SIMPLE WAY TO UNDERSTAND MI IN ECG
Reading File
Finding Sources
Finding Sources
Searching Images
myocardial infarction ECG changes ST elevation Q wave
Finding Sources
Searching Images
ECG localization myocardial infarction territory leads coronary artery
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive textbook content and real ECG images. Let me compile the complete, well-illustrated answer.
MI on ECG — Simple Way to Understand
🫀 Why the ECG Changes in MI
When a coronary artery is blocked, myocardial cells go through three zones:
- Ischemia (outer zone) → T-wave changes
- Injury (middle zone) → ST changes
- Necrosis (inner zone) → Q-wave changes
Each zone produces a characteristic ECG change, and they evolve over time.
📊 The Three Key ECG Changes
| Change | What it Means | Timing |
|---|---|---|
| Hyperacute T waves (tall, peaked T) | Very early ischemia | Minutes |
| ST elevation (convex "tombstone") | Acute transmural injury | Hours |
| Pathological Q waves | Myocardial necrosis (permanent scar) | Hours–days |
| T-wave inversion | Evolving/post-infarction ischemia | Days–weeks |
| ST normalizes | Infarct stabilizing | Days |
Pathological Q wave criteria: width ≥ 0.04 s (1 small square) and depth ≥ 25% of the R-wave height.
⏱️ ECG Evolution Over Time (STEMI)
Minutes: Hyperacute T waves (tall, broad, peaked)
Hours: ST elevation appears — "tombstone" morphology
Reciprocal ST depression in opposite leads
Hours–Day: Q waves develop (necrosis)
Days: T-wave inversion
Weeks: ST returns to baseline; Q waves may persist permanently
🗺️ STEMI Localization — Which Leads = Which Territory
This is the most clinically important part:
| Territory | Leads with ST Elevation | Culprit Artery |
|---|---|---|
| Anterior | V1–V4 | LAD (Left Anterior Descending) |
| Anteroseptal | V1–V2 (±V3) | Proximal LAD |
| Anterolateral | V1–V6, I, aVL | Proximal LAD or LCx |
| Lateral | I, aVL | LCx or diagonal branch |
| Inferior | II, III, aVF | RCA (or LCx) |
| Inferolateral | II, III, aVF + V5–V6 | LCx |
| Posterior | Tall R in V1–V2 + ST depression V1–V3 | RCA or LCx |
| Right Ventricle | II, III, aVF + V3R–V6R (right-sided leads) | Proximal RCA |
Key tips to identify the culprit artery:
- ST elevation in III > II → Right Coronary Artery (RCA)
- ST elevation in I, aVL + ST depression V1–V3 → Left Circumflex (LCx)
- Elevation aVR > V1 → Left Anterior Descending (LAD) or left main
- ST elevation III > II + ST elevation V1 or V4R → Proximal RCA with RV involvement
(Source: Tintinalli's Emergency Medicine, Table 49-5)
🔄 Reciprocal Changes — The Mirror Image
When one wall is injured, the opposite leads show ST depression (mirror image). This confirms the ST elevation is real infarction, not artifact:
- Inferior STEMI (II, III, aVF) → Reciprocal depression in I, aVL
- Anterior STEMI (V1–V4) → Reciprocal depression in inferior leads
- Posterior MI → No ST elevation in standard leads; shows tall R + ST depression in V1–V3
📋 STEMI Diagnostic Criteria (Standard)
-
≥ 2 contiguous leads with:
- V2–V3: ≥ 2.5 mm in men <40 yrs; ≥ 2 mm in men ≥40 yrs; ≥ 1.5 mm in women
- All other leads: ≥ 1 mm
-
New LBBB + chest pain = treat as STEMI equivalent
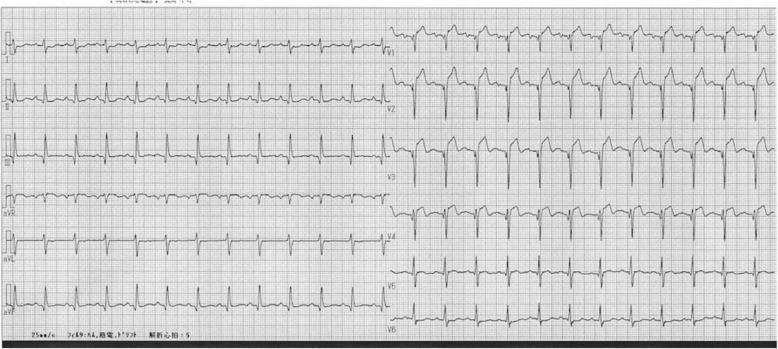
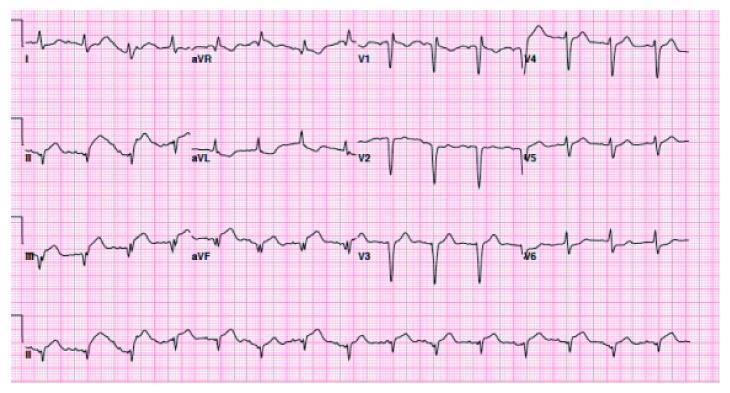
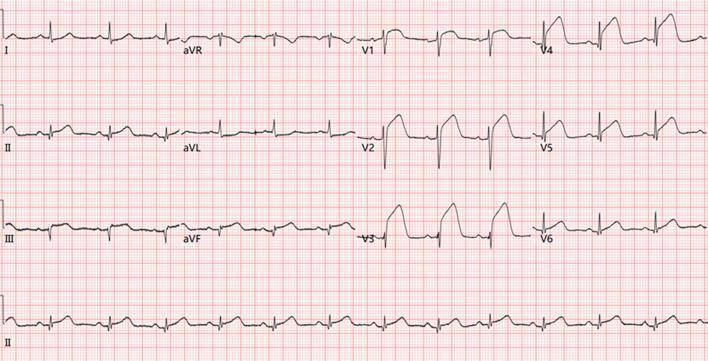
🖼️ Real ECG Examples
Anterior STEMI (LAD occlusion) — Tombstone morphology V2–V4
Inferior STEMI (RCA occlusion) — Classic pattern
Extensive STEMI — Multi-territory involvement
🧠 Quick Memory Aid: "STEMI in a NUTSHELL"
S — ST elevation (convex, upward)
T — Tombstone shape = bad sign
E — Elevation in ≥2 contiguous leads
M — Mirror image (reciprocal depression)
I — Identify territory → coronary artery
Then later...
Q — Q waves form (necrosis)
I — Inversion of T waves (evolving)
⚠️ STEMI Mimics (Don't Miss These)
| Condition | Clue to Distinguish |
|---|---|
| Early repolarization | Notched J point, concave ST, young athlete |
| Pericarditis | Diffuse ST elevation all leads, PR depression, saddle-shaped |
| LBBB (old) | Apply Sgarbossa criteria |
| LVH | ST elevation in V1–V2 with large QRS voltages |
| Brugada | Downsloping ST in V1–V2, right bundle pattern |
| Hyperkalemia | Peaked T waves, no chest pain, wide QRS |
Summary Flow
Chest pain + ECG
↓
ST elevation in ≥2 contiguous leads?
↓ YES
Identify territory (table above)
↓
Look for reciprocal depression (confirms it)
↓
Activate cath lab → PCI within 90 min (door-to-balloon)
(Sources: Tintinalli's Emergency Medicine — STEMI chapter; Goldman-Cecil Medicine)
This is a shared conversation. Sign in to Orris to start your own chat.