Hypothyroidism
hypothyroidism management treatment
Hypothyroidism
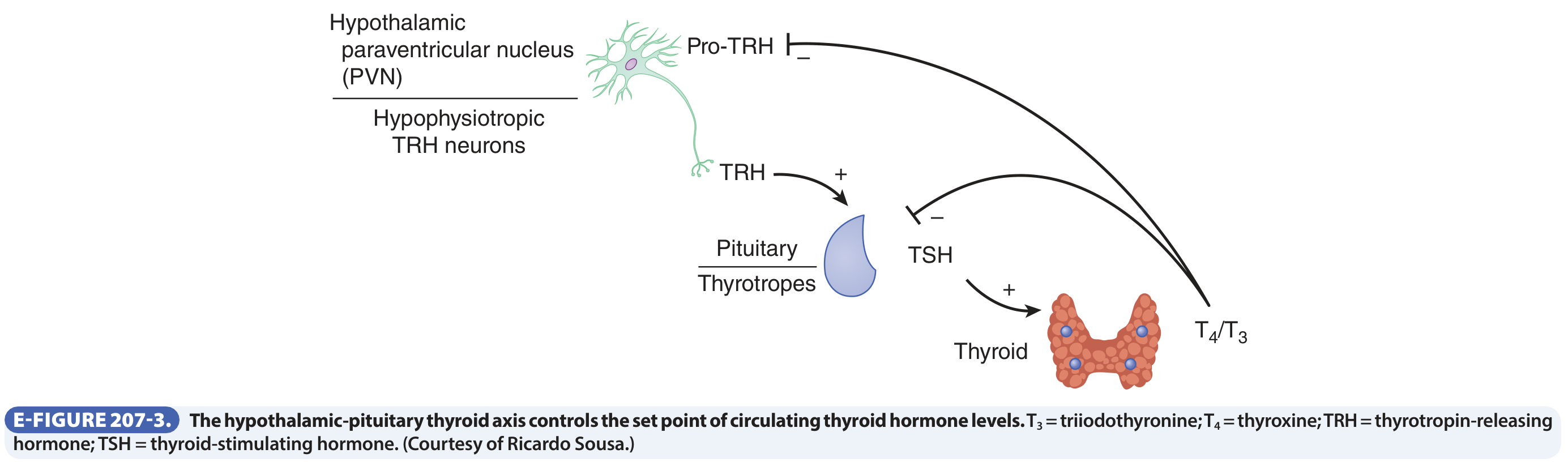
The Hypothalamic-Pituitary-Thyroid (HPT) Axis
Classification
| Type | TSH | Free T4 | Notes |
|---|---|---|---|
| Overt Primary | >20 mIU/L (often much higher) | Low | Symptomatic; most common type |
| Subclinical Primary | 4.5-20 mIU/L | Normal | Often found incidentally |
| Secondary (Central) | Low or inappropriately normal | Low | Pituitary or hypothalamic failure |
- Goldman-Cecil Medicine, p. 2433
Causes
Primary Hypothyroidism
| Cause | Mechanism |
|---|---|
| Hashimoto thyroiditis | Autoimmune lymphocytic destruction; most common cause in iodine-sufficient regions |
| Iodine deficiency | Decreased hormone synthesis; most common cause worldwide (~2 billion affected) |
| Post-surgical/post-radiation | Loss of thyroid tissue |
| Thyroiditis (subacute, postpartum) | Inflammatory destruction - often transient |
| Drugs | Lithium, amiodarone, interferon-α, tyrosine kinase inhibitors, immune checkpoint inhibitors |
| Dyshormonogenetic goiter | Congenital defect in hormone synthesis (rare) |
| Thyroid hormone resistance | Mutation in TR receptor (rare) |
| Congenital (1 in 3500 births) | Transcription factor defects causing thyroid dysgenesis |
Secondary (Central) Hypothyroidism
Hashimoto Thyroiditis (Chronic Lymphocytic Thyroiditis)
- CD8+ cytotoxic T cells kill thyroid epithelial cells directly
- Cytokines (IFN-γ, TNF) from activated T cells induce apoptosis via Fas-FasL pathway
- Anti-TPO (thyroid peroxidase) and anti-thyroglobulin antibodies are present in nearly all patients - TPO-Ab titers predict progression to overt hypothyroidism
- Autoimmune risk is highly heritable (variants in immunomodulatory genes)
Clinical Features of Hypothyroidism
| System | Manifestations |
|---|---|
| General | Fatigue, weight gain, cold intolerance, lethargy |
| Skin | Dry, coarse, cool skin; coarse brittle hair; loss of lateral eyebrow (Queen Anne's sign); non-pitting edema (myxedema) - due to accumulation of glycosaminoglycans |
| Face | Periorbital puffiness, broadening/coarsening of features, macroglossia, deepening voice |
| Cardiovascular | Bradycardia, reduced cardiac output, diastolic hypertension, pericardial effusion |
| Neuromuscular | Slow reflexes (prolonged relaxation phase), myalgia, carpal tunnel syndrome, cerebellar ataxia, cognitive slowing |
| Psychiatric | Depression, memory impairment ("myxedema madness" in severe cases) |
| GI | Constipation, ileus (severe) |
| Reproductive | Menorrhagia, anovulation, infertility; in men - decreased libido, erectile dysfunction |
| Labs | Elevated LDL cholesterol, elevated CK (from muscle involvement), hyponatremia, normocytic or macrocytic anemia |
Diagnosis
- In primary hypothyroidism: TSH is elevated because loss of T4/T3 removes negative feedback on TRH and TSH
- In central hypothyroidism: TSH is low or inappropriately normal despite low T4
- Serum T4 (free T4): decreased in overt hypothyroidism of any cause
- TPO-Ab: confirms autoimmune etiology; elevated in >95% of Hashimoto thyroiditis
- Pitfalls to be aware of (Goldman-Cecil Table 207-1):
- Biotin supplementation (>100 mg/day): artificially lowers TSH, elevates T4/T3 - resolves after stopping biotin 2-3 days
- Heterophile antibodies: artificially raise TSH
- Macro-TSH: elevated TSH but bioinactive - use polyethylene glycol precipitation to detect
Treatment
Overt Hypothyroidism
- Average replacement dose: 1.6 µg/kg/day orally
- Start lower (25-50 µg/day) in elderly patients and those with cardiac disease; titrate upward every 4-6 weeks
- Goal: TSH in the normal reference range (0.5-2.5 mIU/L for most patients)
- Monitor TSH annually once stable
- Take on empty stomach; separate from calcium, iron, cholestyramine (absorption interference)
Combination T4/T3 Therapy
Subclinical Hypothyroidism
- TSH >10 mIU/L: L-T4 treatment reasonable - may reduce LDL cholesterol; no symptom benefit in elderly (>65 years)
- TSH 5-10 mIU/L: Consider treating if symptoms are present OR elevated TPO-Ab titers
- Otherwise: recheck TSH and free T4 annually
Hypothyroidism in Pregnancy
- L-T4 dose requirement increases by 25-50% during pregnancy (increased TBG, fetal demand, placental metabolism)
- A practical approach: increase from 7 tablets/week to 9 tablets/week as soon as pregnancy is confirmed
- Target TSH: <2.5 mIU/L throughout gestation
- Check TSH every 4 weeks until mid-gestation
- Untreated hypothyroidism in early pregnancy is linked to impaired fetal neurological development
Myxedema Coma
- IV L-T4: loading dose 200-300 µg IV, then 1.6 µg/kg IV every 24 hours
- IV T3: 5-10 µg every 8-12 hours (added because T4→T3 conversion is impaired)
- IV hydrocortisone: 100 mg every 6 hours until adrenal insufficiency excluded (concurrent adrenal insufficiency is common)
- Passive rewarming only - active rewarming worsens hypotension
Special Populations and Considerations
Congenital Hypothyroidism
- Incidence: 1 in 3,500 births
- Causes: thyroid dysgenesis, dyshormonogenesis, or severe iodine deficiency
- Consequences: devastating irreversible neurological damage ("cretinism") if untreated
- Neonatal TSH screening programs have dramatically reduced impact
Drug-Induced Hypothyroidism
Thyroiditis Summary Table
| Hashimoto | Subacute (de Quervain) | Painless | Riedel | |
|---|---|---|---|---|
| Pathogenesis | Autoimmune (CD8 T cells) | Presumed viral | Presumed autoimmune | IgG4-related disease |
| Pain | None | Painful neck, fever | None | Hard fixed mass |
| Thyroid function | Progressive hypothyroidism | Transient hyper → hypothyroid | Transient hyperthyroid | Usually euthyroid |
| Histology | Lymphocytic infiltrate, germinal centers, fibrosis | Disrupted follicles, granulomas | Lymphocytic inflammation | Extensive fibrosis, IgG4+ plasma cells |
Recent Evidence (2024-2026)
- A 2025 systematic review (PMID 40446861) in Complementary Therapies in Medicine found long-term exercise-based interventions may modestly improve thyroid function in hypothyroid patients, though evidence remains limited.
- A 2026 meta-analysis (PMID 42095176) identified predictors of permanent hypothyroidism after subacute thyroiditis.
- A 2025 meta-analysis (PMID 40609565) in Lancet Diabetes & Endocrinology examined links between gestational thyroid function/autoimmunity and gestational diabetes.
- Goldman-Cecil Medicine International Edition, pp. 2431-2436
- Robbins & Kumar Basic Pathology, pp. 729-731
- Textbook of Family Medicine 9e, pp. 1021-1022
Patient with hashimotos need life long levothyroxine
Hashimoto thyroiditis levothyroxine discontinuation remission
Hashimoto thyroiditis levothyroxine withdrawal spontaneous remission
hypothyroidism levothyroxine discontinuation euthyroid
PMID: 41482002
Is Levothyroxine Lifelong in Hashimoto's? - Not Always
The Key Distinction: What Are You Treating?
| Scenario | Lifelong L-T4? |
|---|---|
| Overt hypothyroidism (low FT4, TSH >20) with progressive gland destruction | Yes - almost certainly lifelong |
| Subclinical hypothyroidism (TSH mildly elevated, normal FT4) | Not necessarily - reassess |
| Hashimoto's with normal TSH and FT4 (euthyroid) | No treatment needed at all |
| Transient hypothyroidism during a flare | May resolve spontaneously |
Spontaneous Remission is Real (in ~10% of Cases)
"Hypothyroidism resulting from Hashimoto thyroiditis is transient in approximately 10% of cases. Spontaneous remission is associated with the presence of a larger goiter, a high initial TSH level, and a family history of thyroid disease."
The Problem of Overuse and Deprescribing
- Levothyroxine is one of the most overprescribed medications in the US
- Many patients are started on it for mild subclinical hypothyroidism or non-evidence-based indications (e.g., weight gain, depression in euthyroid individuals)
- High-certainty evidence does NOT show benefit of levothyroxine in subclinical hypothyroidism for quality of life or symptom outcomes
- Once started, it is continued lifelong for most patients - even when not warranted
- The paper argues for "deprescribing" - a structured, supervised withdrawal of levothyroxine in selected patients where it is no longer necessary or never was
When Levothyroxine IS Lifelong
- Overt hypothyroidism (low FT4, markedly elevated TSH) - especially with symptoms
- Advanced gland destruction - ultrasound showing severe fibrosis/atrophy with negligible residual tissue
- Post-thyroidectomy or post-radioiodine (not Hashimoto per se, but often co-exists)
- Pregnancy history of dose requirements confirms significant gland failure
- Persistently positive TPO-Ab with progressive TSH rise over serial testing - predicts irreversible failure
"As [Hashimoto's] progresses, more functioning thyroid gland becomes fibrotic, and less indigenous T4 is produced. After diagnosis, replacement doses of T4 should be used... Serum TSH is followed annually to ensure adequate control."
Practical Clinical Approach
- Periodic reassessment is mandatory - TSH annually even in stable patients
- If TSH normalizes on a low L-T4 dose, consider a supervised trial of dose reduction or discontinuation with close TSH monitoring (every 6-8 weeks initially)
- Do not assume lifelong need simply because Hashimoto's is the diagnosis - titrate to the thyroid function, not the antibody status
- Antibody titers alone (TPO-Ab, TgAb) are not an indication for treatment in a euthyroid patient
- For subclinical hypothyroidism (TSH 5-10 mIU/L), guidelines suggest treatment only if TSH >10, or if symptomatic, or if pregnant - not reflexively lifelong in all cases
Bottom Line
- Cummings Otolaryngology Head and Neck Surgery, p. 2717
- Textbook of Family Medicine 9e, p. 1022
- Maraka S & Papaleontiou M. "Approach to the Patient Considering Thyroid Hormone Deprescribing." J Clin Endocrinol Metab, 2026 (PMID: 41482002)


In this patient tsh is nearly 11 and t4 is normal and the anti tpo is elevated it ite clearly autoimmune right?
- TSH: 11.7 µIU/mL (ref: 0.38-5.33) - elevated
- fT4: 0.7 ng/dL (ref: 0.58-1.64) - low-normal (within range but toward the lower end)
- Anti-TPO: 116.99 IU/mL (ref: <5.61) - markedly elevated (~20x upper limit)
- Anti-Tg: 4.08 IU/mL (ref: <4.11) - borderline normal
- Patient: Thanusree, 20-year-old female, Government Stanley Medical College / Dr. Stanley Hospital, Chennai
Interpretation
| Finding | Value | Significance |
|---|---|---|
| TSH elevated | 11.7 (ref <5.33) | Subclinical-to-borderline overt hypothyroidism |
| fT4 low-normal | 0.7 (ref 0.58-1.64) | At the lower quarter of the reference range - the pituitary is working hard to keep T4 "within range" |
| Anti-TPO markedly elevated | 116.99 (ref <5.61) | ~20x upper limit - strongly autoimmune |
| Anti-Tg borderline | 4.08 (ref <4.11) | Near the cutoff - not independently significant here |
Important Nuances for This Specific Patient
1. This is Subclinical Hypothyroidism (borderline overt)
- TSH at 11.7 is above the "subclinical" threshold of 10 mIU/L - this is the zone where treatment benefit becomes clearer
- fT4 is still technically within range, but sitting low-normal - the pituitary compensation is working but barely
2. Age and sex matter
- 20-year-old female: high prior probability of autoimmune thyroid disease (female:male = 10:1 to 20:1)
- At this age with active autoimmune destruction and TSH >10, treatment with levothyroxine is recommended - this is not the elderly patient where benefit is uncertain
3. Anti-Tg adds little here
- Anti-Tg (4.08 vs ref <4.11) is essentially normal
- Anti-TPO alone is sufficient to diagnose Hashimoto's - and it is very clearly positive here
4. What "autoimmune" does NOT automatically mean
- It does not tell you the degree of gland destruction yet - a thyroid ultrasound would help (heterogeneous echotexture, hypoechogenicity, increased vascularity are typical in Hashimoto's)
- Anti-TPO positivity alone in a euthyroid individual does not require treatment - but this patient is not euthyroid (TSH 11.7)
Bottom Line for Thanusree
| Question | Answer |
|---|---|
| Is it autoimmune? | Yes - Hashimoto thyroiditis |
| Is it overt or subclinical? | Borderline - TSH 11.7 with low-normal fT4 |
| Does she need levothyroxine? | Yes - TSH >10 + young symptomatic age + positive TPO-Ab = treat |
| Is it lifelong? | Likely yes - but recheck TSH every 6-12 months; at 20, her gland has years of progressive destruction ahead |
| Any other workup? | Thyroid ultrasound to assess gland morphology; check for other autoimmune diseases (she is young) |
After few years is there any chance to stop levothyroxine and live a life without tablet
Hashimoto thyroiditis levothyroxine discontinuation remission euthyroid
hypothyroidism levothyroxine deprescribing withdrawal remission
Hashimoto thyroiditis spontaneous remission young adults
hypothyroidism levothyroxine deprescribing thyroid hormone overuse
selenium Hashimoto thyroiditis TPO antibody reduction
Honest Answer: Stopping Levothyroxine in Hashimoto's
The Short Answer
Why Stopping is Unlikely in Most Hashimoto's Patients
- Destroyed thyroid tissue does not regenerate. Once follicles are replaced by fibrosis, that functional mass is gone permanently.
- The disease generally progresses over decades - meaning the thyroid makes less and less hormone over time, not more.
- A young patient (20 years old) with already-elevated TSH and high Anti-TPO is at an early-to-mid stage of this process. Without treatment, it will worsen, not reverse.
- Annual TSH monitoring in Hashimoto's patients shows a 4-5% per year progression rate from subclinical to overt hypothyroidism.
The ~10% Who Can Stop
"Hypothyroidism resulting from Hashimoto thyroiditis is transient in approximately 10% of cases. Spontaneous remission is associated with: a larger goiter, a high initial TSH level, and a family history of thyroid disease."
What "Deprescribing" Research Says (2026)
- Levothyroxine is one of the most overprescribed drugs in the world
- Many patients are started unnecessarily and stay on it lifelong without re-evaluation
- Structured, supervised withdrawal IS feasible and safe in selected patients
- The key selected patients are those with: mild subclinical hypothyroidism at initiation, or who were started for non-evidence-based reasons
What Actually Helps Reduce the Autoimmune Burden
| Intervention | Evidence | What it Does |
|---|---|---|
| Selenium 200 µg/day | Moderate (multiple RCTs) | Reduces Anti-TPO titers; modest anti-inflammatory effect on thyroid; may slow progression |
| Adequate iodine (not excess) | Good | Excess iodine worsens Hashimoto's - avoid high-iodine supplements |
| Vitamin D sufficiency | Emerging | Low Vit D is associated with higher TPO-Ab; correction may help |
| Gluten-free diet | Weak/controversial | Some benefit in Hashimoto's with co-existing celiac (screen for it); no clear benefit in non-celiac patients |
| Stress reduction, sleep | Indirect | Autoimmune activity is worsened by chronic stress/sleep deprivation |
The Most Realistic Path Forward for Thanusree
| Timeframe | What to do | What to watch for |
|---|---|---|
| Now - 6 months | Start levothyroxine, recheck TSH in 6-8 weeks, titrate to TSH 1-2 mIU/L | Symptom improvement |
| Every 6-12 months | Check TSH, fT4, and periodically Anti-TPO | Is TSH stable or rising? Is gland failing further? |
| After 1-2 years of stable TSH | If dose requirement is very low (e.g., 25-50 µg/day), discuss a supervised trial of dose reduction with her endocrinologist | TSH should be rechecked 6-8 weeks after any dose change |
| Thyroid ultrasound | Do once to assess gland volume and echogenicity | A near-normal volume with mild changes has better prognosis than a small atrophic gland |
| Long term | If Anti-TPO falls significantly and TSH stays normal on low/no dose - carefully attempt supervised discontinuation | Never stop abruptly or without monitoring |
The Honest Message for the Patient
"The tablet replaces what your thyroid is no longer making - it is not a drug that treats the disease itself. For most people with Hashimoto's, the thyroid makes progressively less hormone over the years, which means the tablet becomes more necessary with time, not less. About 1 in 10 patients do see their thyroid recover, but we cannot predict this at the start. What we can do is check your thyroid function every year, and if your TSH ever normalizes on a very small dose, we can try - carefully and under supervision - to reduce or stop the tablet. Right now, at age 20 with these results, the tablet is protecting your brain, heart, and reproductive health. It is a very safe medication and does not cause side effects when the dose is right."