Entamoeba history tics for 2 nd bds microbiology
Reading File
Finding Sources
Searching the Web
Entamoeba histolytica important points BDS microbiology exam
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from the medical microbiology textbooks. Let me compile the full BDS-focused answer.
Entamoeba histolytica - High-Yield Points for 2nd BDS Microbiology
1. Classification (Taxonomy)
| Feature | Detail |
|---|---|
| Kingdom | Protista (Protozoa) |
| Phylum | Sarcomastigophora |
| Class | Lobosea |
| Order | Amoebida |
| Species | Entamoeba histolytica |
| Disease caused | Amebiasis (Amoebiasis) |
2. Morphology - Two Key Forms
A. Trophozoite (Vegetative Form) - Invasive form
- Size: 12-60 µm (average 15-30 µm)
- Only form found in tissues
- Cytoplasm has two zones: hyaline ectoplasm (outer) + granular endoplasm (inner)
- PATHOGNOMONIC FEATURE: Contains ingested red blood cells (erythrophagocytosis) in cytoplasm
- Single nucleus with a central, small karyosome + fine, evenly distributed peripheral chromatin
- Motility: Unidirectional, rapid movement with pseudopodia (finger-like)
- Found in: liquid/diarrheal stools; survives only a few hours outside host
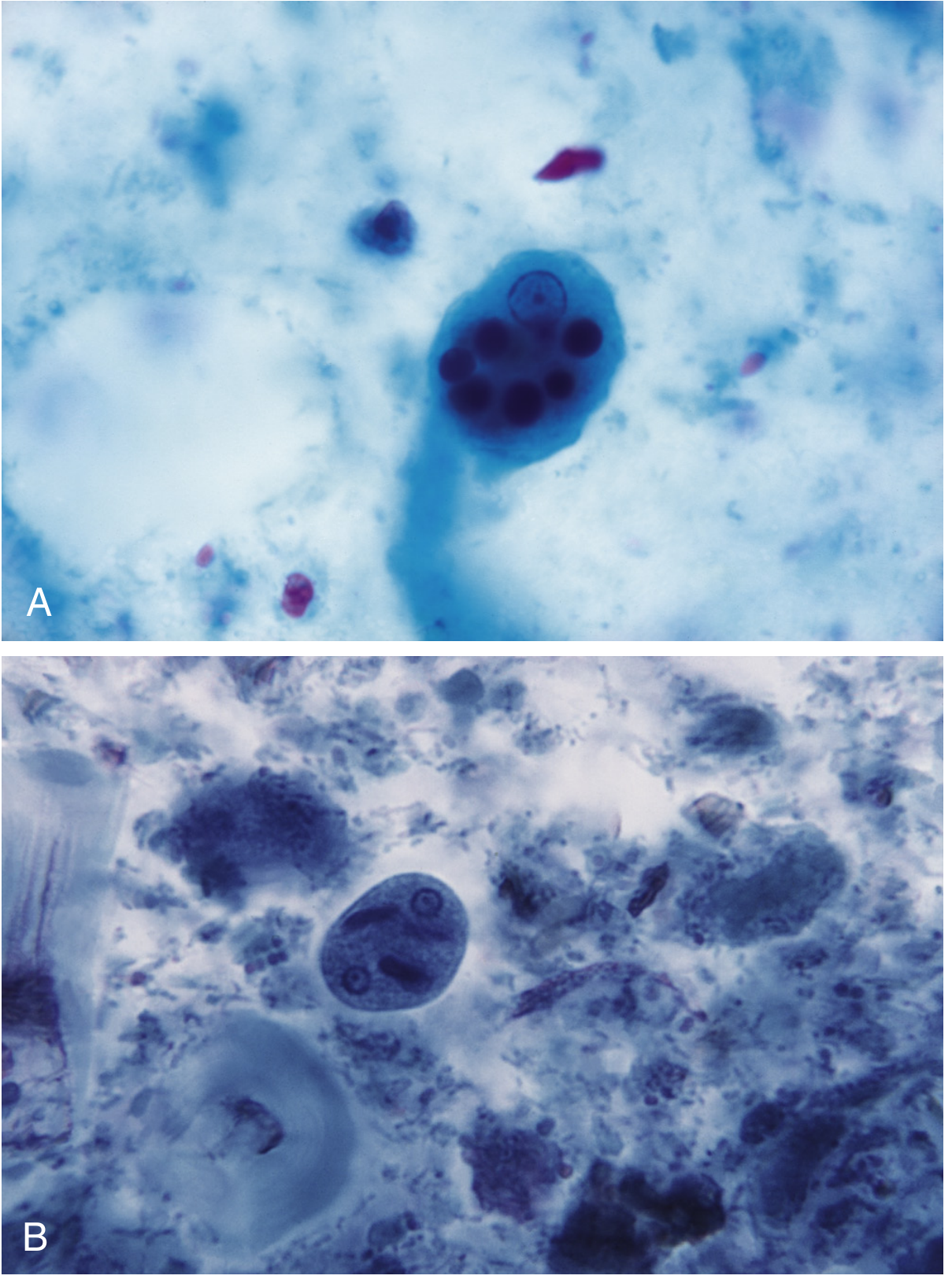
B. Cyst (Infective Form) - Transmission form
- Size: 10-20 µm
- Up to 4 nuclei (mature quadrinucleate cyst is infective)
- Contains chromatoid bars with rounded/blunt ends (important to distinguish from E. coli - which has splintered/frayed ends)
- May contain glycogen vacuole (disappears in mature cyst)
- Found in: formed/solid stools; resistant to gastric acid, chlorination
3. Life Cycle
Ingestion of mature quadrinucleate CYST (fecal-oral route)
↓
Excystation in duodenum (gastric acid stimulates release)
↓
TROPHOZOITES released → multiply in large intestine
↓
Either:
(a) Invade colonic epithelium → Disease (amebiasis)
(b) Remain in lumen → form PRE-CYST → mature CYST
↓
Cysts passed in formed feces → Environmental contamination
↓
Re-ingestion (fecal-oral route) completes cycle
- Definitive host: Humans (only natural host)
- No intermediate host
- Infective stage: Mature quadrinucleate cyst
- Diagnostic stage: Trophozoite (diarrheal stool) or Cyst (formed stool)
4. Pathogenesis - "Flask-Shaped Ulcer" (High-Yield!)
- Cysts excyst in duodenum → trophozoites invade large intestine (especially cecum, ascending colon, sigmoid, rectum)
- Trophozoites attach via galactose-inhibitable adherence lectin (Gal/GalNAc lectin)
- Cause lytic necrosis of colonic epithelial cells by:
- Cytotoxin production
- Lethal alteration of host cell membrane permeability
- Irreversible rise in intracellular calcium
- Classic lesion: Flask-shaped ulcer - small point of entry, narrow neck, expanded necrotic submucosa
- Lysis of neutrophils → toxic contents released → further tissue destruction
- Ameboma: inflammatory granulomatous mass in intestinal wall (can mimic carcinoma)
Extraintestinal Spread:
- Via portal circulation → Liver (most common - right lobe affected)
- Amebic liver abscess: contains "anchovy paste/chocolate sauce" material (sterile, necrotic)
- Less common: lungs, brain, spleen, pericardium
5. Clinical Features
Intestinal Amebiasis:
- Majority are asymptomatic carriers (most carry non-pathogenic E. dispar)
- Symptomatic: crampy abdominal pain, diarrhea, dysentery
- Amoebic dysentery: bloody mucoid stools ("red-currant jelly" stool), tenesmus
- No fever typically (unlike bacillary dysentery)
Amebic Liver Abscess (Extraintestinal):
- Right hypochondriac pain, hepatomegaly
- Elevation of right dome of diaphragm
-
50% of liver abscess patients give NO history of intestinal symptoms
- Diagnosed by USG/CT/MRI
6. Laboratory Diagnosis
| Test | Finding/Note |
|---|---|
| Stool microscopy (gold standard for intestinal) | Trophozoites with RBCs in cytoplasm (pathognomonic) |
| Multiple stool samples | At least 3 samples needed (parasites unevenly distributed) |
| Hot stool examination | To find motile trophozoites in diarrheal stool |
| Trichrome / iron-hematoxylin stain | Permanent stain for detailed morphology |
| Stool antigen detection (EIA/ELISA) | Highly specific; distinguishes E. histolytica from E. dispar |
| Serology (IHA, IFA, ELISA) | Positive in >90% of liver abscess cases; useful for extraintestinal |
| PCR | Gold standard for species differentiation |
| Proctoscopy/colonoscopy | Flask-shaped ulcers with normal intervening mucosa |
| USG/CT abdomen | For liver abscess (hypoechoic lesion, right lobe) |
7. Differentiation: E. histolytica vs E. coli (Very Exam-Frequent!)
| Feature | E. histolytica | E. coli |
|---|---|---|
| Trophozoite size | 12-50 µm | 20-30 µm |
| Cyst size | 10-20 µm | 10-30 µm |
| Nucleus - karyosome | Central, small, sharp | Eccentric, large, irregular |
| Peripheral chromatin | Fine, evenly dispersed | Coarse, clumped, irregular |
| Ingested RBCs | Present (pathognomonic) | Absent |
| Cyst nuclei number | 1-4 (max 4) | 1-8 (up to 8) |
| Chromatoid bars | Rounded ends | Splintered/frayed ends |
| Pathogenicity | Pathogenic | Non-pathogenic (commensal) |
8. E. histolytica vs E. dispar (Important!)
- Morphologically identical - cannot be differentiated by microscopy
- E. dispar is the non-pathogenic, more common commensal form
- Differentiated by: isoenzyme analysis (zymodeme), monoclonal antibody-based stool antigen tests, PCR
- Only E. histolytica contains erythrocytes in trophozoite cytoplasm
9. Treatment
| Situation | Drug of Choice |
|---|---|
| Intestinal/invasive amebiasis | Metronidazole (tissue amebicide) |
| Asymptomatic cyst passers (luminal) | Diloxanide furoate (Furamide) - luminal amebicide |
| Luminal alternatives | Iodoquinol, Paromomycin |
| Amebic liver abscess | Metronidazole + luminal amebicide (to clear intestinal source) |
- Note: Metronidazole alone does NOT eradicate luminal cysts - always follow with a luminal agent.
10. Epidemiology
- Worldwide distribution; highest in tropical/subtropical regions with poor sanitation
- Prevalence 10-15% in endemic areas; up to 50% in some zones
- ~50 million cases/year globally; up to 100,000 deaths/year
- 2nd most common cause of death from parasitic disease (after malaria)
- Transmission: fecal-oral (contaminated water, food, vegetables)
- Mechanical vectors: flies, cockroaches
- High-risk groups: institutionalized patients, homosexual men (oral-anal practices), travelers to endemic areas
11. Quick-Recall Points for MCQs
- Infective form = mature quadrinucleate cyst
- Diagnostic form in tissue = trophozoite
- RBCs in cytoplasm = pathognomonic of E. histolytica
- Ulcer shape = Flask-shaped
- Liver abscess contents = "Anchovy paste" (chocolate sauce colored)
- Most common site of liver abscess = Right lobe
- Drug for invasive = Metronidazole; drug for luminal/cyst passer = Diloxanide furoate
- Non-pathogenic lookalike = E. dispar
- Chromatoid bars in E. histolytica = rounded ends (vs splintered in E. coli)
Sources: Medical Microbiology (Murray), 9th ed.; Jawetz, Melnick & Adelberg's Medical Microbiology, 28th ed.
Leishmania Donovani 2nd bds microbiology
Finding Sources
Searching the Web
Leishmania donovani important points 2nd BDS microbiology exam high yield
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
I now have comprehensive information from multiple textbooks. Let me compile the complete BDS-focused answer.
Leishmania donovani - High-Yield Points for 2nd BDS Microbiology
1. Classification (Taxonomy)
| Feature | Detail |
|---|---|
| Kingdom | Protista (Protozoa) |
| Phylum | Sarcomastigophora |
| Class | Zoomastigophora |
| Order | Kinetoplastida |
| Genus | Leishmania |
| Species | L. donovani |
| Group | Hemoflagellate (blood flagellate) |
| Disease | Visceral Leishmaniasis (Kala-azar) |
2. Historical Facts (MCQ-Favourite!)
- Discovered in 1903 simultaneously by:
- William Boog Leishman - found parasite in spleen smears from soldiers in India
- Charles Donovan - found it at Government General Hospital, Madras
- Hence named Leishman-Donovan (LD) bodies - the amastigote stage seen in tissue
- "Kala-azar" = Hindi for "black fever" (due to skin darkening)
- "Dum-Dum fever" - after Dum-Dum cantonment near Calcutta where early cases described
3. Morphology - TWO Key Stages
A. Amastigote (Leishman-Donovan body) - in HUMANS
- Size: 2-3 µm, oval/round
- Non-flagellate (no external flagellum)
- Found intracellularly inside macrophages/reticuloendothelial cells
- On Leishman/Giemsa stain: "dot and dash" appearance
- Dot = nucleus (round, red-purple)
- Dash = kinetoplast (rod-shaped, dark-staining, next to nucleus)
- Found in: spleen, liver, bone marrow, lymph nodes
B. Promastigote (Leptomonad form) - in SANDFLY
- Size: 15-25 µm, elongated/spindle-shaped
- Has a free anterior flagellum (motile)
- Kinetoplast at anterior end
- Found in: sandfly gut + saliva (infective stage)
- Cultivated on NNN medium (Novy-MacNeal-Nicolle medium)
4. Life Cycle
SANDFLY (Phlebotomus) - Intermediate/Vector Host
|
Infected sandfly bites human → injects PROMASTIGOTES
↓
Promastigotes phagocytosed by macrophages/monocytes
↓
Convert to AMASTIGOTES inside macrophages
(lose flagellum, become intracellular)
↓
Amastigotes multiply by binary fission → fill cytoplasm
↓
Cell bursts → released amastigotes phagocytosed by new macrophages
↓
Spreads via reticuloendothelial system:
SPLEEN → LIVER → BONE MARROW → LYMPH NODES
↓
Uninfected sandfly bites infected human → ingests amastigotes
↓
In sandfly midgut: amastigotes → PROMASTIGOTES (with flagella)
↓
Migrate to sandfly proboscis → infective for next bite
- Definitive host: Humans
- Intermediate/Vector: Female sandfly (Phlebotomus spp.)
- Infective stage to humans: Promastigote
- Diagnostic stage in humans: Amastigote (LD body)
5. Vector - Sandfly (Phlebotomus)
| Feature | Detail |
|---|---|
| Vector | Phlebotomus argentipes (India - main vector) |
| Other vectors | P. perniciosus, P. ariasi (Mediterranean) |
| New World vector | Lutzomyia longipalpis |
| Only females bite | Yes - require blood meal for egg development |
| Active time | Dusk to dawn (night-biting) |
| Flight range | Very limited (<1 km) |
| Breeding sites | Damp soil, leaf litter, cracks in walls |
6. Reservoirs
| Region | Reservoir |
|---|---|
| India | Humans (anthroponotic - human-vector-human) |
| Mediterranean/China/Middle East | Dogs (canine reservoir) |
| Sudan/Africa | Wild carnivores, rodents |
| South America | Domestic dogs, wild canids |
7. Pathogenesis & Clinical Features - Visceral Leishmaniasis
Incubation period: 1-4 months (can be up to 1 year)
The parasite invades the reticuloendothelial system - attacking:
Cardinal Features (HFAS mnemonic):
- Hepatosplenomegaly (massive splenomegaly - most prominent sign)
- Fever - intermittent, irregular, sometimes double-daily spike; 39-40°C
- Anemia + Agranulocytosis + thrombocytopenia (pancytopenia)
- Skin darkening (hyperpigmentation - especially forehead, temples, perioral, midabdomen) → "Kala-azar" = black fever
Progressive Disease:
- Emaciation, marked weight loss, weakness
- Epistaxis, purpura (due to thrombocytopenia)
- Susceptibility to secondary bacterial infections
- Oral ulcerations (cancrum oris/noma)
- FATAL if untreated - death ~2 years from onset
Post-Kala-Azar Dermal Leishmaniasis (PKDL):
- Occurs 1-2 years after apparent cure of kala-azar
- Especially in India
- Macular/maculopapular/nodular skin rash (face, trunk)
- Parasites abundant in skin lesions
- Patient becomes a reservoir for transmission
- Treated with prolonged antimony therapy
8. Laboratory Diagnosis
Definitive Diagnosis:
| Test | Specimen | Finding |
|---|---|---|
| Splenic aspirate smear | Spleen pulp | Best yield (>95% sensitive); risk of bleeding |
| Bone marrow biopsy | Sternal/iliac marrow | Safe; good yield |
| Liver biopsy | Liver tissue | Lower sensitivity |
| Lymph node aspiration | Lymph node | Useful if enlarged |
| Peripheral blood smear | Blood (buffy coat) | In Indian kala-azar (heavy parasitemia) |
| NNN medium culture | Any of above | Promastigotes grow at 22-25°C |
Stain used: Leishman stain or Giemsa stain → shows LD bodies (amastigotes) inside macrophages
Serological Tests:
| Test | Details |
|---|---|
| Aldehyde (Napier's) test | Formalin gel test - turbidity within 20 min; indicates hypergammaglobulinemia (not specific) |
| DAT (Direct Agglutination Test) | Sensitive and specific; widely used in field |
| rK39 ICT (Immunochromatography) | Rapid diagnostic test, field-applicable, high sensitivity/specificity |
| IFA, ELISA | High sensitivity |
| Complement Fixation Test | Older test |
Montenegro (Leishmanin) Skin Test:
- NEGATIVE during active kala-azar (anergy due to immunosuppression)
- Becomes positive after cure (indicates past exposure/immunity)
- Not useful for active diagnosis of visceral leishmaniasis
Other:
- Pancytopenia on CBC (anemia + leukopenia + thrombocytopenia)
- Hypergammaglobulinemia (polyclonal) + hypoalbuminemia (reversed A:G ratio)
- Elevated ESR, elevated serum bilirubin, abnormal liver function tests
- PCR: most sensitive and specific; used for species identification
9. Treatment
| Drug | Use |
|---|---|
| Amphotericin B (liposomal) | First-line in India (due to antimony resistance); least toxic form |
| Sodium stibogluconate (Pentostam) | Pentavalent antimonial; traditional DOC worldwide; IM/IV |
| Miltefosine | Oral alkyl-phosphocholine; first oral drug for kala-azar; used in India and Ethiopia; as effective as amphotericin B |
| Meglumine antimoniate (Glucantime) | Alternative pentavalent antimonial |
| Paromomycin | Alternative/combination therapy |
India note: Widespread resistance to antimonials (sodium stibogluconate) → Amphotericin B / Miltefosine now preferred in India
10. Comparison of Leishmaniasis Types (High-Yield Table)
| Feature | Visceral (Kala-azar) | Cutaneous (Oriental Sore) | Mucocutaneous (Espundia) |
|---|---|---|---|
| Species | L. donovani | L. tropica, L. major | L. braziliensis |
| Vector | Phlebotomus argentipes | P. papatasi | Lutzomyia spp. |
| Reservoir (India) | Humans | Humans/rodents | Wild animals |
| Lesion site | Viscera (spleen, liver, BM) | Skin (self-healing) | Skin + mucosa (destructive) |
| Other name | Black fever, Dum-Dum fever | Delhi boil, Baghdad boil | Espundia |
| Montenegro test | Negative | Positive | Positive |
| Outcome | Fatal if untreated | Self-limiting | Disfiguring |
11. Quick-Recall Points for MCQs
| Point | Answer |
|---|---|
| Causative organism of kala-azar | Leishmania donovani |
| Tissue form (in humans) | Amastigote (LD body) |
| Flagellate form (in sandfly/culture) | Promastigote |
| Vector in India | Phlebotomus argentipes |
| Culture medium | NNN medium |
| "Dot and dash" appearance | Nucleus (dot) + Kinetoplast (dash) |
| Kala-azar = | "Black fever" (skin darkening) |
| Most sensitive specimen for diagnosis | Splenic aspirate |
| Aldehyde test positive = | Hypergammaglobulinemia (non-specific) |
| Montenegro test in active kala-azar | NEGATIVE (anergy) |
| Most prominent organ affected | Spleen (massive splenomegaly) |
| Oral drug for kala-azar | Miltefosine |
| Post-kala-azar dermal leishmaniasis | 1-2 years after cure, skin nodules |
| Pancytopenia caused by | Bone marrow infiltration |
| Reservoir in India | Humans (anthroponotic) |
Sources: Medical Microbiology (Murray), 9th ed.; Jawetz, Melnick & Adelberg's Medical Microbiology, 28th ed.; Andrews' Diseases of the Skin, Clinical Dermatology
This is a shared conversation. Sign in to Orris to start your own chat.