Hello teach me something abt medical today
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here's your medical lesson for today! 🫀
Today's Topic: The Cardiac Action Potential
This is one of the most fundamental concepts in cardiology - it explains how every single heartbeat is electrically generated and controlled.
What Is a Cardiac Action Potential?
A cardiac action potential (AP) is the rapid change in electrical voltage across the membrane of a heart muscle cell that triggers it to contract. Think of it as the "electrical spark" behind every heartbeat.
At rest, most cardiac cells sit at a resting membrane potential of -80 to -90 mV (negatively charged inside relative to outside). The SA node and AV node are exceptions, sitting at around -50 to -65 mV - which is why they can fire spontaneously.
The 5 Phases (Phases 0-4)
| Phase | Name | Ion Responsible | What Happens |
|---|---|---|---|
| 0 | Rapid Depolarization | Na+ rush IN | Voltage spikes from -90mV to +30mV - this is the "upstroke" |
| 1 | Initial Repolarization | K+ brief OUT | Slight dip just after peak |
| 2 | Plateau | Ca2+ IN, K+ slow OUT | Voltage held steady for ~200ms - Ca2+ entry triggers contraction |
| 3 | Rapid Repolarization | K+ rapid OUT | Cell returns to resting -90mV |
| 4 | Resting / Pacemaker | K+ (IK1) at rest | Stable in ventricular cells; slow depolarization in SA/AV node |
The plateau phase (Phase 2) is unique to cardiac cells - skeletal muscle and nerves don't have it. It is what makes the cardiac refractory period so long (~200ms), which prevents the heart from going into tetanic (sustained) contraction like a skeletal muscle would.
How It Spreads Through the Heart
Here is the conduction diagram from Costanzo Physiology:
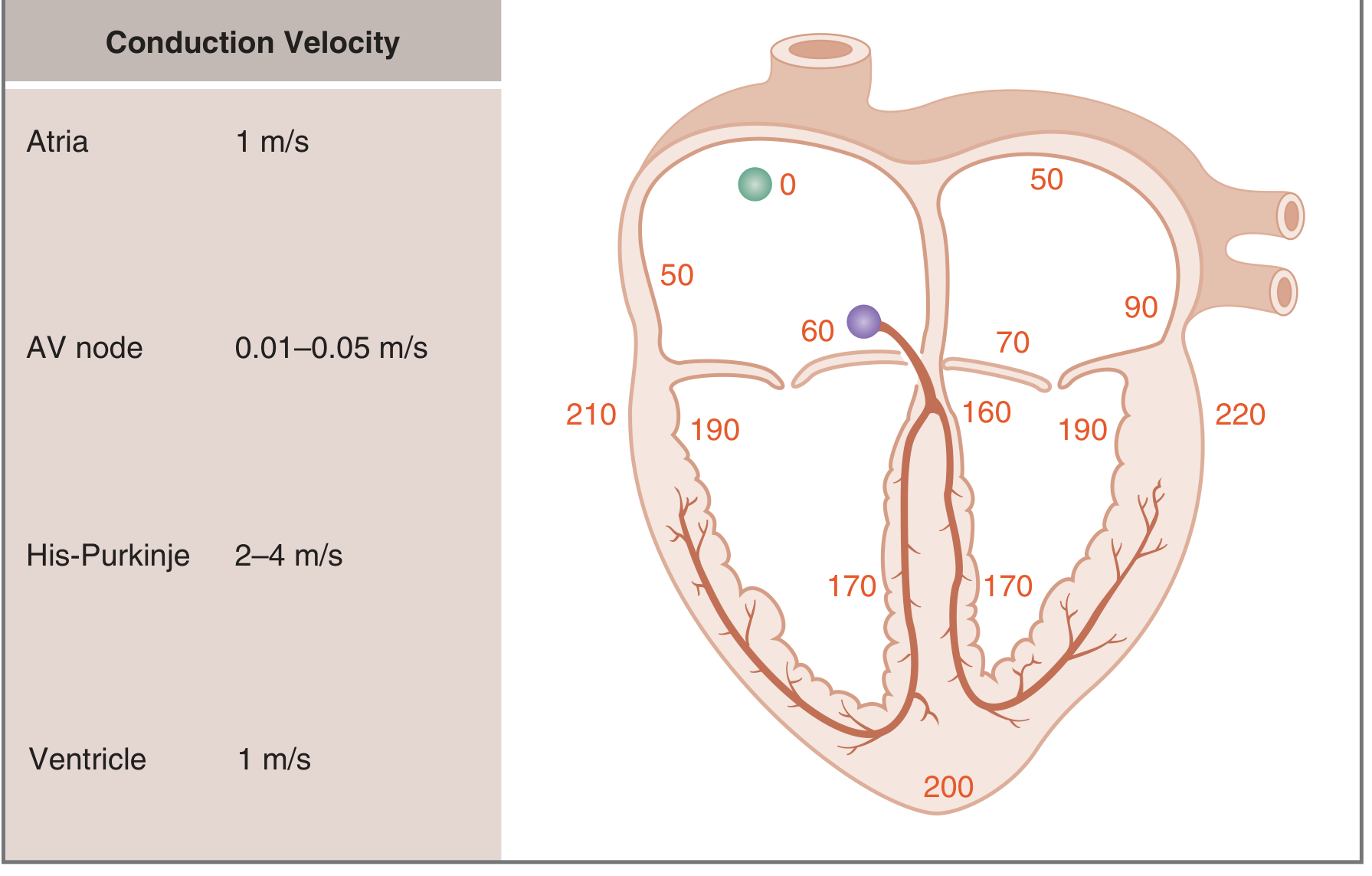
The signal travels from the SA node (time = 0) and reaches the farthest part of the ventricles at ~220 ms. Notice the key conduction velocities:
- SA node fires first (it's the natural pacemaker at ~60-100 bpm)
- Atria: 1 m/s - fast enough to contract the atria together
- AV node: only 0.01-0.05 m/s - the slowest! This deliberate AV delay (~100ms) ensures the ventricles don't fire until the atria have finished filling them
- His-Purkinje system: 2-4 m/s - the fastest! This ensures both ventricles activate almost simultaneously for efficient ejection
The Ion Channels and Genes Behind Each Phase
This diagram from Goodman & Gilman's Pharmacology shows every current and the gene that encodes it:
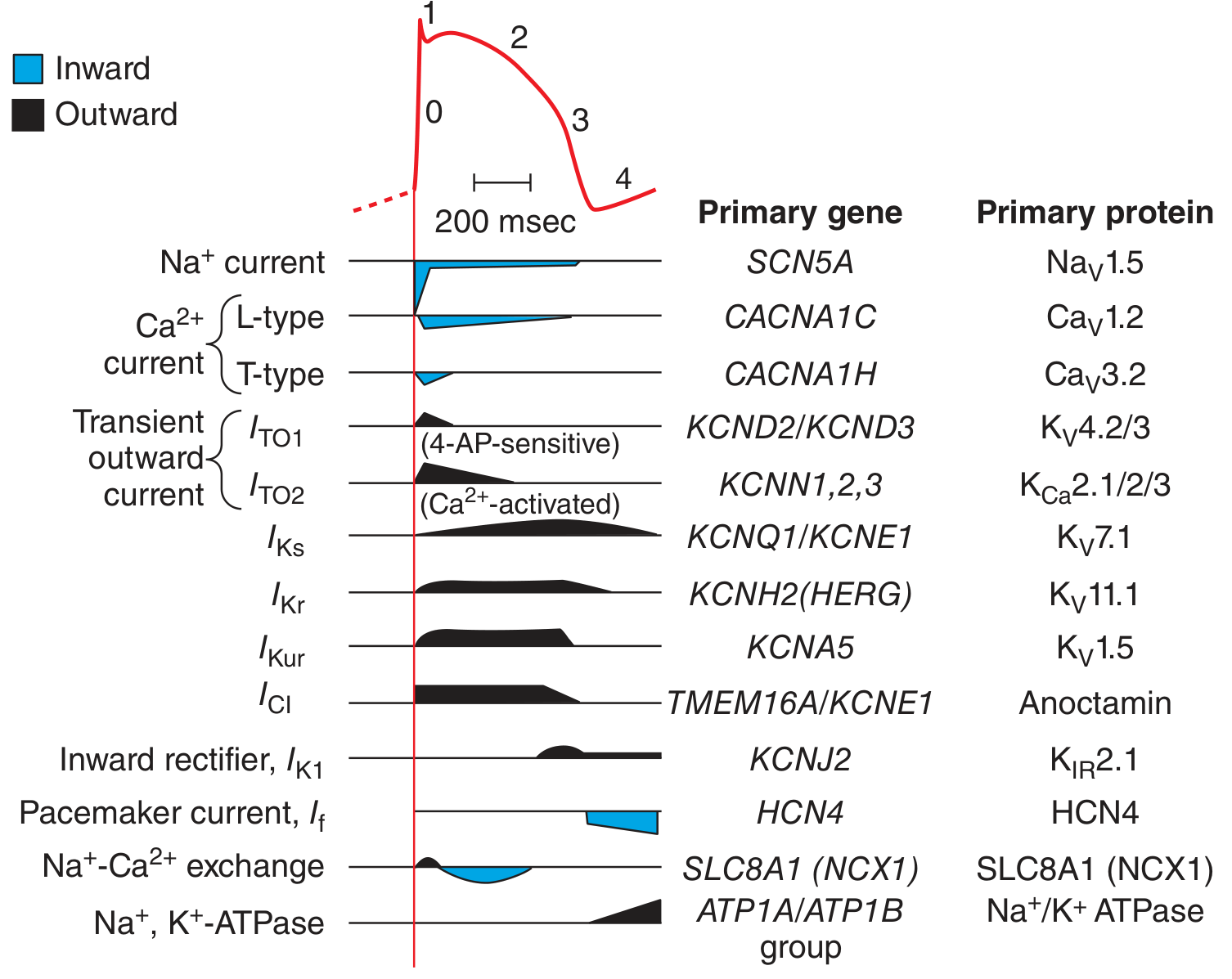
Key channels to know:
- SCN5A / Na_V1.5 - the main fast Na+ channel (Phase 0). Mutations cause Brugada syndrome and Long QT Type 3.
- CACNA1C / Ca_V1.2 - the L-type Ca2+ channel (Phase 2 plateau). Blocked by calcium channel blockers like verapamil and diltiazem.
- KCNH2 (HERG) / K_V11.1 - the rapid delayed rectifier K+ current (I_Kr). This is the infamous channel blocked by many drugs causing Long QT syndrome.
- HCN4 - the pacemaker current (I_f, "funny current") in the SA node. Blocked by ivabradine to slow heart rate.
Why This Matters Clinically
Understanding action potential phases directly explains how antiarrhythmic drugs work (Vaughan-Williams classification):
- Class I (lidocaine, flecainide) - block Na+ channels (Phase 0) → slow conduction
- Class II (beta-blockers) - reduce pacemaker firing (Phase 4) → slow heart rate
- Class III (amiodarone, sotalol) - block K+ channels (Phase 3) → prolong refractory period
- Class IV (verapamil, diltiazem) - block Ca2+ channels (Phase 2) → slow AV node conduction
A prolonged Phase 2-3 (long QT interval on ECG) is dangerous because the ventricle stays depolarized longer, creating a window where early afterdepolarizations can trigger Torsades de Pointes, a potentially fatal arrhythmia.
Sources: Braunwald's Heart Disease, Goodman & Gilman's Pharmacological Basis of Therapeutics, Costanzo Physiology 7th Edition
Want me to go deeper on any part of this - like pacemaker vs non-pacemaker cells, specific antiarrhythmics, Long QT syndrome, or something completely different? 😊
Make a quiz on this
🫀 Cardiac Action Potential Quiz
Test your knowledge! Try answering before you peek at the answers.
Q1. What is the resting membrane potential of a typical ventricular myocyte?
- A) 0 mV
- B) -40 mV
- C) -80 to -90 mV
- D) +30 mV
👉 Click to reveal answer
✅ C) -80 to -90 mV
Ventricular (and atrial/Purkinje) cells rest at -80 to -90 mV. The SA and AV nodes are less negative (-50 to -65 mV), which allows them to depolarize spontaneously.
Q2. During Phase 0 (rapid depolarization), which ion rushes INTO the cell?
- A) K+
- B) Ca2+
- C) Cl-
- D) Na+
👉 Click to reveal answer
✅ D) Na+
A massive inward Na+ surge through Na_V1.5 (encoded by SCN5A) drives the rapid upstroke from -90mV to about +30mV. This is the fastest phase of the action potential.
Q3. Which phase is UNIQUE to cardiac muscle (not found in skeletal muscle or nerves)?
- A) Phase 0 - rapid depolarization
- B) Phase 2 - the plateau
- C) Phase 3 - rapid repolarization
- D) Phase 4 - resting potential
👉 Click to reveal answer
✅ B) Phase 2 - the plateau
The plateau is sustained by Ca2+ flowing in (via L-type channels) balancing K+ flowing out. It lasts ~200ms and is what gives the heart its long refractory period, preventing tetanic contraction.
Q4. The AV node has the SLOWEST conduction velocity in the heart (0.01-0.05 m/s). What is the physiological purpose of this delay?
- A) To increase the force of ventricular contraction
- B) To allow the atria to finish filling the ventricles before they contract
- C) To prevent the SA node from firing too fast
- D) To increase blood pressure
👉 Click to reveal answer
✅ B) To allow the atria to finish filling the ventricles before they contract
The ~100ms AV delay accounts for nearly half of the total conduction time. Without it, the ventricles would fire before they're fully filled, drastically reducing cardiac output.
Q5. A patient is prescribed verapamil for their arrhythmia. Which ion channel does verapamil primarily block, and which phase does it affect?
- A) Na+ channel - Phase 0
- B) K+ channel - Phase 3
- C) L-type Ca2+ channel - Phase 2
- D) HCN channel - Phase 4
👉 Click to reveal answer
✅ C) L-type Ca2+ channel - Phase 2
Verapamil is a Class IV antiarrhythmic. It blocks Ca_V1.2 (L-type Ca2+ channels), slowing AV node conduction. This is why it's useful for rate control in atrial fibrillation/flutter.
Q6. Which gene encodes the "funny current" (I_f) pacemaker channel in the SA node? Which drug specifically blocks it?
- A) KCNH2 - blocked by amiodarone
- B) HCN4 - blocked by ivabradine
- C) SCN5A - blocked by lidocaine
- D) CACNA1C - blocked by diltiazem
👉 Click to reveal answer
✅ B) HCN4 - blocked by ivabradine
The HCN4 channel carries the I_f "funny" current that drives spontaneous Phase 4 depolarization in the SA node. Ivabradine selectively blocks it to reduce heart rate without affecting contractility - useful in heart failure and stable angina.
Q7. A drug blocks the KCNH2 (HERG) K+ channel. What is the expected ECG finding, and what dangerous arrhythmia can result?
- A) Shortened PR interval → WPW syndrome
- B) Prolonged QRS → bundle branch block
- C) Prolonged QT interval → Torsades de Pointes
- D) ST elevation → STEMI
👉 Click to reveal answer
✅ C) Prolonged QT interval → Torsades de Pointes
HERG encodes the I_Kr rapid delayed rectifier K+ channel (Phase 3). Blocking it delays repolarization → long QT on ECG → risk of early afterdepolarizations → Torsades de Pointes, which can degenerate into ventricular fibrillation. This is why so many drugs are screened for HERG channel activity.
Q8. Rank these cardiac structures from SLOWEST to FASTEST conduction velocity:
His-Purkinje fibers / AV node / Atria / Ventricles
👉 Click to reveal answer
✅ AV node (0.01-0.05 m/s) → Atria (1 m/s) = Ventricles (1 m/s) → His-Purkinje (2-4 m/s)
The Purkinje system is the fastest - it needs to activate both ventricles almost simultaneously so they contract as a unit for maximum efficiency.
🏆 Score Yourself
| Score | Result |
|---|---|
| 8/8 | Cardiologist material! |
| 6-7/8 | Solid understanding |
| 4-5/8 | Good foundation, review the phases |
| <4/8 | Re-read the lesson and try again! |
Want a harder round with clinical scenarios (e.g. ECG findings, drug interactions, channelopathies), or shall we move on to a new medical topic?
This is a shared conversation. Sign in to Orris to start your own chat.