Positive findings & PG level assessment for Parkinson's disease & explain anatomy ,types & pathology of disease & difference between parkinson's & parkinsonism
"Parkinson disease"[MeSH Terms] AND diagnosis
Parkinson's disease positive findings clinical signs PG level assessment pathology 2025
Parkinson's Disease - Complete Clinical Review
1. Anatomy Relevant to Parkinson's Disease
The Basal Ganglia Circuit
- Pars compacta (SNpc): contains melanin-pigmented dopaminergic neurons that project to the striatum via the nigrostriatal pathway - this is the primary site of neurodegeneration in PD
- Pars reticulata (SNpr): a GABAergic output nucleus of the basal ganglia
- Direct pathway: striatum → GPi/SNpr → thalamus → cortex (facilitatory; uses D1 receptors, activated by dopamine)
- Indirect pathway: striatum → GPe → subthalamic nucleus (STN) → GPi/SNpr → thalamus → cortex (inhibitory; uses D2 receptors, inhibited by dopamine)
- Olfactory bulb and enteric nervous system (early; stages 1-2)
- Locus coeruleus, dorsal raphe, dorsal motor nucleus of vagus (stages 1-2)
- Substantia nigra and basal forebrain (stages 3-4 - symptomatic phase)
- Limbic cortex, neocortex (late stages 5-6)
2. Types of Parkinson's Disease
A. Idiopathic (Primary) Parkinson's Disease
| Subtype | Features | Prognosis |
|---|---|---|
| Tremor-dominant | Prominent rest tremor, slow progression | Slower disease course, longer levodopa benefit |
| Akinetic-rigid | Bradykinesia + rigidity dominate, minimal tremor | Faster progression |
| Mixed/Postural instability & gait difficulty (PIGD) | Prominent gait freeze, falls | More rapid decline, worse prognosis |
B. Genetic Forms of PD
| Gene | Locus | Inheritance | Notes |
|---|---|---|---|
| SNCA (α-synuclein) | 4q21 | Autosomal dominant | First PD gene identified; protein aggregates as Lewy bodies |
| LRRK2 (leucine-rich repeat kinase 2) | 12q12 | Autosomal dominant | Most common cause of late-onset familial PD |
| Parkin (PARK2) | 6q26 | Autosomal recessive | Most common early-onset (<40 yrs) |
| PINK1 | 1p36 | Autosomal recessive | Mitochondrial dysfunction |
| DJ-1 (PARK7) | 1p36 | Autosomal recessive | Rare; oxidative stress mechanism |
| GBA | 1q22 | Risk factor | Glucocerebrosidase; increased PD susceptibility |
3. Positive Findings in Parkinson's Disease
Cardinal Motor Signs (TRAP)
- Characteristic 4-6 Hz "pill-rolling" rest tremor
- Appears when limb is fully at rest; disappears with voluntary movement
- Asymmetric onset (typically one hand)
- Re-emergent postural tremor (appears after a latency of a few seconds when arms are outstretched)
- Velocity-independent lead-pipe resistance to passive movement
- Cogwheel rigidity: tremor superimposed on rigidity, gives a ratchet-like quality
- Present at wrist, elbow, neck; tested by passive joint movement
- Froment's maneuver (contralateral voluntary movement amplifies rigidity on the tested side - positive finding)
- Slowness of movement (bradykinesia) with progressive decrement in speed and amplitude on repetitive movements
- Assessed by finger tapping, hand opening/closing, foot tapping
- Hypomimia: masked/poker face, reduced blinking (2-10/min vs normal 12-20/min)
- Hypophonia: soft, monotone voice
- Micrographia: progressively smaller handwriting
- Hypodiadochokinesia: impaired rapid alternating movements
- Pull test (Retropulsion test): examiner pulls patient backward by shoulders; patient fails to take a corrective step or falls - strongly positive in PD
- Usually a late feature (if early, suggests atypical parkinsonism)
Other Positive Clinical Findings
- Festination: shuffling gait with short steps, accelerating to keep up with shifted centre of gravity
- Reduced arm swing (often unilateral early)
- Freezing of gait (FOG): sudden inability to initiate or continue walking
- Camptocormia: abnormal forward flexion of thoracolumbar spine
- Procerus sign (furrowing between brows): more typical of PSP; PD shows hypomimia instead
- Seborrhoeic dermatitis over face
- Orthostatic hypotension
- Constipation (often precedes motor symptoms by years)
- Urinary dysfunction
- Hyperhidrosis
- Sialorrhoea (drooling)
- Hyposmia/anosmia (often precedes motor symptoms; one of earliest markers)
- REM Sleep Behavior Disorder (RBD): acting out dreams; a major prodromal feature
- Depression and anxiety
- Cognitive impairment / dementia (Parkinson's disease dementia, PDD)
- Visual hallucinations (later stage)
- Pain and sensory symptoms
4. PG Level Assessment (Prognostic Grading / Clinical Scales)
A. Hoehn and Yahr Scale (H&Y)
| Stage | Description |
|---|---|
| Stage I | Unilateral involvement only; minimal or no functional impairment |
| Stage II | Bilateral or midline involvement; no impairment of balance |
| Stage III | First sign of impaired righting reflex (positive pull test); mild-moderate disability; physically independent |
| Stage IV | Fully developed, severely disabling disease; patient still able to walk/stand unassisted |
| Stage V | Confinement to bed or wheelchair unless aided |
B. MDS-UPDRS (Movement Disorder Society - Unified Parkinson's Disease Rating Scale)
| Part | What it Measures |
|---|---|
| Part I | Non-motor aspects of daily living (mentation, behavior, mood) |
| Part II | Motor aspects of daily living (ADL impairment) |
| Part III | Motor examination (clinician-scored; tremor, rigidity, bradykinesia, gait, postural stability) |
| Part IV | Motor complications (dyskinesia, fluctuations) |
C. Mini-Mental State / MoCA
D. Schwab & England ADL Scale
5. Pathology of Parkinson's Disease
Macroscopic Pathology
- Depigmentation of the substantia nigra: loss of melanin-containing neurons causes visible pallor of the SN in cross-sections of the midbrain (compared to the normal dark appearance)
- Pallor also seen in the locus coeruleus
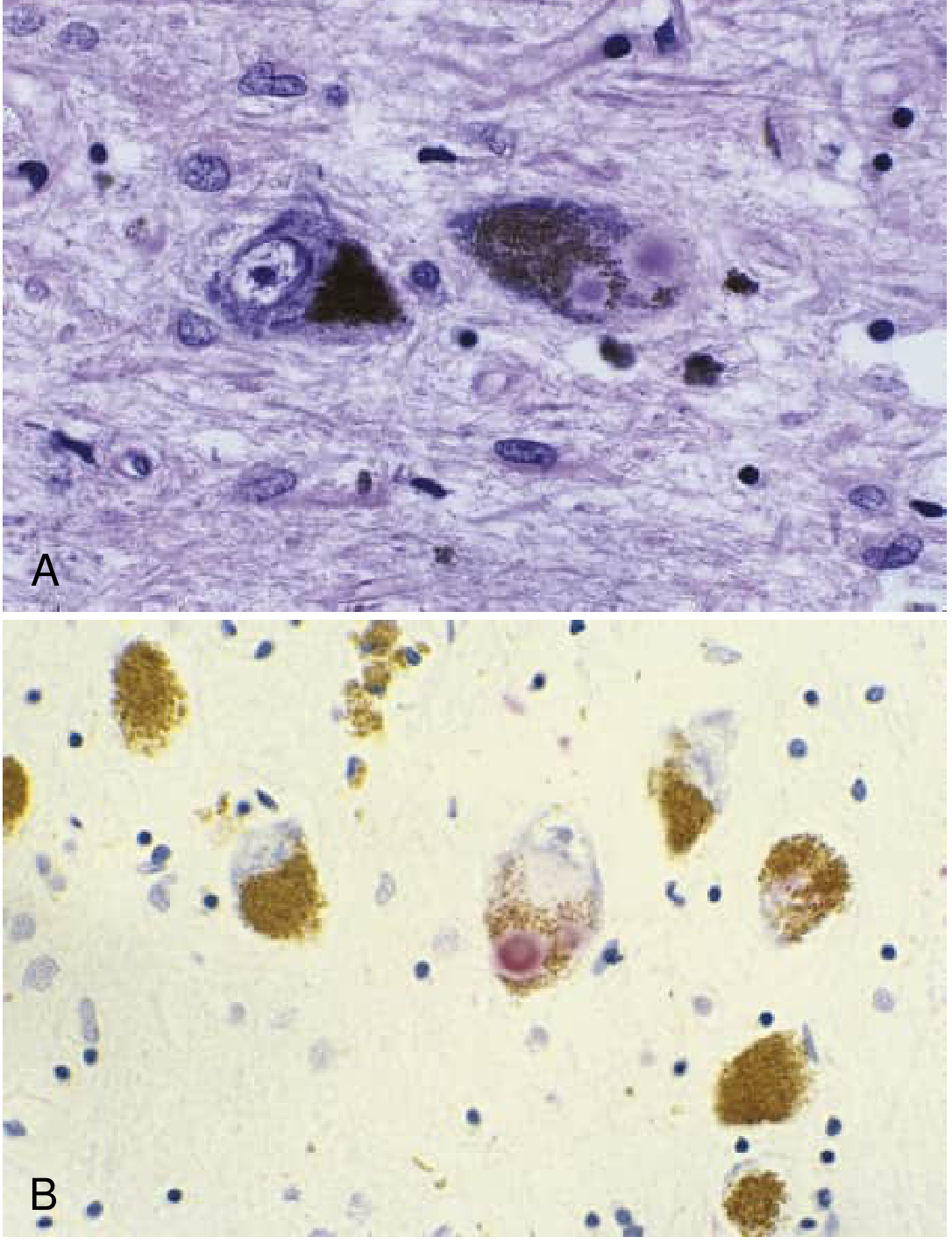
Microscopic Pathology
- Selective loss of dopaminergic neurons in the SNpc (60-80% lost before symptoms appear)
- Remaining neurons show degenerative changes
- Intraneuronal, round, eosinophilic cytoplasmic inclusions with a pale halo
- On H&E: dense core (eosinophilic, 5-25 µm) surrounded by a clear halo, displacing neuromelanin
- Composed of: α-synuclein (major protein), ubiquitin, neurofilaments, proteasome components
- On α-synuclein immunostaining: stain intensely red/brown
- Found in SNpc, locus coeruleus, dorsal vagal nucleus, cortex (in PDD)
- Abnormal, dystrophic neuritic processes containing α-synuclein aggregates
- Found in the CA2/3 region of the hippocampus and elsewhere
- Astrocytic gliosis in areas of neuronal loss
Braak Staging of PD Pathology
| Stage | Location of Lewy Pathology | Clinical Correlate |
|---|---|---|
| 1-2 | Olfactory bulb, dorsal motor nucleus of vagus, enteric NS | Anosmia, constipation, RBD (prodrome) |
| 3-4 | Substantia nigra, basal forebrain, amygdala | Motor symptoms begin |
| 5-6 | Limbic cortex → neocortex | Dementia, psychosis |
Neurochemical Pathology
| Neurotransmitter | Change | Circuit Effect |
|---|---|---|
| Dopamine | Severely reduced in striatum (>80% at symptom onset) | Bradykinesia, rigidity, tremor |
| Norepinephrine | Reduced (locus coeruleus loss) | Autonomic dysfunction, depression |
| Serotonin | Reduced (raphe nuclei) | Depression, mood changes |
| Acetylcholine | Reduced (nucleus basalis of Meynert) | Dementia, cognitive decline |
6. Parkinson's Disease vs. Parkinsonism - Key Differences
| Feature | Parkinson's Disease (PD) | Parkinsonism |
|---|---|---|
| Definition | A specific neurodegenerative disease caused by idiopathic dopaminergic loss with Lewy body pathology | A clinical syndrome of bradykinesia + rigidity ± tremor ± postural instability, from ANY cause |
| Relationship | PD IS a form of parkinsonism (most common cause; ~80%) | Parkinsonism is the umbrella term; PD is a subtype |
| Pathology | Lewy bodies (α-synuclein) + SNpc degeneration | Varies by cause; no Lewy bodies in most secondary forms |
| Onset | Asymmetric; unilateral at onset | Often bilateral/symmetric at onset (atypical or secondary forms) |
| Tremor | Prominent 4-6 Hz resting tremor | Minimal or absent in most atypical and secondary forms |
| Levodopa response | Excellent (70-100%) initially | Poor or absent (atypical); good (drug-induced, after withdrawal) |
| Progression | Slow (years to decades) | Faster in atypical forms |
| Postural instability | Late feature | Early prominent feature in PSP, MSA |
| Dementia | Late feature (PDD) or with DLB spectrum | Early in DLB, PSP |
| Brain imaging (MRI) | Normal on standard imaging | Abnormal in many: midbrain atrophy (PSP), putaminal atrophy (MSA), white matter lesions (vascular) |
| DAT scan | Reduced (asymmetric) | Reduced in neurodegenerative forms; normal in drug-induced/functional |
Causes of Parkinsonism (Non-PD)
| Condition | Key Distinguishing Features |
|---|---|
| Progressive Supranuclear Palsy (PSP) | Vertical supranuclear gaze palsy, axial (nuchal) rigidity > limb, early falls backward, Procerus sign ("astonished look"), midbrain atrophy ("hummingbird sign" on MRI) |
| Multiple System Atrophy (MSA) | Profound early dysautonomia, cerebellar signs (MSA-C), anterocollis, no/poor levodopa response, "hot cross bun sign" on MRI |
| Corticobasal Degeneration (CBD) | Alien limb, cortical sensory loss, apraxia, limb dystonia, asymmetric fronto-parietal atrophy on MRI |
| Dementia with Lewy Bodies (DLB) | Cognitive decline preceding/co-emerging with parkinsonism, early visual hallucinations, neuroleptic sensitivity, RBD, fluctuating cognition |
| Cause | Key Feature |
|---|---|
| Drug-induced | Onset during offending drug (antipsychotics, metoclopramide, reserpine); improves after withdrawal |
| Vascular (VP) | Lower body predominance, pyramidal signs, white matter lesions/lacunar infarcts on MRI, stepwise progression |
| Post-infectious/Encephalitis lethargica | History of encephalitis, oculogyric crises |
| Toxic | MPTP (meperidine analog), manganese, carbon monoxide exposure |
| Normal Pressure Hydrocephalus (NPH) | Gait apraxia + dementia + urinary incontinence triad; communicating hydrocephalus on CT/MRI |
| Wilson's disease | Young age, Kayser-Fleischer rings, liver disease, low ceruloplasmin |
7. Diagnostic Criteria Summary (MDS Clinical Criteria)
- Absence of absolute exclusion criteria
- At least two supportive criteria
- No red flags
- Unilateral onset
- Clear and dramatic response to levodopa (70-100%)
- Levodopa-induced dyskinesia
- Rest tremor
- Hyposmia or loss of smell
- Cardiac sympathetic denervation on MIBG scintigraphy
- Presence of Lewy bodies on biopsy (definitive)
- Unequivocal cerebellar features
- Downward vertical supranuclear gaze palsy
- Frontotemporal dementia within first 5 years
- Purely lower-limb parkinsonism for >3 years
- No response to levodopa despite adequate dose
- Cortical sensory loss, alien limb
Recent Evidence Note
- Bradley and Daroff's Neurology in Clinical Practice (9780323642613)
- Adams and Victor's Principles of Neurology, 12th Edition (9781264264520)
- Harrison's Principles of Internal Medicine 22E (9781265977061)
- MDS Clinical Diagnostic Criteria for Parkinson's Disease (Postuma et al., 2015)
Explain to me types in detail & how to diagnose those types clinically & then give me management for same or clinical feature wise (make a short term & long term goals & then give me management)
"Parkinson disease"[MeSH Terms] AND management AND treatment
PSP MSA CBD DLB clinical diagnosis features management guidelines 2024 2025
https://practicalneurology.com/diseases-diagnoses/movement-d…
What Was Covered
Part 1 - Types in Detail (7 types)
- Idiopathic PD - with 4 motor subtypes (Tremor-dominant, Akinetic-Rigid, PIGD, Young-onset)
- PSP - 5 phenotypes, MDS OPAC diagnostic framework, hummingbird sign
- MSA - MSA-P vs MSA-C, autonomic criteria, hot cross bun sign
- CBD/CBS - alien limb, asymmetric rigidity, apraxia, cortical sensory loss
- DLB - McKeith criteria, fluctuating cognition, RBD, neuroleptic sensitivity
- Drug-Induced Parkinsonism - symmetric, reversible, normal DAT scan
- Vascular Parkinsonism - lower body predominance, pyramidal signs, MRI white matter changes
Part 2 - Goals
- Short-term: motor control, fall prevention, ADL independence, dysphagia screening, education
- Long-term: delay motor complications, manage dementia/autonomic/psychiatric features, DBS candidacy, advance care planning
Part 3 - Management
- Drug-wise: Levodopa, DAs, MAO-B inhibitors, COMT inhibitors, Amantadine, Anticholinergics - each with mechanism, indication, and when to use
- Feature-wise: tremor, rigidity, gait/freezing, speech, dysphagia, depression, psychosis, RBD, constipation, orthostatic hypotension
- Atypical types: individual management tables for PSP, MSA, CBD, DLB, DIP, Vascular
- Non-pharmacological: MDT roles, exercise evidence (2024 Cochrane), LSVT, PT/OT/SLT
- Palliative: late-stage goals including aspiration management and advance care planning
Typical physiotherapy management
"Parkinson disease"[MeSH Terms] AND "physical therapy"[MeSH Terms]
physiotherapy management Parkinson's disease evidence based guidelines 2024 2025 NICE European
"Parkinson disease" AND "exercise" AND "balance" AND rehabilitation
https://www.nature.com/articles/s41531-026-01326-7
PMID: 38588457
PMID: 38897907
PMID: 37641007
"Parkinson disease" AND "treadmill" OR "tai chi" OR "dance" AND "gait" rehabilitation
Physiotherapy Management of Parkinson's Disease
Overview and Rationale
Physiotherapy Assessment Framework
| Domain | Assessment Tool |
|---|---|
| Motor severity | MDS-UPDRS Part III, Hoehn and Yahr stage |
| Balance | Berg Balance Scale (BBS), Mini-BESTest, Functional Reach Test |
| Gait | Timed Up and Go (TUG), 10-metre walk test, 6-minute walk test |
| Falls risk | Falls history, Dynamic Gait Index, ABC Scale (Activities-specific Balance Confidence) |
| Freezing of gait | Freezing of Gait Questionnaire (FOG-Q) |
| Functional mobility | Functional Independence Measure (FIM), Barthel Index |
| Posture | Visual postural analysis; kyphosis/camptocormia measurement |
| Muscle strength | Manual muscle testing; grip dynamometry |
| Flexibility | ROM at trunk, hip, shoulder |
| Respiratory | Peak flow, chest expansion (relevant in late stage) |
| Cognitive | MoCA (influences therapy delivery) |
Physiotherapy Goals
Short-Term Goals (4-12 weeks)
| Goal | Target Outcome |
|---|---|
| Improve gait pattern | Increase step length, walking speed, arm swing |
| Reduce fall risk | Improve reactive and proactive balance responses |
| Improve transfers | Sit-to-stand, bed mobility, rolling |
| Reduce rigidity | Improve range of motion through stretching and active exercise |
| Improve posture | Reduce kyphosis; improve axial extension |
| Patient education | Teach home exercise program; cueing strategies; fall prevention |
| Improve confidence | Reduce fear of falling; improve self-efficacy |
Long-Term Goals (Months to Years)
| Goal | Target Outcome |
|---|---|
| Slow functional decline | Maintain independence in ambulation and ADLs as long as possible |
| Prevent complications | Reduce falls, contractures, pressure injuries, aspiration |
| Maintain cardiovascular fitness | Reduce deconditioning; promote neuroprotective exercise |
| Manage disease progression | Adapt program as disease advances through stages |
| Caregiver training | Teach safe handling, transfers, cueing techniques |
| Advance to assistive devices | Timely introduction of walking aids when indicated |
Core Physiotherapy Interventions
1. Gait Training
A. Treadmill Training
- One of the most well-studied interventions
- Body-Weight Supported Treadmill Training (BWS-TT): rated highest for improving overall balance scores (BBS p-score 0.97) and dynamic steady-state balance in a 2023 network meta-analysis of 24 exercise types (PMID 37641007)
- Provides a rhythmic, forced pace that bypasses the basal ganglia deficit
- Improves walking speed, stride length, endurance
- Protocol: typically 3x/week, 20-30 min sessions, moderate intensity
B. Overground Gait Training
- Focus on attentional strategies: "big steps," "high steps," "swing arms"
- Lee Silverman Voice Treatment BIG (LSVT BIG): translates the amplitude-focused LSVT principle to whole-body movements - patients trained to take LARGE movements; improves gait and motor function
C. Cueing Strategies
| Cue Type | Method | Evidence |
|---|---|---|
| Auditory cueing | Metronome beat; music with rhythmic beat; verbal rhythm ("1-2-3-step") | BEST EVIDENCE: auditory cueing + walking training improves walking speed by +0.09 m/s more than walking training alone (PMID 38897907) |
| Visual cueing | Floor stripes (3-5 cm bands at step-length intervals); laser pointer on walking frame; transverse lines on floor | Helps initiate stepping; improves step length; useful for FOG |
| Attentional strategies | Conscious focus on step size ("think big step") | Overrides defective automatic movement generation |
| Somatosensory cueing | Rhythmic vibration on wrist; tactile metronome | Emerging evidence; adjunct |
D. Freezing of Gait (FOG) Strategies
- Mental imagery before stepping: visualise a large stride before moving
- Step-over obstacle: laser pointer on walking frame; stepping over imaginary line
- Counting or marching in place before initiating
- Shifting weight: rock side to side to initiate stepping
- Backward walking: can paradoxically unfreeze some patients
- Environmental modifications: remove rugs, clutter; widen doorways; avoid narrow spaces
2. Balance Training
A. Static Balance Exercises
- Narrow base of support standing (feet together)
- Single-leg stance (with support as needed)
- Tandem standing
- Standing on foam/unstable surface (proprioceptive challenge)
B. Dynamic Balance Exercises
- Weight shifting: side-to-side and forward-backward
- Stepping in all directions
- Reaching tasks (moving centre of gravity outside base of support)
- Functional reach training
C. Reactive Balance / Perturbation Training
- Therapist applies unexpected perturbations to the patient while standing
- Patient practices rapid stepping responses
- Evidence suggests reactive balance training specifically reduces fall frequency
- BGT-ECA (Balance and Gait Training with External Cue or Attention) - top ranked for reactive balance (PMID 37641007)
D. Dual-Task Training
- PD patients are highly susceptible to dual-task interference (walking + talking = falls)
- Training: practice balance/walking while performing cognitive tasks (counting backwards, carrying a tray)
- Gradually progress cognitive challenge
- Motor-cognitive dual-task training improves both gait and cognition
E. Technology-Assisted Balance
- Wii Fit / Balance Board: visual biofeedback of centre of pressure; engaging and motivating
- Robotic-assisted gait and balance (RA-GT): top-ranked for reactive balance (PMID 37641007)
- Virtual reality (VR): immersive environments for obstacle avoidance, balance challenges
3. Strengthening Exercises
- Lower limb strengthening: squats, sit-to-stand, step-ups, leg press, calf raises
- Trunk stabilisation: core exercises (bridges, dead bug, bird-dog), particularly important for camptocormia/Pisa syndrome
- Upper limb: shoulder external rotation, rowing exercises (counteract the flexed stooped posture)
- Resistance training: 2024 Cochrane (PMID 38588457) - small but meaningful improvement in UPDRS motor scores (MD -4.96 vs passive control)
- Frequency: 2-3x/week; 2-3 sets of 8-15 repetitions; progressive overload
4. Flexibility and Stretching
- Active and passive ROM exercises for all major joints
- Trunk rotation exercises: rotational movements in lying, sitting, standing
- Chest wall stretches: doorway stretches, thoracic extension over foam roller
- Hip flexor stretches: lunge position
- Postural correction: shoulder retraction, scapular squeezes, chin tucks
- Yoga: systematic review evidence supports yoga for rigidity, flexibility, and quality of life in PD
- Timing: best performed during medication "on" phase when rigidity is reduced
5. Postural Training
- Thoracic extension exercises over foam roller
- Wall standing: standing with back against wall; practice maintaining upright posture
- Mirror feedback: patient observes and corrects posture in mirror
- Taping techniques: kinesiotaping to facilitate erect posture
- McKenzie extension exercises (adapted)
- Scapular stabilisation program
- Body awareness training: Feldenkrais, Alexander Technique
- For severe camptocormia: thoracolumbar orthosis (TLSO) as adjunct
6. Transfers and Functional Mobility
Sit-to-Stand
- Move to edge of seat first
- Feet hip-width apart, tuck feet under chair
- Lean forward ("nose over toes")
- Push through arms and legs simultaneously
- Verbal counting cue to initiate ("1-2-3-up")
- Chair height modifications (raised seat cushion)
Bed Mobility
- Log roll technique: bend knees, arms crossed, roll to side
- Push up to sitting from side-lying
- Satin/silk sheets to reduce friction during turning in bed
- Bed rails or rope ladder if needed
Floor Rise
- Essential life skill to address early
- Sequence: roll to side → hands and knees → step one foot up → use chair to push to standing
- Practise regularly; family to be taught also
Car Transfers
- Swivel cushion for car seat
- Grab handles; avoiding low sports car seats
7. Aerobic / Cardiovascular Exercise
- Cycling: stationary cycling (including forced-rate cycling at higher cadence than voluntary); improvements in motor symptoms
- Walking programs: regular brisk walking; Nordic walking (poles improve posture and arm swing)
- Swimming: aquatic exercise - ranked highly for static balance (sSSB, p-score 0.85; PMID 37641007); water buoyancy reduces fall risk, allows larger movements
- Dance: strongest evidence for motor signs in 2024 Cochrane NMA - UPDRS-M MD -10.18 (dance ranked FIRST; moderate confidence); tango has most evidence among dance forms; Irish set dancing, ballroom also studied
- Tai Chi: high-quality evidence for balance and fall reduction; improves reactive balance; accessible and enjoyable
- Target: ≥150 minutes/week moderate-intensity aerobic activity (WHO/NICE recommendation)
8. Respiratory Physiotherapy
- Diaphragmatic breathing exercises: deep belly breathing; pursed lip breathing
- Inspiratory muscle training (IMT): threshold device (eg Threshold IMT); improves inspiratory muscle strength
- Active cycle of breathing technique (ACBT): for secretion clearance
- Thoracic mobility exercises: rotational and lateral flexion
- Postural drainage (if secretions present)
- Huffing and assisted cough: important in late-stage disease
9. Aquatic Physiotherapy (Hydrotherapy)
- Warm water (34-36°C) reduces rigidity and facilitates movement
- Buoyancy support allows balance training with reduced fall risk
- Hydrostatic pressure assists proprioception
- Exercises: walking in water, stepping, balance challenges, rotation, swimming
- Aquatic exercise ranked top for improving static steady-state balance (PMID 37641007)
- Particularly useful for patients with severe postural instability or fear of falling
10. Mind-Body Therapies
| Approach | Evidence | Notes |
|---|---|---|
| Tai Chi | Strong - reduces falls, improves balance (Li et al., 2012) | 2x/week recommended; improves reactive balance particularly |
| Yoga | Moderate - improves flexibility, rigidity, quality of life, balance | Evidence supports adapted yoga; requires modification for PD posture |
| Dance (Tango) | Strongest motor evidence in Cochrane 2024 NMA | Social engagement benefit; improves rhythm, balance, dual-tasking |
| Pilates | Top-ranked for proactive balance (p-score 0.95; PMID 37641007) | Core strengthening; postural control |
| Qi Gong | Moderate - balance and well-being | Related to Tai Chi |
| Feldenkrais | Small studies - body awareness, posture | |
| Alexander Technique | Small evidence - postural re-education |
11. Home Exercise Programme (HEP)
- 2023 meta-analysis (PMID 38114897): home-based exercise improves motor symptoms, quality of life, and functional performance significantly vs control
- Components: stretching, strengthening, balance, walking, breathing
- Frequency: daily practice preferred; minimum 5 days/week
- Technology: smartphone apps (Parkinson's Exercise: PD Warrior), YouTube programs, Nintendo Wii/games
- Caregiver involvement in monitoring and assistance
- Review and progress every 4-8 weeks
Stage-Based Physiotherapy Approach
| H&Y Stage | Main Problems | Physiotherapy Focus |
|---|---|---|
| Stage 1-2 (Mild, unilateral) | Reduced arm swing, mild rigidity, early posture changes | Preventive exercise; aerobic fitness; postural correction; education; HEP |
| Stage 2.5-3 (Moderate) | Balance impairment, bilateral symptoms, early gait changes | Balance training; cueing for gait; transfer training; fall prevention; strengthening |
| Stage 3-4 (Moderate-Severe) | Frequent falls, FOG, postural instability, transfer difficulty | Reactive balance; FOG strategies; assistive device prescription; carer training; respiratory PT |
| Stage 5 (Severe, wheelchair/bedbound) | Immobility, contractures, pressure injuries, aspiration | Passive ROM; positioning; chest PT; pressure area care; carer education; palliative focus |
Assistive Devices and Equipment
| Device | Indication |
|---|---|
| Walking poles / Nordic walking poles | Mild-moderate gait disorder; improves posture and arm swing |
| Rollator (wheeled walking frame with brakes) | Moderate gait disorder; FOG - some models have laser line projector attached |
| Weighted walker | PSP (where retrocollis/backward falling is the problem) |
| Laser cane / walking frame with laser | Provides a visual cue line to step over; reduces FOG |
| Raised toilet seat | Difficulty with sit-to-stand from toilet |
| Grab rails | Bathroom, stairs, bedside |
| Recliner / high-seat chair | Easier sit-to-stand |
| Satin sheets | Night-time turning difficulty |
| Cushioned insoles | Foot dystonia / striatal deformity |
Physiotherapy in Atypical Parkinsonism
| Condition | Key PT Focus | Special Considerations |
|---|---|---|
| PSP | Prevent backward falls (retrocollis); use weighted walker (counteracts backward pull); transfer training; early introduction of seating adaptations | Do NOT use rollator (backward fall risk); patient tends to fall BACKWARD |
| MSA | Manage orthostatic hypotension before exercise (gradual position changes); balance and gait; respiratory PT for stridor/sleep apnea | Compression garments before standing; shorter sessions due to autonomic intolerance |
| CBD/CBS | Alien limb management (mirror therapy, splinting); apraxia retraining; asymmetric balance training; ADL retraining with unaffected limb | Functional goal-setting critical as motor function is very asymmetric |
| DLB | Cognitive engagement during PT; avoid complex dual-task (cognitive fluctuations); fall prevention; gentle exercise | Adapt to cognitive fluctuations; avoid high-stimulation environments |
Multidisciplinary Integration
- Physiotherapy + Speech-Language Therapy (LSVT LOUD for voice; LSVT BIG for movement - these are linked programmes)
- Physiotherapy + Occupational Therapy (ADL integration of movement gains)
- Physiotherapy + Neurologist (timing PT sessions in medication "on" phase for maximum benefit)
- Physiotherapy + Dietitian (nutritional support for exercise; weight management)
- ParkinsonNet model (Netherlands): specialist PT network trained specifically in PD - associated with better outcomes and lower healthcare costs
Evidence Summary Table
| Intervention | Best Outcome | Evidence Level | Key Reference |
|---|---|---|---|
| Dance | Motor signs (UPDRS-M MD -10.18) | Moderate confidence | PMID 38588457, Cochrane 2024 |
| Gait/Balance/Functional training | Motor signs (UPDRS-M MD -7.50) | Moderate confidence | PMID 38588457, Cochrane 2024 |
| BWS Treadmill | Overall balance (BBS p-score 0.97) | Low-moderate | PMID 37641007 |
| Aquatic exercise | Static steady-state balance | Low-moderate | PMID 37641007 |
| Pilates | Proactive balance (p-score 0.95) | Low | PMID 37641007 |
| Auditory cueing + walking | Walking speed (+0.09 m/s) | Low | PMID 38897907 |
| Balance-specific training | Mini-BESTest, BBS, TUG | Moderate | npj Parkinson's 2026 |
| Home exercise | Motor + QoL + functional performance | Moderate | PMID 38114897 |
| Tai Chi | Balance, fall reduction | Moderate | Li et al. 2012 |
| Multi-domain training | Motor signs (UPDRS-M MD -5.90) | Moderate | PMID 38588457 |
Key Clinical Tips for Physiotherapists
- Time sessions during medication "on" phase - typically 45-90 minutes after levodopa dose; motor performance is significantly better during "on"
- Start early - physiotherapy in early PD has better long-term outcomes than starting late; neuroprotective exercise principles apply
- High intensity when possible - forced-rate exercise (cycling at cadence above voluntary maximum) shows particular benefit; intensity appears important
- Progress the programme - static → dynamic → dual-task → perturbation; continue adding challenge
- Group sessions - peer motivation; social engagement; cost-effective; evidence supports group exercise formats
- Avoid over-fatigue - PD patients tire easily; balance effort with rest; monitor for medication wearing-off during sessions
- Educate family and carers - cueing strategies, transfer assistance, fall response should be taught to carers
- Fear of falling is common and disabling - address psychological component alongside physical; graded exposure to challenging situations
- Adams and Victor's Principles of Neurology, 12th Edition
- European Physiotherapy Guideline for Parkinson's Disease (ParkinsonNet, 2014 - still primary reference)
- ANPT Clinical Practice Guideline for Physical Therapist Management of Parkinson Disease (2022)
- Cochrane NMA on Exercise in PD (PMID 38588457, 2024)
- Network meta-analysis of 24 exercise types (PMID 37641007, 2023)
- Auditory cueing systematic review (PMID 38897907, 2024)
- npj Parkinson's Disease balance physiotherapy dose-response meta-analysis (2026)