Explain diabetes mellitus pharmacology in detailed
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
diabetes mellitus pharmacotherapy guidelines
Loading Image
Reading File
I now have all the detailed content needed. Let me compile the comprehensive response.
Diabetes Mellitus Pharmacology: A Detailed Overview
Source: Lippincott Illustrated Reviews: Pharmacology; Katzung's Basic and Clinical Pharmacology, 16th Ed; Harrison's Principles of Internal Medicine 22E
I. Background and Classification
Diabetes mellitus is a heterogeneous group of syndromes characterized by elevated blood glucose from a relative or absolute deficiency of insulin. The American Diabetes Association (ADA) recognizes four main types:
| Feature | Type 1 | Type 2 |
|---|---|---|
| Onset | Childhood/puberty | Commonly >35 years |
| Body habitus | Undernourished | Obesity common |
| Prevalence | 5-10% of DM | 90-95% of DM |
| Defect | Beta-cell destruction, no insulin | Insulin resistance + inadequate secretion |
Diagnostic criteria:
- Fasting plasma glucose ≥ 126 mg/dL
- 2-hr postprandial glucose ≥ 200 mg/dL
- HbA1c ≥ 6.5%
- ADA target for most patients: A1C ≤ 7% (mean glucose ≤ 154 mg/dL)
II. Insulin
Types and Pharmacokinetics
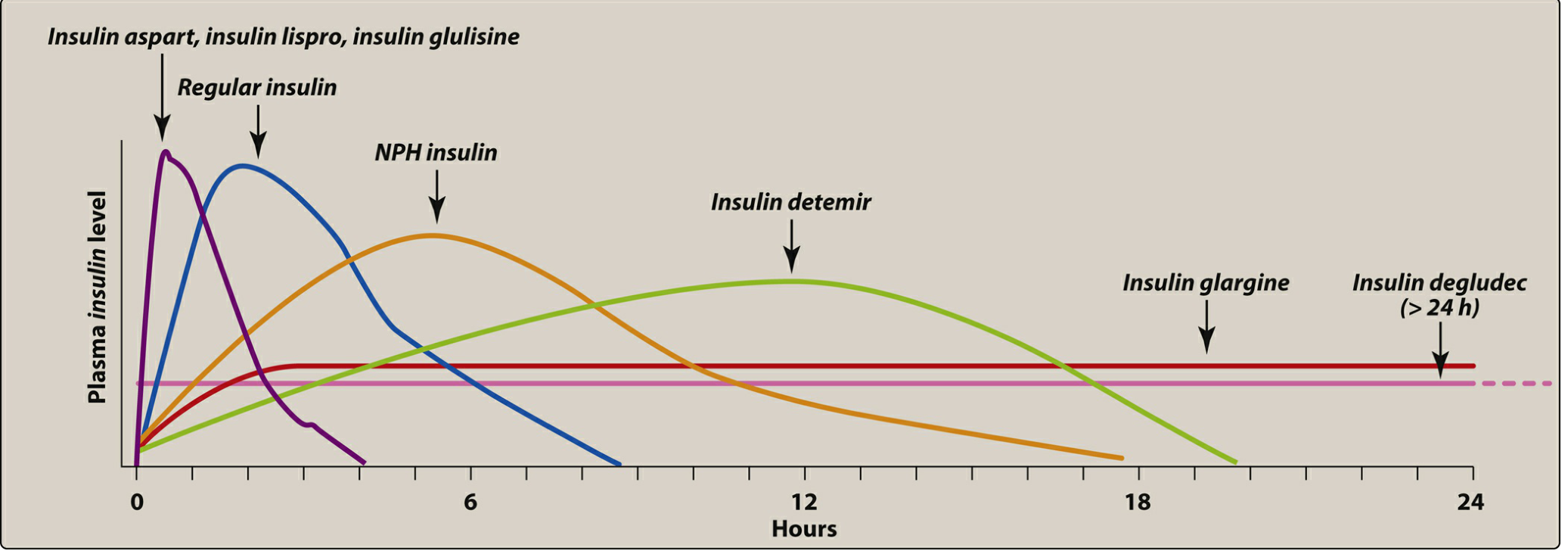
Rapid-acting (prandial coverage):
- Insulin lispro, aspart, glulisine - Onset 15-30 min, peak 30-90 min; given 15 min before or within 15-20 min after a meal
- Inhaled insulin - peak within 10-20 min; dry powder absorbed through pulmonary tissue
- Used to mimic prandial insulin release; can also be used in insulin pumps
Short-acting:
- Regular insulin - Onset ~30 min, peak 50-120 min; inject 30 min before a meal; used IV in DKA
Intermediate-acting:
- NPH (Neutral Protamine Hagedorn) - Formed by adding zinc and protamine to regular insulin; delayed absorption, longer duration; used as basal insulin; given subcutaneously only (never IV)
Long-acting (basal insulins):
- Insulin glargine - A "peakless" basal insulin with a flat profile lasting ~24 hours; precipitates at subcutaneous pH
- Insulin detemir - Binds albumin; prolonged action up to ~18 hours
- Insulin degludec - Ultra-long acting (>24 hours); forms multi-hexamers in subcutaneous tissue
Mechanism of Action
Insulin binds its tyrosine kinase receptor on target cells (liver, muscle, adipose), triggering GLUT-4 translocation to cell surfaces to increase glucose uptake. In the liver, it suppresses gluconeogenesis and promotes glycogen synthesis.
Adverse Effects
- Hypoglycemia - most serious and common; risk highest with intensive regimens
- Weight gain
- Lipodystrophy - local atrophy or hypertrophy at injection sites
- Hypokalemia - insulin drives K+ into cells
Intensive vs. Standard Therapy
Intensive therapy (≥3 injections/day with frequent monitoring) achieves better A1C control and significantly reduces microvascular complications (retinopathy, nephropathy, neuropathy), but increases hypoglycemic episodes, coma, and seizures. Not recommended for elderly patients, those with long-standing disease or hypoglycemic unawareness.
III. Amylin Analog: Pramlintide
Drug: Pramlintide (synthetic amylin analog)
Mechanism: Delays gastric emptying, decreases postprandial glucagon secretion, promotes satiety
Use: Adjunct to mealtime insulin in both Type 1 and Type 2 diabetes
Key points:
- Reduce mealtime insulin dose by 50% when initiating (risk of severe hypoglycemia)
- Cannot be mixed with insulin in the same syringe
- Contraindicated in diabetic gastroparesis and hypoglycemic unawareness
- Adverse effects: nausea, anorexia, vomiting
IV. Oral Agents for Type 2 Diabetes
A. Biguanides - Metformin (First-line therapy)
Metformin is the preferred initial therapy for Type 2 diabetes, started at diagnosis.
Mechanism of action:
- Reduces hepatic gluconeogenesis (primary effect - addresses the major source of fasting hyperglycemia)
- Slows intestinal absorption of sugars
- Improves peripheral glucose uptake and insulin sensitivity
Key distinction: Does NOT promote insulin secretion - therefore, hypoglycemia risk is very low with monotherapy
Pharmacokinetics: Well absorbed orally; not protein-bound; not metabolized; renally excreted unchanged
Adverse effects:
- GI: diarrhea, nausea, vomiting (minimize by slow dose titration, take with food)
- Weight loss (reduces appetite)
- Lactic acidosis (rare but potentially fatal)
- Vitamin B12 deficiency with long-term use - monitor B12 levels, especially with anemia or peripheral neuropathy
Contraindications / Cautions:
- Severe renal dysfunction (eGFR <30 mL/min/1.73 m²) - lactic acidosis risk
- Acute MI, decompensated heart failure, sepsis (acute renal failure risk)
- Caution: age >80 years, alcohol abuse history
- Temporarily hold for IV contrast procedures
B. Sulfonylureas (Insulin Secretagogues)
Drugs: Second-generation - glipizide, glyburide, glimepiride
Mechanism of action: Bind ATP-sensitive K+ channels on pancreatic beta cells → channel closure → membrane depolarization → Ca²+ influx → insulin secretion (glucose-independent)
Pharmacokinetics: Oral; protein-bound; hepatically metabolized; excreted in urine and feces; duration 12-24 hours
Adverse effects:
- Hypoglycemia (most significant - glucose-independent mechanism)
- Hyperinsulinemia
- Weight gain
- Drug interactions: many drugs potentiate hypoglycemia (e.g., sulfonamides, NSAIDs, warfarin) or reduce glycemic control (e.g., thiazides, corticosteroids)
Renal considerations: Glyburide is most problematic in renal dysfunction - accumulates and worsens hypoglycemia risk. Glipizide or glimepiride are safer choices in renal impairment and elderly patients.
C. Meglitinides (Postprandial Glucose Regulators)
Drugs: Repaglinide, nateglinide
Mechanism: Like sulfonylureas - close ATP-sensitive K+ channels on beta cells. However, rapid onset and shorter duration make them effective specifically for early postprandial insulin release.
Pharmacokinetics:
- Take before each meal
- Repaglinide: metabolized via CYP2C8/3A4; excreted in feces
- Nateglinide: metabolized via CYP2C9/3A4; excreted in urine
Adverse effects: Hypoglycemia and weight gain (less than sulfonylureas)
Key caution:
- Do NOT combine with sulfonylureas (overlapping mechanism, severe hypoglycemia risk)
- Gemfibrozil (lipid-lowering) inhibits CYP2C8, markedly increases repaglinide levels - combination contraindicated
D. Thiazolidinediones (TZDs) - Insulin Sensitizers
Drugs: Pioglitazone, rosiglitazone
Mechanism: Agonists at PPARγ (peroxisome proliferator-activated receptor-gamma), a nuclear hormone receptor in adipose tissue, liver, and skeletal muscle. PPARγ activation regulates insulin-responsive gene transcription → increased insulin sensitivity. Require insulin for their action but do NOT stimulate its release (no hyperinsulinemia risk).
Adverse effects:
- Fluid retention and edema
- Weight gain
- Increased risk of osteoporotic fractures (especially in women)
- Pioglitazone: potential increased risk of bladder cancer
- Contraindicated in symptomatic heart failure (fluid retention worsens heart failure)
E. GLP-1 Receptor Agonists (Incretin Mimetics)
Background - The Incretin Effect: Oral glucose triggers 60-70% of postprandial insulin secretion via gut-released incretins (GLP-1 and GIP). This incretin effect is markedly reduced in Type 2 diabetes.
Drugs (all injectable): Dulaglutide, exenatide, liraglutide, lixisenatide, semaglutide
(Semaglutide is also available orally)
Mechanism of action:
- Bind and activate GLP-1 receptors on pancreatic beta cells → glucose-dependent insulin secretion
- Decrease postprandial glucagon secretion
- Slow gastric emptying (reduce postprandial glucose excursion)
- Enhance satiety / reduce food intake → weight loss
- Promote beta-cell proliferation
Cardiovascular benefits: Dulaglutide, liraglutide, and semaglutide are approved to reduce cardiovascular mortality in Type 2 DM with established CVD.
Adverse effects:
- Nausea, vomiting, constipation (most common - GI)
- Pancreatitis (rare)
- Thyroid C-cell tumors (seen in animal studies; avoid in personal/family history of MTC or MEN2)
Note: Do NOT combine with DPP-4 inhibitors (overlapping mechanism, increased toxicity potential).
F. DPP-4 Inhibitors (Gliptins)
Drugs: Sitagliptin, saxagliptin, linagliptin, alogliptin
Mechanism: Inhibit dipeptidyl peptidase-4 (DPP-4), the enzyme that rapidly inactivates GLP-1 and GIP. By prolonging incretin activity → increased mealtime insulin secretion (glucose-dependent) and reduced glucagon. Weight-neutral (no satiety effect unlike GLP-1 agonists).
Pharmacokinetics:
- Well absorbed orally; food does not affect absorption
- Sitagliptin and alogliptin: renally excreted unchanged
- Saxagliptin: CYP3A4/5 metabolism to active metabolite; renal excretion
- Linagliptin: primarily enterohepatic elimination (no renal dose adjustment needed)
- All except linagliptin require dose adjustment in renal dysfunction
Adverse effects:
- Generally well tolerated
- Nasopharyngitis, headache
- Rare but serious: hypersensitivity reactions, pancreatitis, severe joint pain
- Saxagliptin increases risk of heart failure hospitalizations - use with caution in heart failure
G. SGLT2 Inhibitors (Gliflozins)
Drugs: Canagliflozin, dapagliflozin, empagliflozin, ertugliflozin
Mechanism: Inhibit sodium-glucose cotransporter 2 (SGLT2) in the proximal renal tubule → decreased glucose reabsorption → increased urinary glucose excretion (glycosuria). Also reduces sodium reabsorption → osmotic diuresis → mild blood pressure reduction.
Added cardiovascular and renal benefits:
- Canagliflozin and empagliflozin: approved to reduce cardiovascular death in T2DM + CVD
- Canagliflozin and dapagliflozin: reduce heart failure hospitalizations and progression to end-stage kidney disease
- Dapagliflozin and empagliflozin: approved for heart failure with reduced ejection fraction (HFrEF), even without diabetes
Mechanism in heart failure: NHE (sodium-hydrogen exchanger) inhibition, reduced glucose utilization for ATP, slowed CKD progression - these appear to be class effects.
Adverse effects:
- Genital mycotic infections (most common - due to glycosuria)
- Urinary tract infections
- Urinary frequency/polyuria
- Euglycemic DKA (especially in Type 1 DM - not approved for T1DM)
- Canagliflozin: increased risk of lower-limb amputation and fractures
H. Alpha-Glucosidase Inhibitors
Drugs: Acarbose, miglitol
Mechanism: Inhibit intestinal alpha-glucosidases → slow breakdown and absorption of complex carbohydrates → reduce postprandial glucose spikes
Adverse effects: Flatulence, bloating, diarrhea (undigested carbohydrates fermented by gut bacteria)
V. Drug Class Summary Table
| Drug Class | Example Agents | Primary Mechanism | Hypoglycemia Risk | Weight Effect |
|---|---|---|---|---|
| Insulin | Glargine, lispro, NPH | Direct glucose uptake | High | Gain |
| Metformin | Metformin | ↓ Hepatic gluconeogenesis | Very low | Neutral/loss |
| Sulfonylureas | Glipizide, glyburide, glimepiride | ↑ Insulin secretion (K+ channel) | High | Gain |
| Meglitinides | Repaglinide, nateglinide | ↑ Prandial insulin secretion | Moderate | Gain |
| TZDs | Pioglitazone | PPARγ agonist, ↑ insulin sensitivity | Very low | Gain |
| GLP-1 agonists | Semaglutide, liraglutide | Incretin mimetic, ↑ satiety | Very low | Loss |
| DPP-4 inhibitors | Sitagliptin, linagliptin | ↑ Incretin duration | Very low | Neutral |
| SGLT2 inhibitors | Empagliflozin, dapagliflozin | ↑ Urinary glucose excretion | Very low | Loss |
| Alpha-glucosidase inhibitors | Acarbose | ↓ Carbohydrate absorption | Very low | Neutral |
VI. Treatment Strategy
Type 1 DM: Insulin is mandatory (basal-bolus regimen). Pramlintide may be added as an adjunct.
Type 2 DM:
- Step 1: Metformin at diagnosis (unless contraindicated)
- Step 2: Add a second agent based on comorbidities:
- CVD or high CV risk → GLP-1 RA (semaglutide, liraglutide) or SGLT2 inhibitor (empagliflozin, canagliflozin)
- Heart failure → SGLT2 inhibitor preferred
- CKD → SGLT2 inhibitor (canagliflozin, dapagliflozin)
- Weight loss needed → GLP-1 RA or SGLT2 inhibitor
- Hypoglycemia must be avoided → DPP-4 inhibitor, GLP-1 RA, TZD, SGLT2i
- Step 3: Add or intensify with additional agents; add basal insulin when needed
- Insulin: Initiate when A1C remains uncontrolled or in acute illness
VII. Recent Evidence Update
A 2025 living systematic review and network meta-analysis (PMID 40813122, BMJ) confirmed the hierarchy of cardiorenal benefits for SGLT2 inhibitors and GLP-1 receptor agonists, supporting their prioritization in patients with established CVD, heart failure, or CKD beyond glycemic control alone.
A 2024 SMART-C meta-analysis in Lancet Diabetes & Endocrinology (PMID 38991584) showed that combining SGLT2 inhibitors with GLP-1 receptor agonists provides additive cardiorenal protection compared with either agent alone.
Sources: Lippincott Illustrated Reviews: Pharmacology, pp. 792-824; Katzung's Basic and Clinical Pharmacology 16e; Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.