What-- How do you regulate a BP? If this according is asked. In my physiology exam, what would I write? What is the regulation of BP?
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Finding Sources
I now have all the content I need. Let me compile a comprehensive, well-structured physiology exam answer on BP regulation.
Regulation of Blood Pressure - Complete Physiology Exam Answer
The core formula you must state first:
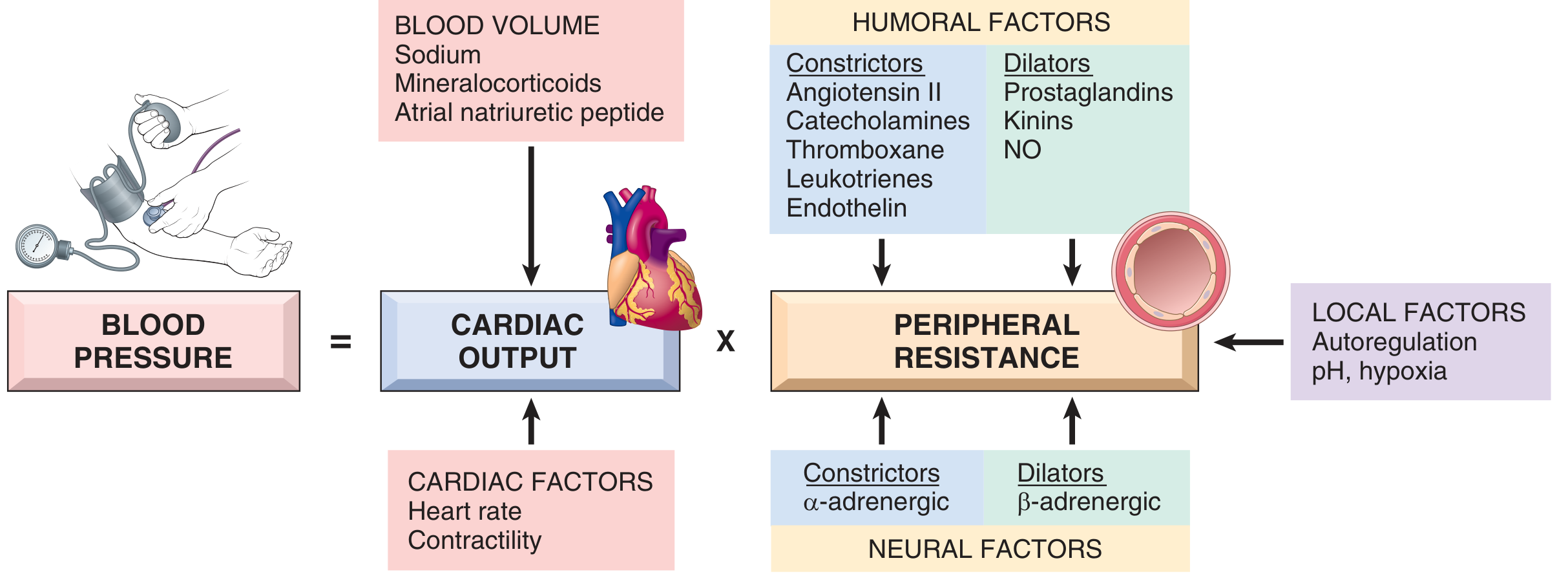
Blood Pressure (BP) = Cardiac Output (CO) × Peripheral Vascular Resistance (PVR)
Anything that regulates BP does so by altering one or both of these variables. CO is itself determined by heart rate × stroke volume; PVR is determined primarily at the arteriole level.
I. BASIC DETERMINANTS OF BLOOD PRESSURE
BP = CO × PVR
| Factor | Determinants |
|---|---|
| Cardiac Output | Heart rate + Stroke volume (preload/contractility/afterload) |
| Peripheral Resistance | Arteriolar tone (neural + humoral + local factors) |
Blood volume is the key upstream regulator - it determines venous return, which determines stroke volume (Frank-Starling law), which determines CO.
(Robbins & Kumar Basic Pathology)
II. NEURAL REGULATION (Short-Term / Fast - seconds to minutes)
Neural regulation is rapid and acts primarily through the autonomic nervous system via the vasomotor center in the medulla oblongata.
1. Baroreceptor Reflex (Most Important)
This is the primary, moment-to-moment pressure regulator.
Receptors: "Spray-type" stretch receptors (mechanoreceptors) located in:
- Carotid sinus - at the bifurcation of the common carotid artery (wall of internal carotid). Most sensitive.
- Aortic arch - in the aortic wall. Responds mainly to increases in pressure; operates ~30 mmHg higher than carotid receptors.
Afferent pathway:
- Carotid sinus → Hering's nerve → Glossopharyngeal nerve (CN IX) → Nucleus Tractus Solitarius (NTS) in medulla
- Aortic arch → Vagus nerve (CN X) → NTS in medulla
Normal operating range: Carotid baroreceptors begin firing at ~60 mmHg; maximum firing at ~180 mmHg. They are most sensitive around the normal mean arterial pressure of ~100 mmHg.
When BP rises:
- Baroreceptors stretch → firing rate increases
- NTS activated → stimulates cardioinhibitory center (dorsal motor nucleus of vagus) + inhibits vasomotor center
- Result: ↑ parasympathetic tone (↓ HR) + ↓ sympathetic tone (↓ contractility, vasodilation)
- BP falls back toward normal
When BP falls:
- Reduced baroreceptor firing
- Vasomotor center activated + cardioinhibitory center inhibited
- ↑ sympathetic outflow → vasoconstriction + ↑ HR + ↑ contractility
- BP rises back toward normal
Limitation: Baroreceptors adapt (reset) over 1-3 days in sustained hypertension - they lose effectiveness for long-term control. They are best suited for minute-to-minute adjustments.
(Guyton and Hall Textbook of Medical Physiology; Costanzo Physiology 7th Edition)
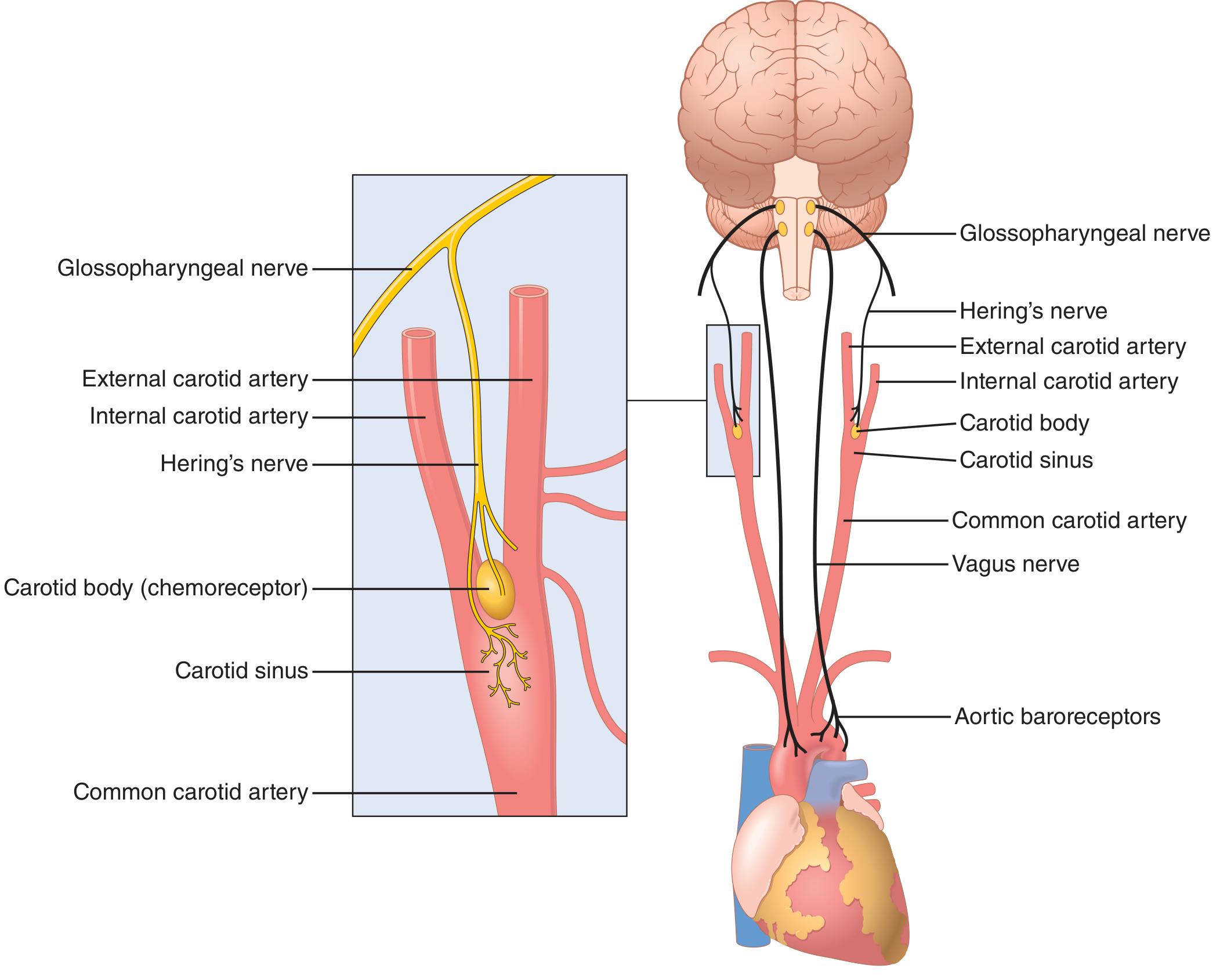
2. Chemoreceptor Reflex (Secondary Neural)
Peripheral chemoreceptors (carotid bodies, aortic bodies) detect ↓PO₂, ↑PCO₂, or ↓pH.
- They exert a positive drive on the vasomotor center → vasoconstriction
- They exert a positive drive on the cardioinhibitory center → bradycardia (when ventilation is fixed)
- In intact breathing: the ventilatory response overrides and produces tachycardia
Central chemoreceptors in the medulla respond to ↑CO₂/↓pH locally.
3. CNS Ischemic Response (Emergency Regulator)
When BP falls below ~60 mmHg, blood flow to the vasomotor center itself is reduced. CO₂ accumulates in the brainstem → intensely stimulates sympathetic vasoconstrictor neurons → BP may shoot up to 250 mmHg. This is a last-ditch "emergency" response.
4. Other Neural Reflexes
- Bainbridge reflex: Atrial stretch receptors (low-pressure receptors) detect increased venous return → reflex tachycardia via vagus → increases CO → prevents venous pooling
- Cushing reflex: Raised intracranial pressure compresses brain vessels → CNS ischemia → massive sympathetic discharge → hypertension + bradycardia (Cushing's triad)
III. HUMORAL REGULATION (Short-to-Intermediate Term - minutes to hours)
These are circulating substances that act on blood vessels and the heart.
Vasoconstrictors (↑ BP):
| Substance | Source | Mechanism |
|---|---|---|
| Angiotensin II | RAAS (kidney/liver/lung) | Direct arteriolar constriction; stimulates aldosterone release |
| Catecholamines (noradrenaline/adrenaline) | Adrenal medulla, sympathetic nerves | α₁ receptors → vasoconstriction; β₁ → ↑ HR, ↑ contractility |
| Endothelin-1 | Vascular endothelium | Extremely potent vasoconstrictor |
| Vasopressin (ADH) | Posterior pituitary | Vasoconstriction + water reabsorption → ↑ blood volume |
| Thromboxane A₂ | Platelets | Vasoconstriction |
Vasodilators (↓ BP):
| Substance | Source | Mechanism |
|---|---|---|
| Nitric Oxide (NO) | Vascular endothelium | ↑ cGMP → smooth muscle relaxation → vasodilation |
| Prostacyclin (PGI₂) | Endothelium | Vasodilation |
| Bradykinin (Kinins) | Plasma; stimulates NO/PGI₂ release | Vasodilation |
| Atrial Natriuretic Peptide (ANP) | Cardiac atria (released by stretch) | Vasodilation + promotes sodium/water excretion |
| Adrenomedullin | Adrenal medulla | Vasodilation |
IV. RENAL REGULATION - LONG-TERM (hours to days)
The kidney is the only organ capable of long-term BP regulation. It does this via the pressure-natriuresis mechanism - when BP rises, the kidney excretes more sodium and water, reducing blood volume, which reduces CO, which lowers BP back to normal.
Renin-Angiotensin-Aldosterone System (RAAS)
This is the most important hormonal system for long-term BP regulation.
Trigger for renin release (from juxtaglomerular cells of afferent arteriole):
- ↓ renal perfusion pressure (detected directly by JG cells)
- ↓ NaCl delivery to macula densa (via tubuloglomerular feedback)
- ↑ sympathetic nerve activity (β₁ receptors on JG cells)
Cascade:
Renin (JG cells)
↓
Angiotensinogen (liver) → Angiotensin I
↓ (ACE in lung)
Angiotensin II
↙ ↘
Vasoconstriction Aldosterone release (adrenal cortex)
(↑ PVR) ↓
Na⁺/H₂O reabsorption (collecting duct)
→ ↑ Blood volume → ↑ CO → ↑ BP
Angiotensin II also:
- Stimulates ADH release from posterior pituitary
- Stimulates thirst (drinking behavior)
- Directly stimulates renal tubular Na⁺ reabsorption
Sodium Homeostasis (Key Concept for Exams)
The kidneys filter ~170 L/day of plasma. ~98% of Na⁺ is reabsorbed by constitutive transporters. The final 2% - controlled by aldosterone via ENaC (epithelial sodium channel) - determines net sodium balance and therefore blood volume and long-term BP.
(Robbins & Kumar Basic Pathology; Guyton and Hall)
V. LOCAL / AUTOREGULATORY MECHANISMS
At the tissue level, blood vessels auto-regulate to maintain constant flow despite changes in perfusion pressure.
- Myogenic response: Increased intravascular pressure → vascular smooth muscle stretches → reflex vasoconstriction (Bayliss effect)
- Metabolic autoregulation: Tissue hypoxia, ↑CO₂, ↑H⁺, ↑K⁺, adenosine → local vasodilation to match blood flow to metabolic demand
- Endothelial-derived factors: NO (dilator), endothelin (constrictor) balance vascular tone continuously
VI. SUMMARY TABLE - FOR EXAM QUICK RECALL
| Mechanism | Onset | Duration | Primary Action |
|---|---|---|---|
| Baroreceptor reflex | Seconds | Minutes | ↑/↓ HR + vasomotor tone |
| Chemoreceptor reflex | Seconds | Minutes | Vasoconstriction + ↓ HR |
| CNS ischemic response | Seconds | Emergency only | Massive vasoconstriction |
| Catecholamines (circulating) | Minutes | Hours | ↑ HR, ↑ contractility, vasoconstriction |
| RAAS (Angiotensin II) | Minutes-hours | Hours | Vasoconstriction + aldosterone → Na⁺ retention |
| Aldosterone (Na⁺ retention) | Hours | Days | ↑ Blood volume → ↑ CO |
| Renal pressure-natriuresis | Hours-days | Permanent | Controls set point of BP |
| ADH (vasopressin) | Minutes | Hours | Water retention + vasoconstriction |
| ANP | Minutes | Hours | Natriuresis + vasodilation |
How to Structure Your Exam Answer
- Start with the formula: BP = CO × PVR
- Divide into 3 categories: Neural (short-term), Humoral (intermediate), Renal (long-term)
- Lead with baroreceptor reflex - give anatomy, arc, and response to both rise and fall in BP
- Then RAAS - draw the cascade with renin → Ang I → Ang II → aldosterone
- Mention local autoregulation briefly
- End with the key concept: Only the kidneys provide infinite-gain, long-term control
Sources:
- Guyton and Hall Textbook of Medical Physiology (Baroreceptor Arterial Pressure Control, pp. 227-231)
- Costanzo Physiology, 7th Edition (Baroreceptor Reflex, p. 169-170)
- Robbins & Kumar Basic Pathology (Blood Pressure Regulation, p. 309)
- Katzung's Basic and Clinical Pharmacology, 16th Edition (Normal Regulation of Blood Pressure, p. 268)
- Medical Physiology (Boron & Boulpaep) (Chemoreceptor control of cardiovascular system)
This is a shared conversation. Sign in to Orris to start your own chat.