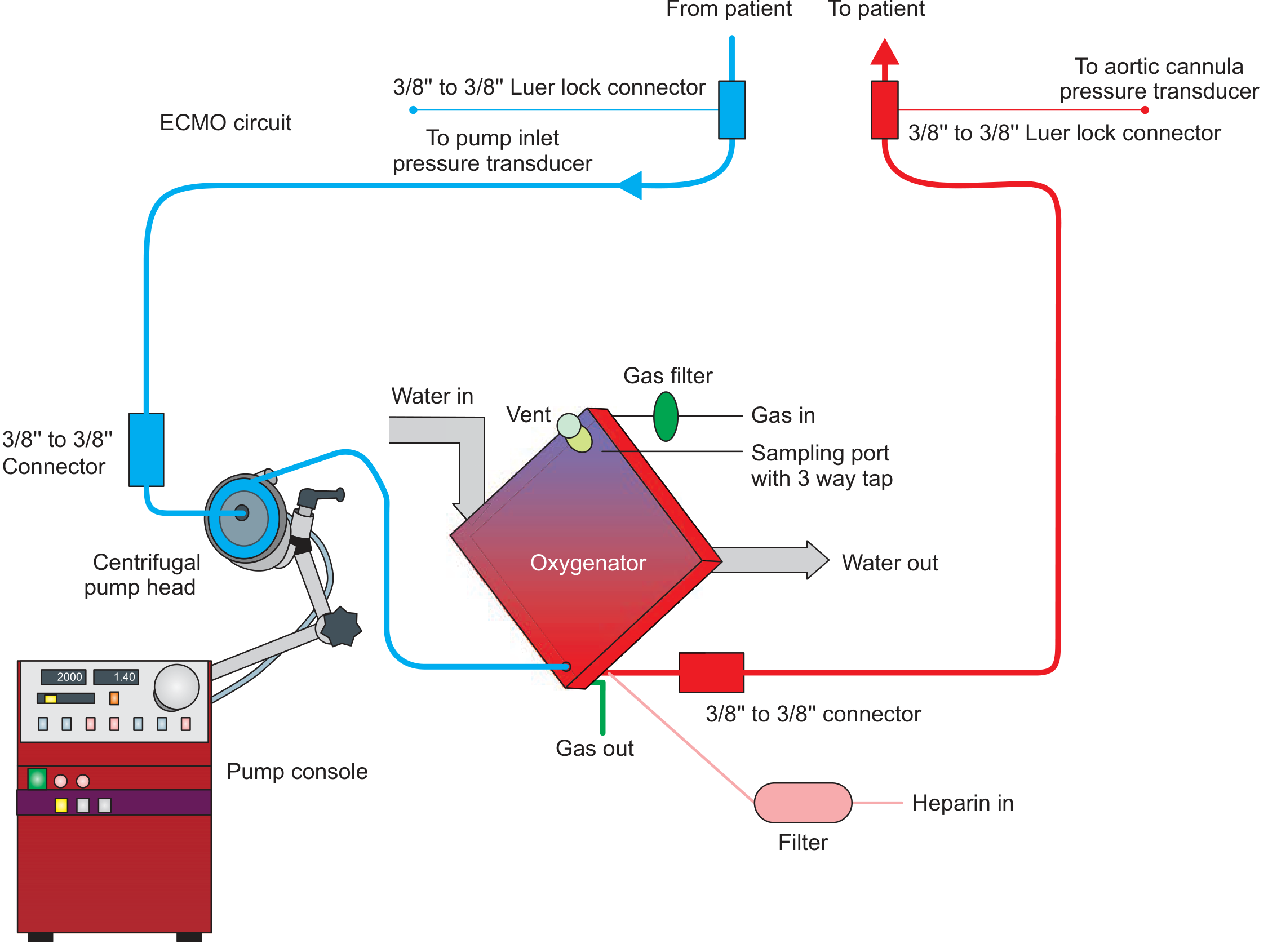
Heparin is infused into the circuit continuously for anticoagulation. Modern oxygenators use polymethylpentene (PMP) hollow-fibre membranes, which have superior durability and gas transfer compared to older silicone membranes.
Two Main Types
1. Veno-Venous (VV) ECMO
- Support provided: Lungs only (oxygenation + CO₂ removal)
- Circuit: Blood drained from a large vein → oxygenated → returned to another vein (typically right heart)
- Common cannulation: Right femoral vein (inflow) + right internal jugular vein (outflow)
- Alternative: Dual-lumen single cannula (e.g., Avalon cannula) via right IJ
- Native cardiac function: Must be intact - VV ECMO does not provide hemodynamic support
- Primary use: ARDS, severe pneumonia, acute respiratory failure
2. Veno-Arterial (VA) ECMO
- Support provided: Heart AND lungs (full cardiopulmonary bypass equivalent)
- Circuit: Venous blood drained (femoral/IJ vein) → oxygenated → returned to an artery (usually femoral, less often subclavian via graft)
- Native cardiac function: Bypassed; provides systemic perfusion
- Primary use: Cardiogenic shock, cardiac arrest, bi-ventricular failure, post-cardiotomy shock
- Key limitation: Can cause pulmonary edema and left ventricular (LV) fluid overload; does not adequately unload a severely impaired LV. Often requires adjuncts like Impella, IABP, or inotropes to vent the LV.
Indications
Respiratory (VV ECMO)
- Severe ARDS (P/F ratio < 80 mmHg despite optimal ventilation)
- Acute respiratory failure refractory to conventional management
- COVID-19 associated severe ARDS
- Bridge to lung transplant
- Status asthmaticus / massive pulmonary embolism (selected cases)
Cardiac (VA ECMO)
- Cardiogenic shock (including MI-related)
- Cardiac arrest refractory to CPR (ECPR - extracorporeal CPR)
- Acute myocarditis
- Post-cardiotomy shock (failure to wean from bypass)
- Bridge to ventricular assist device (VAD) or heart transplant
- Drug-induced cardiovascular collapse (e.g., overdose)
Contraindications
- Absolute: Irreversible end-organ failure without transplant candidacy; severe aortic regurgitation (VA ECMO); aortic dissection
- Relative: Severe coagulopathy or uncontrolled bleeding; advanced age with poor prognosis; prolonged cardiac arrest without CPR (poor neurological prognosis)
Clinical Management on ECMO
- Anticoagulation: Unfractionated heparin (UFH) is standard; target anti-Xa or aPTT per institutional protocol. Heparin-induced thrombocytopenia (HIT) requires switching to argatroban or bivalirudin.
- Ventilator settings: "Lung rest" strategy on VV ECMO - low tidal volumes (2-4 mL/kg), low PEEP, low FiO₂ to prevent ventilator-induced lung injury (VILI)
- Flow rates: Typically 3-6 L/min in adults; adjusted based on patient weight and oxygenation needs
- Sweep gas: Controls CO₂ removal (higher sweep = more CO₂ removed)
- FiO₂ on circuit: Controls oxygenation
- Prone positioning: Can still be performed safely on VV ECMO
Key Complications
| Complication | Notes |
|---|---|
| Bleeding | Most common; cannula sites, intracranial hemorrhage |
| Thrombosis / embolism | Circuit clot, stroke |
| Limb ischemia | Distal perfusion catheter often placed in VA ECMO |
| Infection | Circuit-related bloodstream infections |
| LV distension | VA ECMO specifically; requires LV venting |
| Recirculation | VV ECMO; drained blood immediately re-enters inflow |
| Oxygenator failure | Requires circuit change |
ECMO as Bridge Therapy
ECMO is not a destination therapy - it is always a bridge to one of:
- Bridge to recovery - heart/lungs heal; ECMO removed
- Bridge to transplant - lung or heart transplant
- Bridge to decision - time to assess neurological/organ recovery
- Bridge to durable device - VAD implantation
Key Clinical Trials
- CESAR trial (2009): VV ECMO at specialized centers improved 6-month survival without severe disability vs. conventional ventilation in severe ARDS (63% vs 47%)
- EOLIA trial (2018): Randomized trial of VV ECMO in severe ARDS; did not reach its primary endpoint (mortality reduction at 60 days) due to high crossover (28% of control patients received ECMO). A Bayesian reanalysis by Golgher et al. suggested the trial was statistically underpowered and favored ECMO.
- Recent evidence (2026): A systematic review on long-term psychological outcomes after ECMO highlights significant PTSD, anxiety, and depression in survivors - an increasingly recognized area of post-ECMO care (PMID 42235101). For cardiogenic shock, a Lancet meta-analysis (2024) of individual patient data from randomized trials of temporary mechanical circulatory support found that VA ECMO in MI-related cardiogenic shock did not improve 6-month outcomes versus standard care, reinforcing the need for careful patient selection (PMID 39236726).
Differences from Cardiopulmonary Bypass
| Feature | ECMO | CPB |
|---|---|---|
| Duration | Days to weeks/months | Hours (intraoperative) |
| Purpose | Bridge (respiratory/cardiac recovery) | Intraoperative support |
| Setting | ICU | Operating room |
| Circuit priming | Smaller volume | Larger |
Sources:
- Fishman's Pulmonary Diseases and Disorders (Ch. 149 - ECMO in Acute Respiratory Failure)
- Fischer's Mastery of Surgery, 8th Ed. (p. 346 - VA ECMO in Cardiovascular Support)
- StatPearls: ECMO in Adults
This is a shared conversation. Sign in to Orris to start your own chat.