In detail about myasthenia Gravis
Reading File
Finding Sources
Searching PubMed
"myasthenia gravis"[MeSH Terms] AND treatment
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
I now have enough comprehensive information to write a thorough, detailed response. Let me compile everything.
Myasthenia Gravis (MG) - Comprehensive Overview
Definition
Acquired Myasthenia Gravis is the most common primary disorder of neuromuscular transmission (NMT). In MG, autoantibodies binding to proteins at the neuromuscular junction (NMJ) - most commonly the acetylcholine receptor (AChR) - disrupt normal NMT. This results in muscle weakness that fluctuates with effort and rest, and that typically predominates in specific muscle groups. The NMJ is particularly vulnerable to autoimmune attack because it lacks a blood-nerve barrier.
- Bradley and Daroff's Neurology in Clinical Practice, p. 2769
Epidemiology
-
US prevalence: approximately 20 per 100,000 (~60,000 patients total)
-
Prevalence has been increasing over the past 50 years, largely due to better ascertainment, reduced mortality, and an aging population
-
Sex and age patterns:
- Women are affected ~3 times more often than men before age 40
- Men have higher incidence after age 50
- Roughly equal incidence during puberty
- Mean age of onset: women 28-35 years; men 42-49 years
- Today, the majority of US MG patients are over age 50
-
Bradley and Daroff's Neurology, p. 2769
Pathophysiology
The Neuromuscular Junction
Normal muscle contraction requires efficient transmission of an electrical impulse from a motor axon to its muscle fibers via the NMJ - a specialized synapse where acetylcholine (ACh) is released, binds to nicotinic AChRs on the postsynaptic membrane, and generates a muscle action potential.
Autoantibody Mechanisms
MG involves autoantibodies targeting postsynaptic proteins. Three main mechanisms damage the NMJ:
- Direct blockade - Antibodies block ACh binding sites, preventing ion channel opening
- Cross-linking and internalization - Divalent antibodies cross-link AChRs, accelerating their internalization and degradation (antigenic modulation)
- Complement-mediated lysis - Complement activation destroys the postjunctional membrane and reduces AChR number
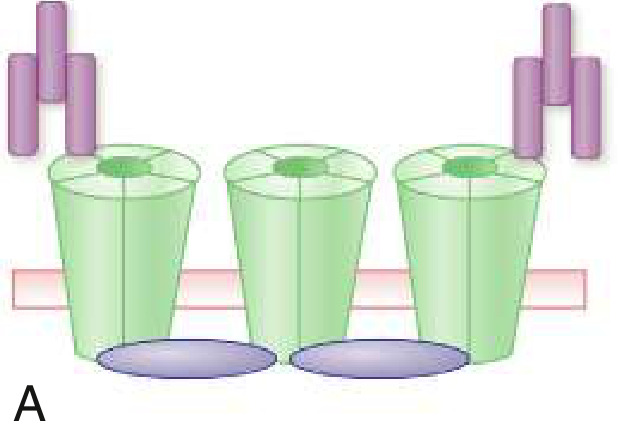
Fig: Mechanisms by which AChR antibodies damage the postsynaptic membrane - Goldman Cecil Medicine, p. 4111
Target Antigens
| Antibody | Prevalence | Mechanism |
|---|---|---|
| Anti-AChR (α1 subunit) | ~85% GMG | Complement activation, modulation, direct blockade |
| Anti-MuSK (muscle-specific kinase) | Up to 50% of AChR-negative GMG | IgG4 - blocks signals that concentrate AChRs at NMJ |
| Anti-LRP4 (lipoprotein receptor-related protein 4) | Minority | Interferes with NMJ integrity signals |
| Agrin, cortactin | Rare | Less well characterized |
Role of the Thymus
-
In early-onset MG: thymic hyperplasia with germinal centers suggests immune tolerance breakdown is initiated in the thymus; autoreactive B cells persist even after thymectomy
-
In thymoma-associated MG: deficiency of the autoimmune regulatory protein AIRE leads to deficient regulatory T cells and increased autoreactivity; local expression of muscle antigens (including AChRs) within the thymoma activates autoreactive T cells
-
Goldman Cecil Medicine, p. 4111
Clinical Presentation
Patients present with fatigable weakness - muscle weakness that worsens with activity and improves with rest. This is the cardinal feature that distinguishes MG from other neuromuscular diseases.
Initial Symptoms (frequency)
- Ocular symptoms (ptosis, diplopia): initial symptom in ~66% of patients; virtually all develop both within 2 years
- Bulbar symptoms (dysphagia, dysarthria): initial symptom in ~16% of patients
- Limb weakness: initial symptom in ~10% of patients
- Respiratory failure as the initial symptom is rare
Ocular Manifestations
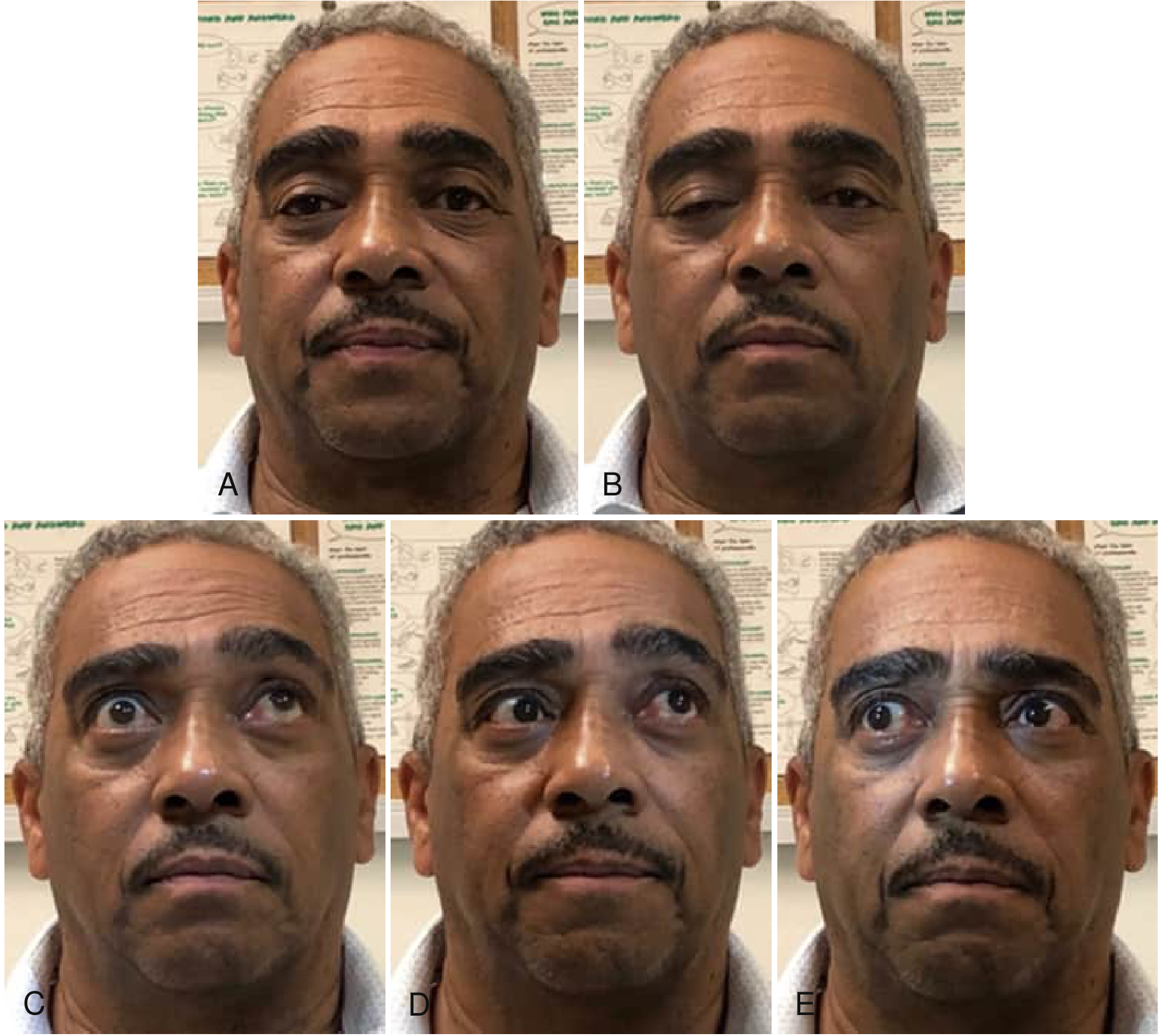
Fig. 108.1: Ocular motility abnormalities due to weakness of multiple periocular muscles - Bradley and Daroff's Neurology, p. 2770
- Ptosis can be unilateral or bilateral, variable throughout the day
- Diplopia results from asymmetric weakness of extraocular muscles
- Gaze can be restricted in any direction; the pattern mimics various third-nerve palsies or gaze palsies but does not conform to a single nerve pattern
- The enhanced ptosis sign: when the ptotic lid is manually elevated, the contralateral lid droops more (Cogan's lid twitch is also classic)
Bulbar Manifestations
- Dysphagia, dysarthria, fatigable chewing
- Pharyngeal phase involvement in virtually all patients with dysphagia (100% in one study)
- Silent aspiration occurs in ≥35% of MG patients with dysphagia
- Bulbar symptoms are a major precipitant of myasthenic crisis in 56% of cases
Respiratory Involvement
- Diaphragmatic and intercostal weakness can develop
- Most feared complication: myasthenic crisis (see below)
Classification / Subtypes
1. Ocular MG (OMG)
- Weakness confined to extraocular muscles and eyelids
- 10%-15% of MG in Caucasians; up to 58% in Asian populations
- If ocular weakness persists exclusively beyond 2 years - 90% probability it will not generalize
- Often seronegative; SFEMG required for confirmation
2. Generalized MG (GMG)
| Early-onset (EOMG, age <50) | Late-onset (LOMG, age >50) | |
|---|---|---|
| Sex | More often female | More often male |
| Antibodies | Anti-AChR | Anti-AChR + anti-titin/anti-ryanodine receptor |
| Thymus | Hyperplastic | Normal or atrophic |
| HLA | A1, B8, DRw3 (women) | A3, B7, DRw2.1 (men) |
3. Thymomatous MG
- ~10%-15% of MG patients have a thymoma
- Equal sex distribution; peak onset age 50
- Often have striated muscle antibodies (anti-titin, anti-ryanodine receptor)
- Removal of thymoma does not cure MG
4. MuSK-Antibody MG
- Found in up to 50% of AChR-negative GMG patients
- Predominantly affects females
- Clinically distinctive: prominent facial, bulbar, and neck weakness with muscle atrophy; less ocular involvement
- Geographic variation: higher incidence closer to the equator
- Responds poorly to acetylcholinesterase inhibitors; more responsive to rituximab
5. LRP4-Antibody MG
- Minority of seronegative patients
- Milder phenotype generally
6. Seronegative MG
- No detectable antibodies by standard assays
- May have low-affinity antibodies detectable by cell-based assays
Diagnostic Procedures
1. Antibody Testing
- AChR binding antibody assay (most widely used): sensitivity ~85% GMG, ~50% OMG; essentially confirms diagnosis when positive in compatible clinical setting
- AChR blocking antibody: lower sensitivity; <1% of patients test positive without also having binding antibodies
- AChR modulating antibody: ~10% of binding-antibody-negative patients are positive
- Anti-MuSK antibody: essential in AChR-negative patients with GMG
- Anti-LRP4 antibody: tested in seronegative patients after negative AChR and MuSK
- AChR-ab levels do not reliably predict disease severity or guide therapy
2. Electrodiagnostic Studies
- Repetitive nerve stimulation (RNS): Low-frequency (2-3 Hz) stimulation shows >10% decremental response in compound muscle action potential (CMAP) amplitude - a hallmark of postsynaptic NMJ disorder; sensitivity higher for proximal/bulbar muscles
- Single-fiber electromyography (SFEMG): Most sensitive test for NMJ dysfunction (>90% sensitivity); measures jitter (variability in interpotential interval between muscle fiber pairs); increased jitter and blocking are characteristic; essential for OMG and seronegative cases
3. Edrophonium (Tensilon) Test
- Edrophonium is a rapid, short-acting acetylcholinesterase inhibitor
- Positive in 60%-95% of OMG and 72%-95% of GMG patients
- Increasingly difficult to obtain; losing favor with widespread autoantibody availability
4. Imaging
- CT of the chest (with/without contrast) in all newly diagnosed MG: mandatory to evaluate for thymoma
- MRI of orbits/brain: to exclude orbital or brainstem lesions mimicking ocular MG
5. Pulmonary Function Tests
- Forced vital capacity (FVC) and negative inspiratory force (NIF) for monitoring respiratory compromise and guiding intubation decisions
Treatment
Treatment is individualized based on severity, antibody status, age, and comorbidities. Four main pillars:
Pillar 1: Symptomatic Treatment - Acetylcholinesterase Inhibitors
Pyridostigmine (Mestinon)
- First-line symptomatic agent
- Initial dose: 30-60 mg TID; titrate to 60-120 mg TID to 5x/day based on symptoms
- Maximum dose typically not exceeding 480 mg/day
- Onset: 15-30 minutes
- Side effects: cholinergic - GI cramps, nausea, diarrhea, sweating, increased secretions, muscle fasciculations
- Does not alter the underlying disease course; does not induce remission
- Less effective in MuSK-MG
Pillar 2: Long-Term Immunosuppression
| Drug | Starting Dose | Target Dose | Onset | Key Adverse Effects |
|---|---|---|---|---|
| Prednisone | 10-20 mg/day (slow escalation) or 50-80 mg/day (fast) | Lowest effective dose, alternate-day taper | 2-4 weeks | Hypertension, diabetes, weight gain, osteoporosis, cataracts, glaucoma, neuropsychiatric effects |
| Azathioprine | 50 mg/day | 2.5-3 mg/kg/day | 2-10 months (max benefit up to 24 months) | Bone marrow suppression, hepatotoxicity, GI upset; check TPMT activity before starting |
| Mycophenolate mofetil | 500 mg BID | 1000-1500 mg BID | 3-12 months | GI effects, leukopenia; teratogenic - contraindicated in pregnancy |
| Cyclosporine | 2.5 mg/kg/day | 4-5 mg/kg/day | 3-6 months | Nephrotoxicity, hypertension; monitor levels |
| Tacrolimus | Variable | Variable | 3-6 months | Nephrotoxicity, hypertension, diabetes |
| Rituximab | 375 mg/m² IV weekly x4 or 1000 mg x2 | Variable | Months | Infusion reactions, infections, PML (rare); preferred for MuSK-MG |
| Methotrexate | 7.5 mg/week | Up to 20 mg/week | Months | Hepatotoxicity, pulmonary toxicity, teratogenic |
Note: A 2025 Cochrane systematic review (PMID 40607605) and a 2025 network meta-analysis (PMID 40346603) confirm rituximab's efficacy, particularly for MuSK-MG.
Pillar 3: Short-Term (Rapid-Onset) Immune Therapies
Plasma Exchange (PLEX)
- Reduces circulating antibodies; improvement within days
- Typical course: 5-6 exchanges every other day (2-3 liters per exchange)
- Duration of benefit: typically begins wearing off at 4 weeks, may last up to 3 months
- Indications: myasthenic crisis, pre-thymectomy optimization, to prevent corticosteroid-induced exacerbations
- Side effects: hypocalcemia (citrate), hypotension, arrhythmias, access-related complications
- Effective in up to 95% of patients in myasthenic crisis
Intravenous Immunoglobulin (IVIG)
- Mechanism: modulates immune response (Fc receptor blockade, anti-idiotype antibodies, complement inhibition)
- Dose: 1-2 g/kg over 2-5 days
- Onset: days; duration similar to PLEX
- Side effects: headache, aseptic meningitis, renal failure, thromboembolism, hemolysis
- Mainstay of myasthenic crisis management alongside PLEX
Pillar 4: Thymectomy
- Indicated in all patients with thymoma regardless of disease severity
- Recommended in non-thymomatous generalized MG patients aged 18-50 years with anti-AChR antibodies (MGTX trial showed benefit even in patients not meeting thymectomy criteria previously)
- Role less clear in MuSK-MG, seronegative MG, ocular MG, and patients >50 years
- Effect on MG is delayed: benefit typically seen 6-12 months post-operatively
- Complete stable remission may occur years later
Newer Targeted Therapies
| Drug | Mechanism | Indication |
|---|---|---|
| Eculizumab | Anti-C5 complement inhibitor | Refractory AChR-positive GMG |
| Ravulizumab | Long-acting anti-C5 | Refractory AChR-positive GMG |
| Efgartigimod | FcRn antagonist (reduces IgG levels) | Refractory AChR-positive GMG |
| Rozanolixizumab | Anti-FcRn | Generalized MG |
| Zilucoplan | C5 complement inhibitor (SC) | AChR-positive GMG |
These represent expanding options from better understanding of MG pathophysiology, per a 2024 risk-benefit analysis (PMID 39470879).
Myasthenic Crisis
Definition: Life-threatening exacerbation of MG with respiratory failure requiring mechanical ventilation or delaying extubation.
- Affects approximately 20% of MG patients at some point
- Precipitants: infections (most common), recent surgery, aspiration/dysphagia, interruption of immunosuppressants, many drugs (aminoglycosides, fluoroquinolones, magnesium, beta-blockers, neuromuscular blocking agents, some anesthetics), and stress
Distinguishing myasthenic crisis from cholinergic crisis:
| Feature | Myasthenic Crisis | Cholinergic Crisis |
|---|---|---|
| Cause | Disease exacerbation, insufficient AChEI | Excess AChEI (pyridostigmine overdose) |
| Pupils | Normal/dilated | Miotic (pinpoint) |
| Secretions | Normal | Excessive (SLUDGE) |
| Fasciculations | Absent/mild | Prominent |
| Edrophonium test | Improves weakness | Worsens weakness |
Management of myasthenic crisis:
- Secure the airway - intubate if FVC <15 mL/kg or NIF <-20 cmH2O
- BiPAP may temporize and prevent intubation in select patients
- PLEX or IVIG are the mainstays of therapy
- Hold or reduce pyridostigmine (may increase secretions and worsen respiratory function)
- Treat precipitating cause
- Escalate immunosuppression once stabilized
MG in Special Populations
Pregnancy
- Fertility is unaffected by MG
- Course during pregnancy is unpredictable; ~2/3 of patients report some worsening during pregnancy or puerperium
- Greatest risk: first trimester and puerperium
- Safe drugs: pyridostigmine, prednisone (low dose), PLEX (relatively safe), IVIG
- Avoid: azathioprine, mycophenolate (teratogenic), cyclosporine if possible; rituximab not recommended for non-life-threatening MG in pregnancy
- MG does not affect uterine smooth muscle (labor strength unaffected)
- Regional anesthesia preferred over general for delivery; neuromuscular blocking agents should be avoided
- Neonatal MG: Transient, affecting 10%-20% of neonates born to MG mothers due to transplacental IgG transfer; resolves within weeks
Elderly Patients
- Late-onset MG is now the most common subgroup in Western countries
- Higher risk of thymoma (especially men)
- Drug tolerability is reduced; corticosteroid side effects (osteoporosis, diabetes) are more common
Prognosis
- With modern treatment, most patients achieve minimal manifestation status or pharmacological remission
- Spontaneous remission occurs in ~10%-15% of patients (more common in early disease)
- Thymectomy can eventually lead to complete stable remission in a significant proportion
- Historically, MG had a mortality of ~30%; current mortality is <5% with optimal management
- Myasthenic crisis still carries a mortality of ~5%
Drugs That Worsen MG (to Avoid or Use Cautiously)
- Aminoglycoside antibiotics (gentamicin, tobramycin, neomycin)
- Fluoroquinolones
- Beta-blockers
- Calcium channel blockers (some)
- Magnesium salts
- Neuromuscular blocking agents (both depolarizing and non-depolarizing)
- Chloroquine/hydroxychloroquine
- Penicillamine
- Statins (rarely)
- Checkpoint inhibitors (can unmask or exacerbate MG)
Summary Table: MG at a Glance
| Feature | Detail |
|---|---|
| Type | Autoimmune, acquired |
| Primary target | Nicotinic AChR at NMJ (α1 subunit) |
| Key mechanism | Antibody-mediated destruction of postsynaptic membrane |
| Cardinal sign | Fatigable weakness (worse with activity, better with rest) |
| Most common initial symptom | Ptosis / diplopia (~66%) |
| Best diagnostic test | Anti-AChR antibody + SFEMG |
| Thymus role | Hyperplasia (early-onset), thymoma (10-15%) |
| First-line symptomatic Rx | Pyridostigmine |
| First-line immunotherapy | Prednisone ± azathioprine |
| Rapid treatment | PLEX or IVIG |
| Life-threatening complication | Myasthenic crisis |
| Novel biologics | Eculizumab, efgartigimod, rozanolixizumab |
Sources: Bradley and Daroff's Neurology in Clinical Practice; Goldman Cecil Medicine 26e; Fishman's Pulmonary Diseases; Rosen's Emergency Medicine; Creasy & Resnik's Maternal-Fetal Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.