Use this article and Give me objective having 6 to 8 lines Result containing 10 to 12 lines, conclusion containing 4 to 6 lines ,
python3 -c " from pypdf import PdfReader reader = PdfReader('/home/daytona/workspace/attachments/5cc56faa-71e6-4739-a26d-194830252d93/Dissertation Final.pdf') print(f'Total pages: {len(reader.pages)}') text = '' for i, page in enumerate(reader.pages): text += f'\n--- PAGE {i+1} ---\n' text += page.extract_text() or '' print(text[:8000]) "
python3 -c " from pypdf import PdfReader reader = PdfReader('/home/daytona/workspace/attachments/5cc56faa-71e6-4739-a26d-194830252d93/Dissertation Final.pdf') text = '' for i, page in enumerate(reader.pages): text += page.extract_text() or '' # Find objectives, results, conclusion sections import re # Print from page 9 onwards (abstract, objectives usually) page_texts = [] for i, page in enumerate(reader.pages): page_texts.append(page.extract_text() or '') # Print pages 8-20 to find abstract/objectives for i in range(8, 25): print(f'--- PAGE {i+1} ---') print(page_texts[i][:2000]) print() "
python3 -c " from pypdf import PdfReader reader = PdfReader('/home/daytona/workspace/attachments/5cc56faa-71e6-4739-a26d-194830252d93/Dissertation Final.pdf') page_texts = [page.extract_text() or '' for page in reader.pages] # Print results and conclusion sections (pages ~84-125) for i in range(83, 125): print(f'--- PAGE {i+1} ---') print(page_texts[i][:2500]) print() " 2>&1 | tail -300
python3 -c " from pypdf import PdfReader reader = PdfReader('/home/daytona/workspace/attachments/5cc56faa-71e6-4739-a26d-194830252d93/Dissertation Final.pdf') page_texts = [page.extract_text() or '' for page in reader.pages] # Print conclusion and summary pages (around page 120-125) for i in range(125, 140): print(f'--- PAGE {i+1} ---') print(page_texts[i][:3000]) print() "
Objective
Result
Conclusion
18 year girl with primary amenorrhea with turner syndrome Give me a case scenario for this case
Case Scenario: Primary Amenorrhea - Turner Syndrome
Patient Identification
Chief Complaint
History of Present Illness
Past History
- No significant childhood illnesses
- No prior surgeries
- No known drug allergies
- Immunization history: up to date
Family History
- No family history of similar condition
- No history of consanguineous marriage
Menstrual History
- Menarche: Never attained (Primary amenorrhea)
- No history of cyclical pain
General Physical Examination
| Parameter | Finding |
|---|---|
| Height | 142 cm (well below 3rd percentile) |
| Weight | 46 kg |
| BMI | 22.8 kg/m² |
| Blood pressure | 148/94 mmHg (elevated - coarctation screening) |
| Pulse | 82 bpm, regular |
| Build | Short stature, stocky build |
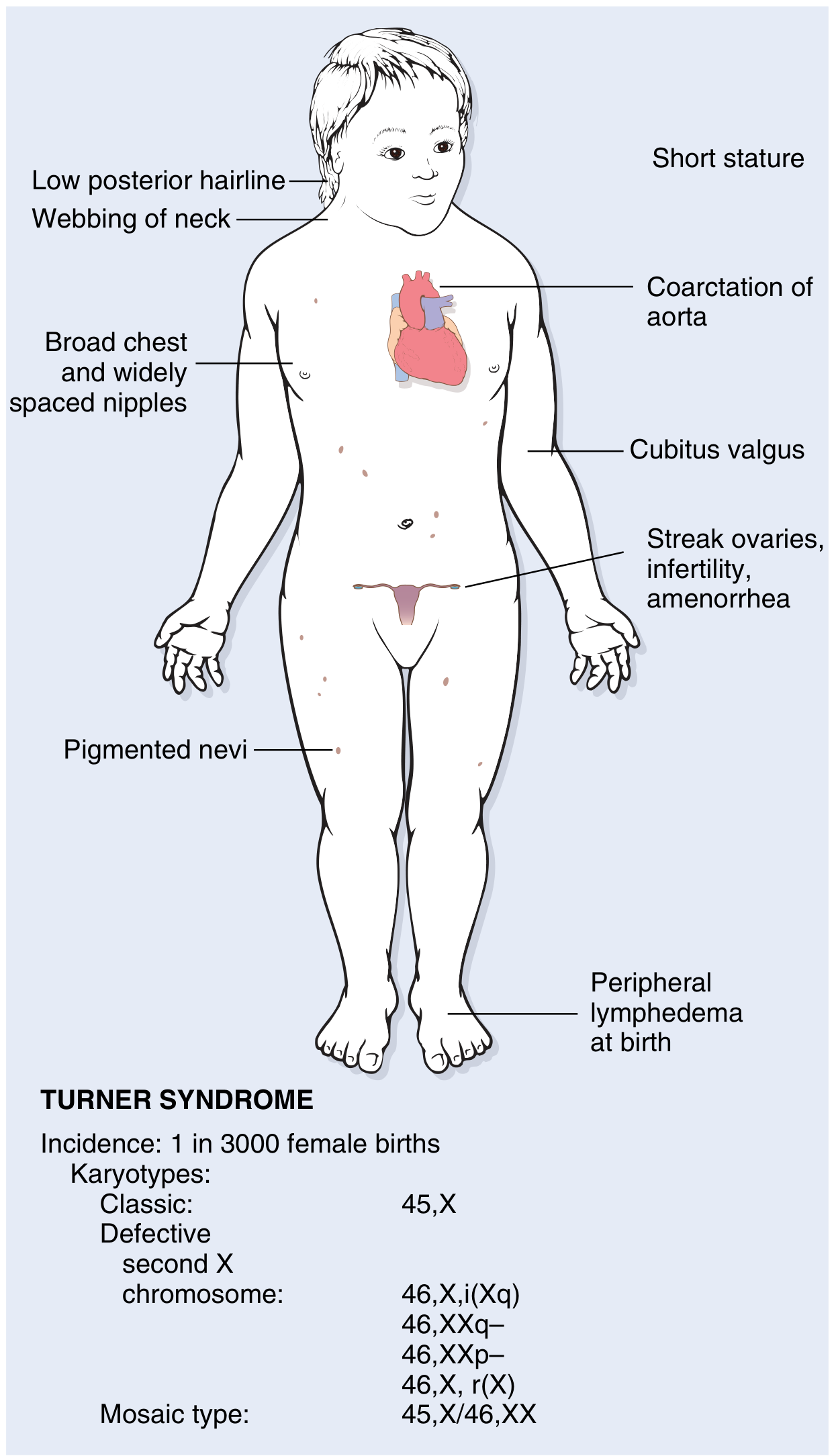
- Low posterior hairline
- Webbing of the neck (pterygium colli)
- Shield-shaped (broad) chest with widely spaced nipples
- Cubitus valgus (increased carrying angle of the arms bilaterally)
- Multiple pigmented nevi over the trunk
- High-arched palate
- Short fourth metacarpals on hand examination
- No peripheral lymphedema at present
Secondary Sexual Characteristics
- Breast development: Absent (Tanner Stage 1)
- Pubic hair: Absent (Tanner Stage 1)
- Axillary hair: Absent
- External genitalia: Normal female, infantile appearance
- Uterus: Small, hypoplastic on per-abdominal examination
Systemic Examination
- Cardiovascular: Systolic murmur heard at the left sternal border and interscapular area; radio-femoral delay present (suggestive of coarctation of aorta)
- Respiratory: Clear to auscultation
- Abdomen: No organomegaly; no palpable pelvic mass
- CNS: Alert, oriented; normal intelligence; mild difficulty with visuospatial tasks noted on informal testing
Investigations Ordered
Hormonal Profile
| Test | Result | Normal |
|---|---|---|
| Serum FSH | 78 mIU/mL | 3-10 mIU/mL (follicular) |
| Serum LH | 42 mIU/mL | 2-15 mIU/mL |
| Serum Estradiol (E2) | <10 pg/mL | 20-350 pg/mL |
| Serum Prolactin | 12 ng/mL | Normal |
| TSH | 6.8 mIU/L | Elevated (subclinical hypothyroidism) |
| Free T4 | Low-normal | |
| Anti-TPO antibodies | Positive | Suggestive of autoimmune thyroiditis |
Karyotype
- Result: 45,X - Confirms Turner syndrome
- No Y chromosome sequences detected
Imaging
- Pelvic ultrasound: Uterus small (4.5 × 1.5 cm); bilateral ovaries replaced by fibrous streak gonads (no follicles identified)
- Echocardiography: Coarctation of aorta confirmed; bicuspid aortic valve noted
- Renal ultrasound: Horseshoe kidney identified
- Bone age X-ray: Delayed bone age (~14 years)
- DEXA scan: Low bone mineral density (Z-score: -2.1) - osteopenia
Other Investigations
- Fasting blood sugar: Normal
- Hearing test: Mild bilateral sensorineural hearing loss
- Liver function, renal function: Normal
Diagnosis
Turner Syndrome (45,X karyotype) presenting as Primary Amenorrhea with Hypergonadotropic Hypogonadism
- Coarctation of aorta + bicuspid aortic valve
- Horseshoe kidney
- Autoimmune hypothyroidism (Hashimoto's thyroiditis)
- Osteopenia
- Mild bilateral sensorineural hearing loss
Pathophysiology (Summary)
- No estrogen surge → no breast development, no endometrial proliferation
- No positive feedback on LH → no ovulation, no progesterone → primary amenorrhea
- No estrogen → poor bone mineralization → osteopenia
Management Plan
1. Hormone Replacement Therapy (HRT) - Priority
- Begin with low-dose estrogen (ethinyl estradiol 5-10 mcg/day orally or transdermal estradiol 0.5 mg/day) to induce puberty gradually
- After 12-18 months or with breakthrough bleeding, add cyclic progestogen (medroxyprogesterone acetate 5-10 mg for 10-12 days/month) to protect the uterus
- Continue HRT until the natural age of menopause (~50 years)
2. Cardiac Management
- Refer to cardiology for surgical repair/intervention for coarctation of aorta
- Echocardiography every 3-5 years; cardiac MRI for aortic surveillance
- Blood pressure control
3. Thyroid Management
- Start levothyroxine for subclinical hypothyroidism
- Annual TSH monitoring
4. Bone Health
- Calcium (1000-1300 mg/day) and Vitamin D (600-800 IU/day) supplementation
- Repeat DEXA scan in 2 years
5. Renal Follow-up
- Urological referral for horseshoe kidney
- Annual blood pressure monitoring and renal function tests
6. Fertility Counseling
- Naturally conceived pregnancy is nearly impossible due to streak ovaries
- Oocyte donation with IVF is the main option for future pregnancy
- Pre-pregnancy cardiac assessment is mandatory given aortic risk
7. Psychological Support
- Counseling regarding diagnosis, body image, and fertility
- Support groups for Turner syndrome
8. Hearing
- Audiological follow-up; hearing aids if needed
Prognosis
- With estrogen replacement therapy, secondary sexual characteristics will develop and menstrual cycles can be induced
- Cardiovascular anomalies (especially coarctation of the aorta and aortic dissection) are the leading cause of premature mortality and require lifelong surveillance
- Intelligence is usually normal; fertility is severely reduced but not impossible with assisted reproductive technology
- Regular screening for diabetes, hypertension, and aortic enlargement is needed lifelong