Blood Vessels and Lymphatics 1. Atherosclerotic Plaque - risk factors, morphology 2. Aneurysm - types, causes, Abdominal Aortic Aneurysm - gross features) 3. Atherosclerosis* - complications; Risk Factors 4. Atherosclerosis of Aorta - pathogenesis, gross, microscopy 1. Atherosclerosis* - pathogenesis, morphology, pathology, complications define all 2mbbs pathology refer harsh mohan cover the points as exam point of view frequently asked add diagrams as well
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
I now have all the content I need. Let me compile the comprehensive exam-focused answer on Atherosclerosis and Aneurysms for 2nd MBBS Pathology.
Blood Vessels and Lymphatics - Atherosclerosis & Aneurysms
2nd MBBS Pathology | Exam-Oriented Notes (Robbins / Harsh Mohan Level)
PART 1: ATHEROSCLEROSIS
Definition
Atherosclerosis is a chronic inflammatory disease of large- and medium-sized arteries characterized by the formation of atheromatous plaques in the intima, consisting of a fibrous cap overlying a soft lipid-rich necrotic core (from Greek: athere = gruel/porridge; sclerosis = hardening).
Risk Factors (TABLE - Frequently Asked in Exams)
| Non-Modifiable (Constitutional) | Modifiable (Acquired) |
|---|---|
| Genetics - Family history; most important independent risk factor | Hyperlipidemia - most important modifiable risk factor |
| Age - Progressive process; clinical manifestations after age 40 in men, later in women | Hypertension - doubles the risk |
| Sex - Males at higher risk; premenopausal women protected by estrogen | Cigarette smoking - most powerful risk factor for MI in young |
| Diabetes mellitus - accelerated atherosclerosis | |
| Obesity / Metabolic syndrome | |
| Inflammation / elevated CRP | |
| Hyperhomocysteinemia | |
| Hypercoagulable states | |
| Sedentary lifestyle / Stress |
Exam Tip: "Increasing age, male sex, family history, hyperlipidemia, hypertension, cigarette smoking, and diabetes mellitus are the major risk factors." Risk factors have greater than additive (multiplicative) effects on each other.
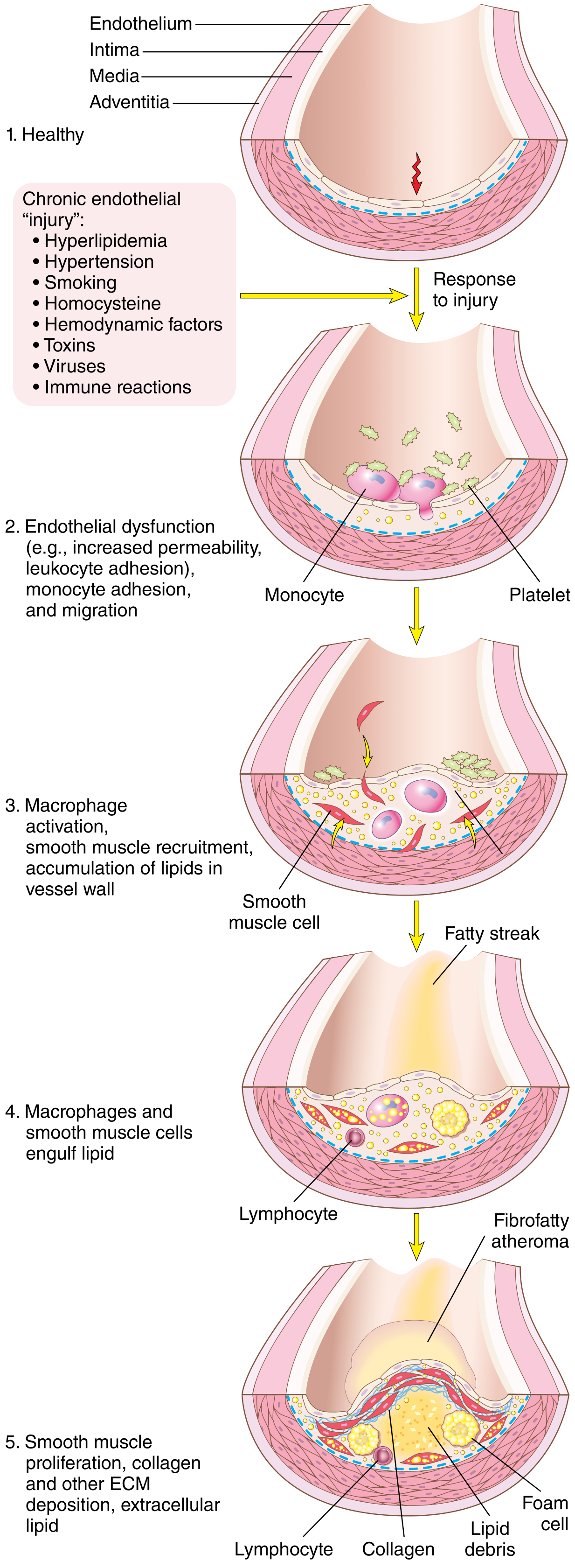
PATHOGENESIS - Response to Injury Hypothesis (Ross, 1993)
The central concept is endothelial injury/dysfunction leading to chronic inflammation in the vessel wall.
Step-by-step sequence:
Step 1 - Endothelial Injury/Dysfunction
- Caused by: hypercholesterolemia, hypertension, cigarette smoke toxins, hemodynamic disturbances (turbulent flow at bifurcations), homocysteine, infections
- Results in: increased permeability, enhanced leukocyte adhesion, altered gene expression
- Laminar (non-turbulent) flow is atheroprotective (upregulates KLF-2 transcription factor)
- Turbulent, non-laminar flow at vessel bifurcations and ostia is atheroprone (explains why plaques form at these sites)
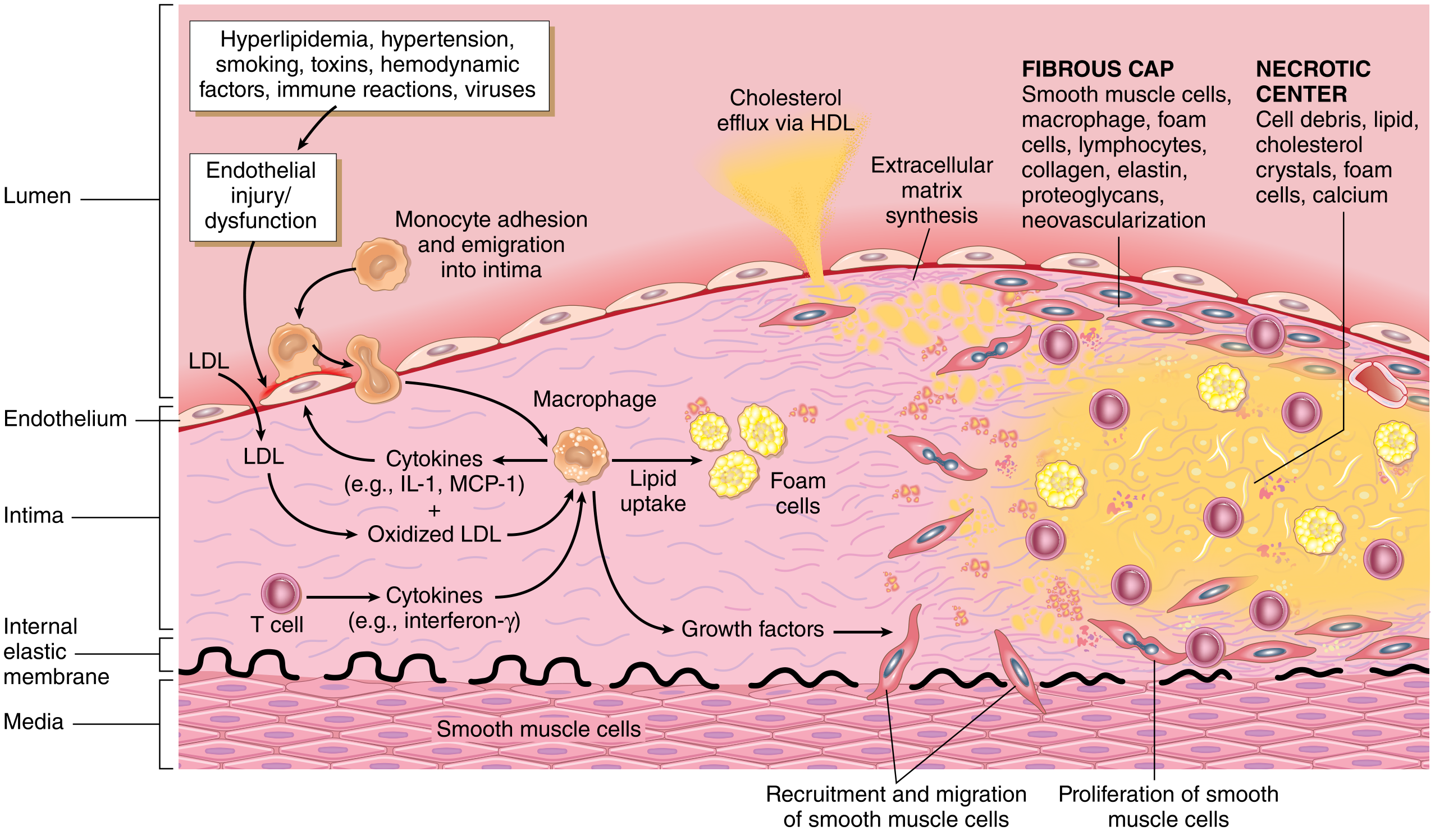
Step 2 - Lipid Accumulation
- LDL enters the vessel wall through dysfunctional endothelium
- LDL is oxidized by reactive oxygen species (ox-LDL)
- Ox-LDL is chemotactic for monocytes and stimulates monocyte adhesion molecules (VCAM-1)
Step 3 - Monocyte Recruitment and Foam Cell Formation
- Monocytes adhere to endothelium (via VCAM-1, ICAM-1) and migrate into intima
- Differentiate into macrophages under influence of M-CSF
- Macrophages phagocytose ox-LDL via scavenger receptors (SR-A, CD36) - NOT the normal LDL receptor
- Lipid-laden macrophages = FOAM CELLS (earliest recognizable lesion = fatty streak)
Step 4 - Inflammation Amplification
- Cholesterol crystals activate NLRP3 inflammasome in macrophages
- Inflammasome cleaves pro-IL-1β → active IL-1 (key proinflammatory cytokine)
- T lymphocytes recruited → produce IFN-γ → further activates macrophages and SMCs
- Macrophages produce reactive oxygen species (enhance LDL oxidation), growth factors, cytokines
Step 5 - Smooth Muscle Cell Proliferation (Key Step)
- Growth factors (PDGF from platelets/macrophages, FGF, TGF-α) recruit SMCs from media into intima
- SMCs proliferate and synthesize collagen, elastin, proteoglycans (ECM)
- SMCs also take up lipid → additional foam cells
- This converts a fatty streak → fibrous/fibrofatty plaque (mature atheroma)
Step 6 - Plaque Maturation
- Continued ECM deposition forms the fibrous cap
- Central necrotic core develops from dead foam cells + extracellular lipid
- Late: calcification occurs
- Neovascularization within the plaque (from adventitia) - a source of intraplaque hemorrhage
MORPHOLOGY (Gross + Microscopy - Very Frequently Asked)
Gross (Macroscopic) Appearances:
1. Fatty Streak (Earliest Lesion)
- Flat, yellow intimal streaks
- Composed of lipid-laden macrophages (foam cells) and SMCs
- Present even in aortas of infants and children
- Not all fatty streaks progress to plaques
2. Fibrofatty (Atheromatous) Plaque (Advanced Lesion)
- Location: Intima of large elastic arteries (aorta, carotid, iliac) and medium muscular arteries (coronary, popliteal)
- Predilection sites: aortic bifurcation, coronary ostia, carotid bifurcation, circle of Willis
- Gross appearance: White-yellow raised lesion, protruding into vessel lumen
- Usually eccentric (involving only part of the vessel circumference)
- On cut section: soft yellow-grey lipid core with overlying white-grey fibrous cap
- Advanced plaques show: calcification (gritty, chalky texture), surface ulceration, superimposed thrombus, intraplaque hemorrhage
Microscopy (Histology):
| Component | Location | Details |
|---|---|---|
| Fibrous cap | Luminal surface | Smooth muscle cells, dense collagen (fibrosis), foam cells, lymphocytes, scattered inflammatory cells |
| Necrotic core | Deep to fibrous cap | Cell debris, extracellular lipid, cholesterol crystals (clefts on H&E - dissolved during processing), foam cells, calcium |
| Shoulders | Periphery of plaque | Most metabolically active area; site of rupture; dense inflammation |
| Neovascularization | Within plaque | Small capillaries growing in from adventitia |
| Media changes | Beneath plaque | Attenuation/thinning of media, loss of SMCs |
Exam Tip (Cholesterol Clefts): On H&E, cholesterol crystals appear as needle-shaped empty clefts (spaces) because the lipid is dissolved during tissue processing.
Stable vs. Vulnerable (Unstable) Plaques
| Feature | Stable Plaque | Vulnerable/Unstable Plaque |
|---|---|---|
| Fibrous cap | Thick, dense | Thin |
| Lipid core | Minimal | Large |
| Inflammation | Little | Dense (especially at shoulders) |
| Calcification | May be heavy | Less |
| Clinical behavior | Chronic stable angina | Acute coronary syndrome (rupture) |
Pathology / Complications of Atherosclerosis (MOST IMPORTANT FOR EXAM)
COMPLICATIONS MNEMONIC: "RACE TO DEAD"
R - Rupture/Ulceration → thrombosis
A - Aneurysm formation
C - Calcification (dystrophic)
E - Embolism (cholesterol/thrombus)
T - Thrombosis (superimposed)
O - Obstruction (luminal stenosis)
D - Dilation (vessel wall weakening)
E - Erosion (endothelial)
A - Acute ischemia (critical stenosis)
D - Downstream ischemia
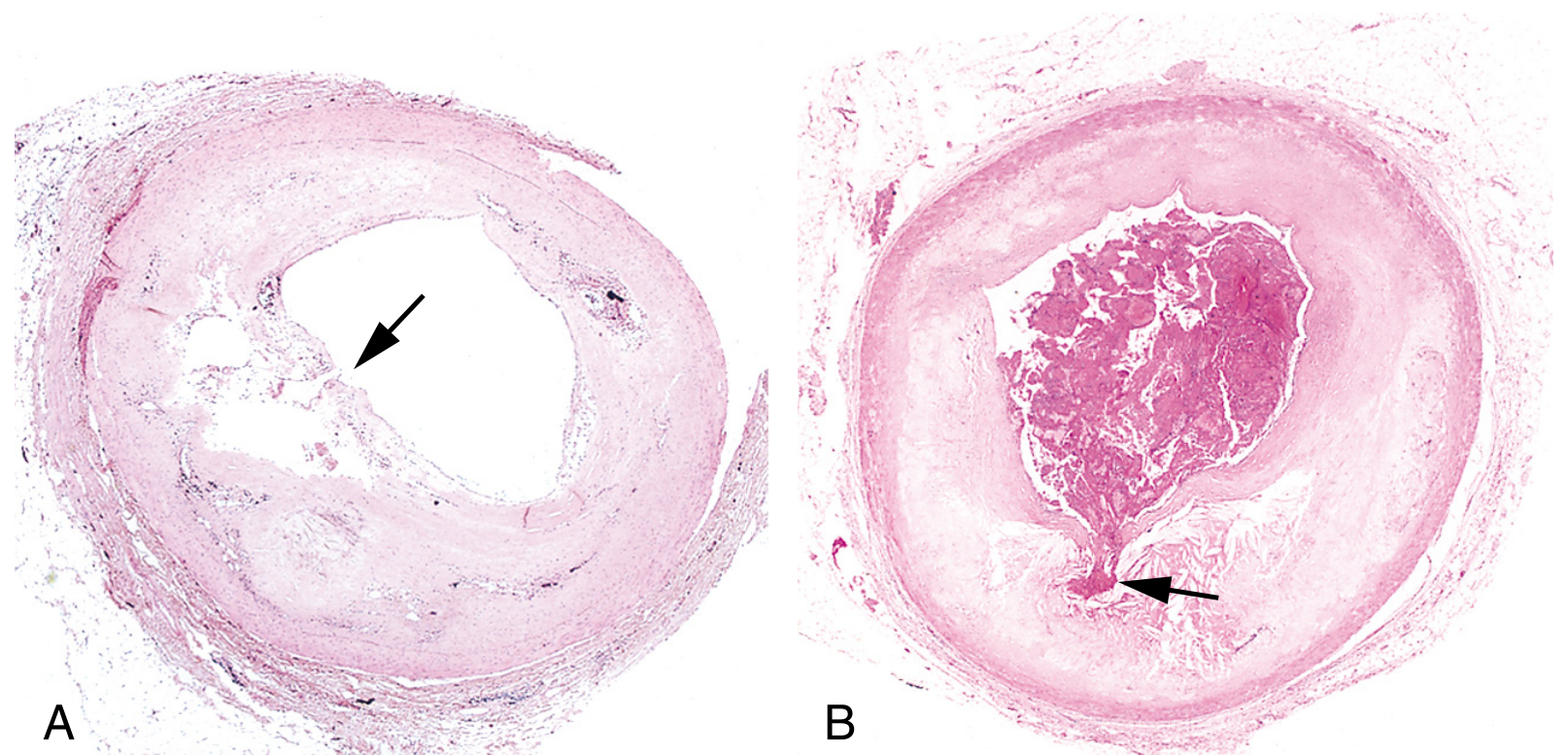
1. Acute Plaque Change (Rupture/Fissuring) - Most Important
- Disruption of fibrous cap → exposes thrombogenic lipid core and subendothelial collagen
- Triggers platelet aggregation + thrombus formation
- Causes: Acute Myocardial Infarction, Unstable Angina, Sudden Cardiac Death
- Vulnerable plaques (thin cap + large lipid core) are paradoxically more dangerous than stable, heavily calcified plaques
2. Chronic Stenosis
- Gradual lumen narrowing → stable chronic ischemia
- Critical stenosis: >70-75% cross-sectional area reduction
- Glagov phenomenon: Outward remodeling compensates early, maintaining lumen size; eventually fails
3. Thrombosis
- Superimposed on ruptured/ulcerated plaque
- Can totally occlude the vessel (MI) or embolize distally
4. Embolism
- Cholesterol crystal emboli from ulcerated plaque
- "Atheroembolism" or "blue toe syndrome"
5. Aneurysm Formation
- Ischemia of medial SMCs (increased diffusion distance from lumen through thickened intima)
- Loss of elastic fibers → wall weakening
- Abdominal aortic aneurysm (AAA) is the classic example
6. Organ Damage
- Coronary arteries → Myocardial infarction, ischemic cardiomyopathy
- Cerebral arteries → Stroke, TIA, vascular dementia
- Renal arteries → Renovascular hypertension, renal failure
- Mesenteric arteries → Mesenteric ischemia
- Peripheral arteries → Intermittent claudication, gangrene
PART 2: ATHEROSCLEROTIC PLAQUE - Risk Factors & Morphology
(Covered in full above; summary for quick revision below)
Risk Factors (Constitutional + Acquired): Genetics, Age, Male sex, Hyperlipidemia, HTN, Smoking, DM, Obesity, Homocysteine, CRP
Morphology - Summary Diagram:
ATHEROMATOUS PLAQUE (Cross-section)
LUMEN
_______________
| FIBROUS CAP | ← SMCs + Collagen + Foam cells + Lymphocytes
|_______________|
| NECROTIC CORE | ← Lipid + Cholesterol clefts + Foam cells + Calcium
| (soft gruel) |
|_______________|
MEDIA ← Thinned, atrophic smooth muscle
PART 3: ANEURYSMS
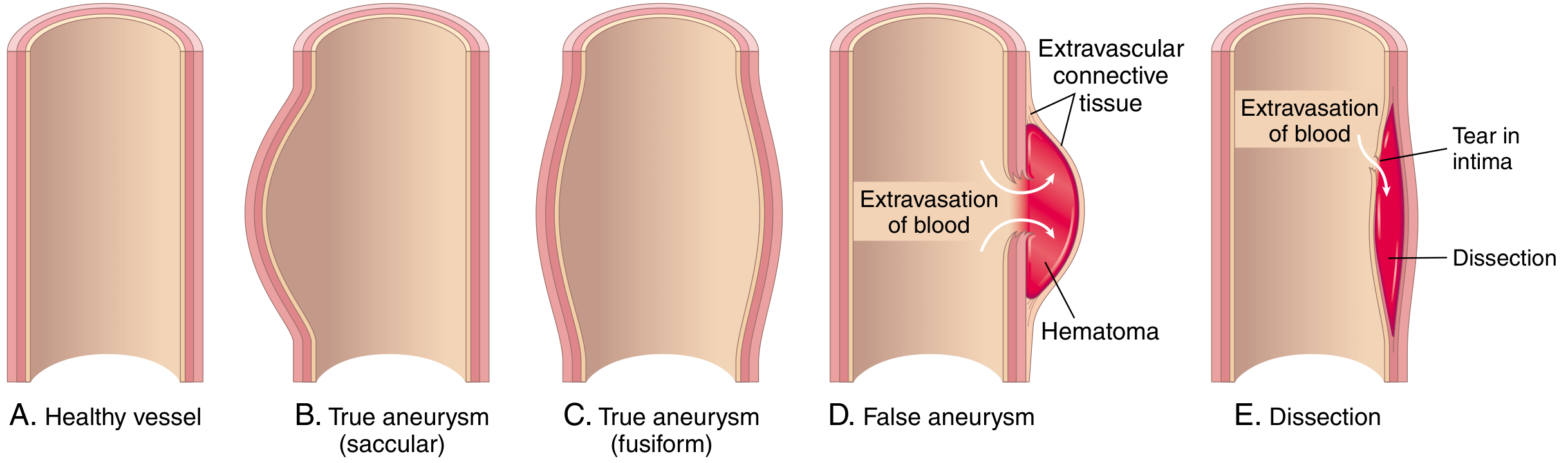
Definition
A localized abnormal dilation of a blood vessel or the heart wall. May be congenital or acquired.
Classification
A. By Wall Structure:
| Type | Description | Examples |
|---|---|---|
| True Aneurysm | All three layers of vessel wall involved (intact but attenuated) | Atherosclerotic aneurysm, Congenital berry aneurysm, Post-MI ventricular aneurysm |
| False Aneurysm (Pseudoaneurysm) | Wall defect → extravascular hematoma communicating with vascular space ("pulsating hematoma") | Post-MI ventricular rupture contained by pericardial adhesion, Vascular graft leak |
| Dissection | Blood enters a defect and tunnels through medial/medial-adventitial planes | Aortic dissection (Type A - ascending; Type B - descending) |
B. By Macroscopic Shape:
| Type | Shape | Features |
|---|---|---|
| Saccular | Spherical outpouching (partial circumference) | 2-20 mm (intracranial); 5-10 cm (aorta) |
| Fusiform | Diffuse, circumferential dilation of long segment | 5-10 cm diameter; can involve entire abdominal aorta |
| Cylindrical | Uniform cylindrical dilation | Less common |
Causes of Aneurysms
| Cause | Mechanism | Type |
|---|---|---|
| Atherosclerosis | Ischemia of media (increased diffusion distance), MMP-mediated ECM destruction | AAA (below renal arteries) |
| Hypertension | Arteriolar disease of vasa vasorum, medial ischemia | Ascending aortic aneurysm |
| Marfan Syndrome | Defective fibrillin → excess TGF-β → ECM destruction | Ascending aorta (type IV Ehlers-Danlos: defective type III collagen) |
| Syphilis (Tertiary) | Obliterative endarteritis of vasa vasorum → medial ischemia | Saccular aortic aneurysm (thoracic) - "tree bark" aortitis |
| Congenital | Berry aneurysm - deficiency of medial muscle | Circle of Willis (subarachnoid hemorrhage) |
| Mycotic (Infective) | Septic embolus → bacterial destruction of wall | Any vessel |
| Trauma | Direct injury | Femoral, popliteal (post-traumatic pseudoaneurysm) |
| Vasculitis | Inflammatory destruction | Polyarteritis nodosa, Takayasu's |
Pathogenesis of Aneurysm Formation:
- Increased MMP (especially from macrophages) degrades elastin and collagen
- Decreased TIMP expression
- Th2 cytokines (IL-4, IL-13) drive elastolytic MMP production in AAA
- Result: loss of elastic fibers → loss of wall recoil → progressive dilation
PART 4: ABDOMINAL AORTIC ANEURYSM (AAA)
Key Facts (High Yield)
- Most common aortic aneurysm
- Atherosclerosis is the major etiologic factor
- Most common in males > 50 years who smoke
- Rarely develops before age 50
- Incidence <5% in males >60 years despite near-universal abdominal aortic atherosclerosis (other factors clearly contribute)
Gross Features (Morphology) - Frequently Asked
- Location: Below the renal arteries (infrarenal aorta) and above the aortic bifurcation - between renal arteries and the bifurcation
- Can extend to involve iliac arteries
- Shape: Saccular or fusiform
- Size: Usually >3 cm; often >5.5 cm (surgical threshold); up to 25 cm in length
- Severe complicated atherosclerosis at the base
- Destruction and thinning of the underlying aortic media
- Contains a laminated mural thrombus (bland, poorly organized) - layered appearance
- Can occlude renal or mesenteric artery ostia by thrombus extension
Three AAA Variants:
- Inflammatory AAA (~5% of cases): Dense perianeurysmal and retroperitoneal fibrosis; sheets of lymphocytes and plasma cells; may be related to IgG4-related disease
- Mycotic (Infective) AAA: Infected from bacteremia/adjacent sepsis
- Aortoiliac Occlusive Disease (Leriche Syndrome): Atherosclerotic occlusion at aortic bifurcation; triad of claudication + impotence + absent femoral pulses
Complications of AAA:
- Rupture - most feared complication; retroperitoneal hemorrhage, can be fatal
- Risk of rupture ↑ sharply when diameter >5.5 cm
- Obstruction of branch vessels (renal, mesenteric, vertebral arteries)
- Embolism from mural thrombus → lower limb ischemia
- Impingement on adjacent structures (vertebrae - erosion, duodenum, ureters)
- Aorto-duodenal/aorto-venous fistula
PART 5: ATHEROSCLEROSIS OF AORTA - Gross, Microscopy, Pathogenesis
Sites of Predilection in Aorta:
- Posterior abdominal aorta (most severely affected) - due to non-laminar flow
- Abdominal aorta > thoracic aorta (in severity)
- Ostia of exiting branch vessels
- Aortic bifurcation
Gross Appearance (Sequence of Lesions):
- Fatty streaks - flat, yellow, lipid streaks in intima (aorta most common site in young)
- Fibrous plaques - raised, pearly white/grey nodular lesions protruding into lumen; firm consistency
- Complicated plaques:
- Surface ulceration (crater-like defects)
- Calcification (dystrophic, "eggshell" or "pipestem" appearance)
- Superimposed thrombus (grey-red, layered)
- Intraplaque hemorrhage (dark red areas within plaque from rupture of neovessels)
- Atheroembolism (yellow cholesterol crystals/fragments in downstream vessels)
Microscopy:
- Intima: Foam cells, cholesterol clefts (empty needle-shaped spaces), fibrosis, calcification, necrotic debris, inflammatory infiltrate (lymphocytes, macrophages)
- Fibrous cap: Dense collagen (stains blue on Masson trichrome), SMCs, scattered foam cells
- Media: Thinned, attenuated; SMC loss; elastic fibers disrupted (Weigert elastic stain shows fragmentation)
- Adventitia: Thickened, may show lymphoplasmacytic infiltrate, thickened vasa vasorum
QUICK REVISION SUMMARY TABLE
| Topic | Key Points |
|---|---|
| Definition of atherosclerosis | Chronic inflammatory intimal disease; atheromatous plaques |
| Most important modifiable RF | Hyperlipidemia (LDL cholesterol) |
| Most important non-modifiable RF | Genetics/family history |
| Earliest lesion | Fatty streak (foam cells only) |
| Key cell in pathogenesis | Macrophage (foam cell) |
| Fibrous cap composition | SMC + Collagen + Foam cells |
| Necrotic core content | Lipid + Cholesterol clefts + Foam cells + Calcium |
| Most dangerous plaque type | Vulnerable plaque (thin cap, large core) |
| Mechanism of plaque rupture | Thin fibrous cap + large lipid core + dense shouldering inflammation |
| Critical stenosis threshold | >70-75% cross-sectional area |
| Most common complication | Ischemic heart disease (MI) |
| Aneurysm mechanism | MMP-mediated ECM degradation → loss of elastic fibers |
| AAA location | Infrarenal aorta (between renal arteries and bifurcation) |
| AAA mural content | Laminated mural thrombus |
| AAA surgical threshold | >5.5 cm diameter |
| Syphilitic aneurysm | Thoracic aorta (saccular); "tree bark" texture |
| Berry aneurysm site | Circle of Willis; rupture → SAH |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease (10th ed.), Chapter 11 - Blood Vessels; Robbins & Kumar Basic Pathology (11th ed.) - aligned with Harsh Mohan Textbook of Pathology exam content for 2nd MBBS.
This is a shared conversation. Sign in to Orris to start your own chat.